Page 8 of 23
IM10.9-11 | Renal Failure Clinical Evaluation — SDL Guide (Part 2)
Interpretation of Clinical Findings
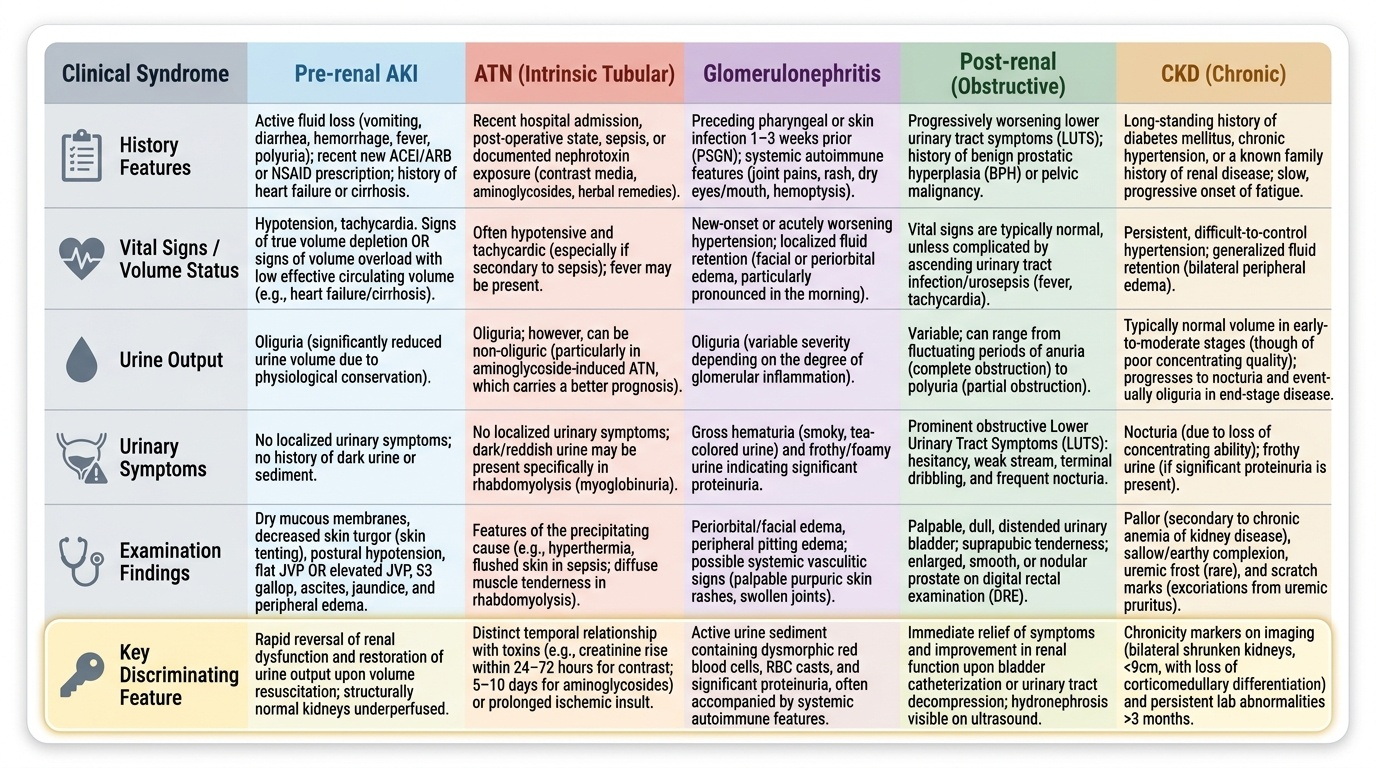
The physical signs elicited in the history and examination do not carry diagnostic weight individually — they must be interpreted as a pattern that maps onto one of the clinical categories. This interpretive step, which bridges the bedside examination and the differential diagnosis, is the skill assessed by IM10.10 and IM10.11. The key clinical syndromes in renal failure each have a characteristic finding constellation.
Provided image
Pre-renal AKI pattern: Symptoms of fluid loss (vomiting, diarrhoea, haemorrhage, fever, polyuria from uncontrolled diabetes), recent new ACEI/ARB or NSAID prescription, or history of heart failure/cirrhosis (effective volume depletion despite total body excess). Examination: volume depletion signs (dry mucous membranes, tenting skin, postural hypotension, tachycardia, flat JVP) OR volume overload signs with low effective circulating volume (elevated JVP, oedema, S3 gallop in heart failure; ascites, caput medusae, jaundice in cirrhosis). No urinary symptoms, no uraemic signs (in early pre-renal), no urinary casts by history. The kidneys are functioning correctly — they are being underperfused.
ATN pattern (intrinsic — tubular): Recent hospital admission, post-operative state, sepsis, nephrotoxin exposure (documented antibiotic use, contrast, herbal). Examination may show features of the precipitating illness (sepsis — fever, hypotension, tachycardia; rhabdomyolysis — muscle tenderness, dark urine). No urinary symptoms. Urine output may be reduced but can be non-oliguric in aminoglycoside ATN (non-oliguric ATN has a better prognosis). History of the appropriate temporal relationship between nephrotoxin exposure and creatinine rise (aminoglycosides: rises 5–10 days into a course; contrast: rises within 24–72 hours).
Glomerulonephritis pattern: Haematuria noticed by patient (smoky, tea-coloured urine), frothy urine (proteinuria), facial or periorbital oedema (often more pronounced in the morning — lymphatic drainage position effect), hypertension of recent onset, preceding pharyngeal or skin infection 1–3 weeks ago (post-streptococcal GN), or systemic features (joint pains, rash, dry eyes/mouth — suggesting lupus or Sjögren's, haemoptysis — Goodpasture's or GPA vasculitis).
Post-renal pattern: Lower urinary tract symptoms (LUTS) — hesitancy, poor stream, terminal dribbling, nocturia (classic BPH history in an elderly man); or history of pelvic malignancy, retroperitoneal pathology, bilateral renal calculi. Examination hallmark: palpable or percussible distended bladder in complete obstruction. Bilateral flank tenderness (hydronephrotic kidneys, if distended). Note: AKI from bilateral ureteric obstruction without bladder obstruction may have no lower urinary symptoms.
CKD pattern: Long history of diabetes or hypertension, prior creatinine results showing gradual rise, long-standing nocturia, fatigue, pruritus, and restless legs. Examination: small palpable kidneys (by percussion — loss of normal renal dullness), anaemic appearance, uraemic complexion (sallow), possible peripheral neuropathy, hypertension. Normal or mildly raised creatinine was documented in the past.
Applied Practice — Clinical Decision-Making at the Bedside
The clinical evaluation leads directly to the bedside management decision. Before any investigations are dispatched, three immediate decisions are made based on history and examination alone, and the clinician who can make them confidently while awaiting investigation results is the clinician who prevents deterioration.
Decision 1 — Volume status and immediate fluid management. If the examination shows volume depletion (dry mouth, tachycardia, postural hypotension, flat JVP), begin isotonic crystalloid resuscitation and reassess response by urine output and JVP at 1-hour intervals. If the examination shows volume overload (elevated JVP, bibasal crepitations, pitting oedema), do NOT give further fluids — the patient needs diuresis or dialysis. If uncertain (euvolaemic patient with rising creatinine), proceed with investigations first. The clinical examination is the most actionable tool for this decision; a bedside ultrasound of the inferior vena cava (collapsibility with inspiration = volume-depleted) augments clinical assessment.
Decision 2 — Bladder catheterisation for suspected obstruction. If the examination reveals a distended bladder, acute urinary retention, or a history strongly suggesting bladder outlet obstruction (elderly man, BPH symptoms, anuria), insert a urethral catheter immediately — both as a therapeutic intervention and to monitor urine output. Do not wait for ultrasound if obstruction is clinically obvious.
Decision 3 — Hyperkalaemia urgency assessment. Based on known or expected cause and clinical context (oliguric ATN, CKD G4–G5, acidaemic patient), request an urgent ECG and potassium level simultaneously. If the patient has peaked T-waves, widened QRS, or clinical risk factors for dangerous hyperkalaemia, begin treatment (calcium gluconate for membrane stabilisation) before the formal potassium result arrives.
The clinical approach also generates a priority differential diagnosis list — a ranked list of probable causes with the most likely first and the most dangerous or treatable causes highlighted even if less likely. This list directly drives the investigation selection and determines urgency. For example: an elderly man with AKI and bilateral lower limb oedema and BPH history: differential priority = (1) obstructive uropathy from BPH [most likely, immediately treatable], (2) acute-on-CKD from volume depletion [check prior bloods], (3) cardiac failure with pre-renal AKI [check JVP, echo], (4) contrast nephropathy if recent contrast exposure. The differential is not a static list — it updates with every clinical finding and investigation result.
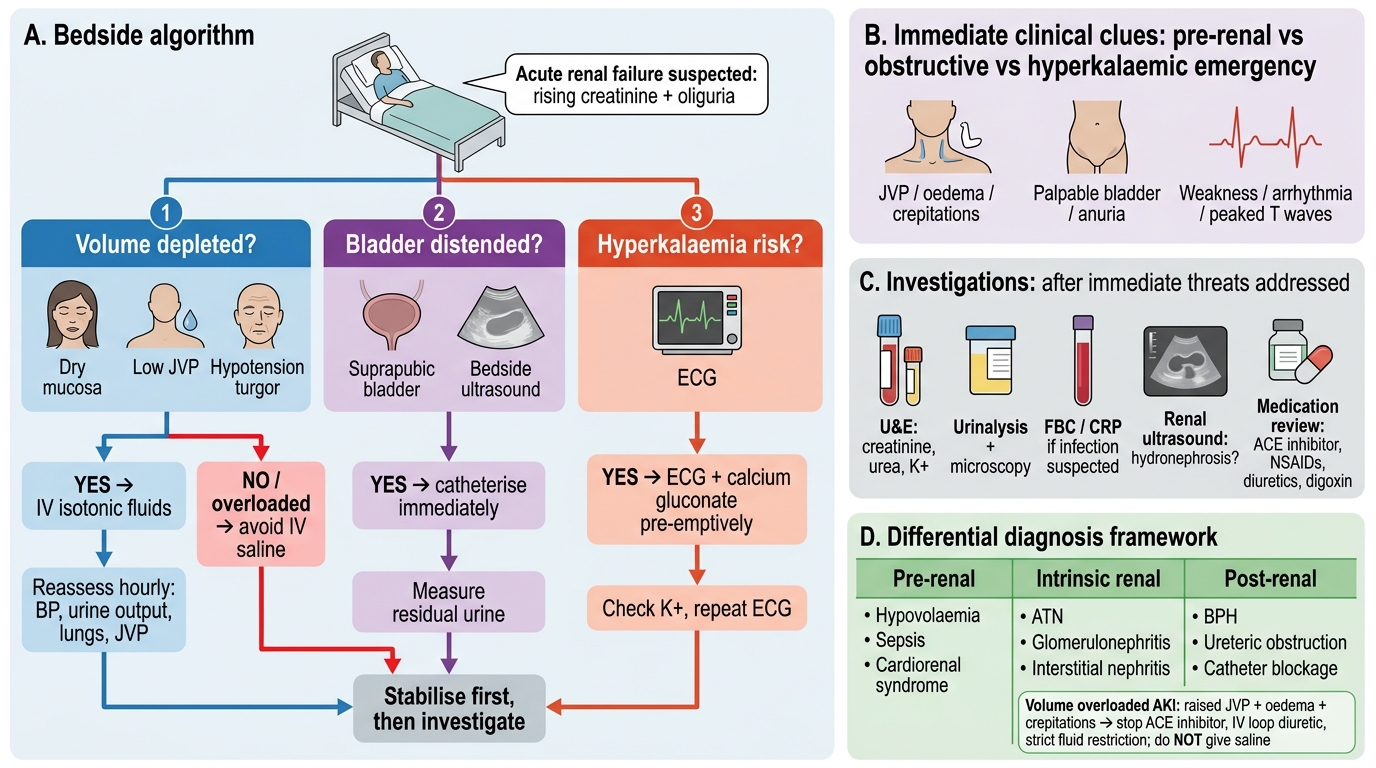
Bedside Decision Algorithm for Acute Renal Failure
SELF-CHECK
You examine a 72-year-old man with creatinine 4.2 mg/dL (baseline 1.3 mg/dL 6 months ago). His BP is 145/90 mmHg, JVP is elevated at 7 cm above sternal angle, he has 3+ pitting oedema bilaterally to the thigh, and bibasal fine crepitations. He has passed only 180 mL in the last 12 hours. He takes furosemide 40 mg/day, an ACE inhibitor, and digoxin. What is the MOST appropriate immediate management step?
A. Give IV normal saline 1 L over 1 hour
B. Stop the ACE inhibitor, increase furosemide to 80 mg IV, and strict fluid restriction
C. Insert a urethral catheter to relieve obstruction
D. Give calcium gluconate for presumed hyperkalaemia
Reveal Answer
Answer: B. Stop the ACE inhibitor, increase furosemide to 80 mg IV, and strict fluid restriction
This patient is volume-overloaded — elevated JVP, bilateral oedema, bibasal crepitations. The AKI is cardiorenal (reduced effective circulating volume from cardiac failure) rather than hypovolaemic. Giving IV saline would worsen pulmonary oedema and is absolutely contraindicated. The correct approach is to hold the ACE inhibitor (which reduces effective circulating volume and intraglomerular pressure, worsening the AKI), increase the diuretic dose (IV furosemide for better bioavailability in fluid-overloaded state), and restrict fluid intake. A urethral catheter is not indicated (no obstruction signs). Calcium gluconate may be needed if hyperkalaemia confirmed, but this is not the immediate priority before the potassium result.
CLINICAL PEARL
The JVP assessment is the single most underused and most impactful physical sign in renal failure evaluation. Many clinicians skip it or perform it incorrectly — positioning the patient flat or at 90° rather than the correct 45°, or failing to distinguish the venous pulsation from the carotid. The JVP is the bedside surrogate for right atrial pressure and hence for the entire cardiac filling pressure. A patient with AKI who is volume-depleted will have a flat, barely visible JVP — this is a signal to give fluids confidently. A patient with AKI and a JVP elevated at 8 cm above the sternal angle has cardiac failure or nephrotic syndrome — this is an absolute contraindication to fluid resuscitation. Getting this right at the bedside, before any investigations, prevents the most common management errors in AKI: fluid loading the volume-overloaded patient and withholding fluids from the volume-depleted one.
Self-Assessment — Clinical Evaluation Scenarios
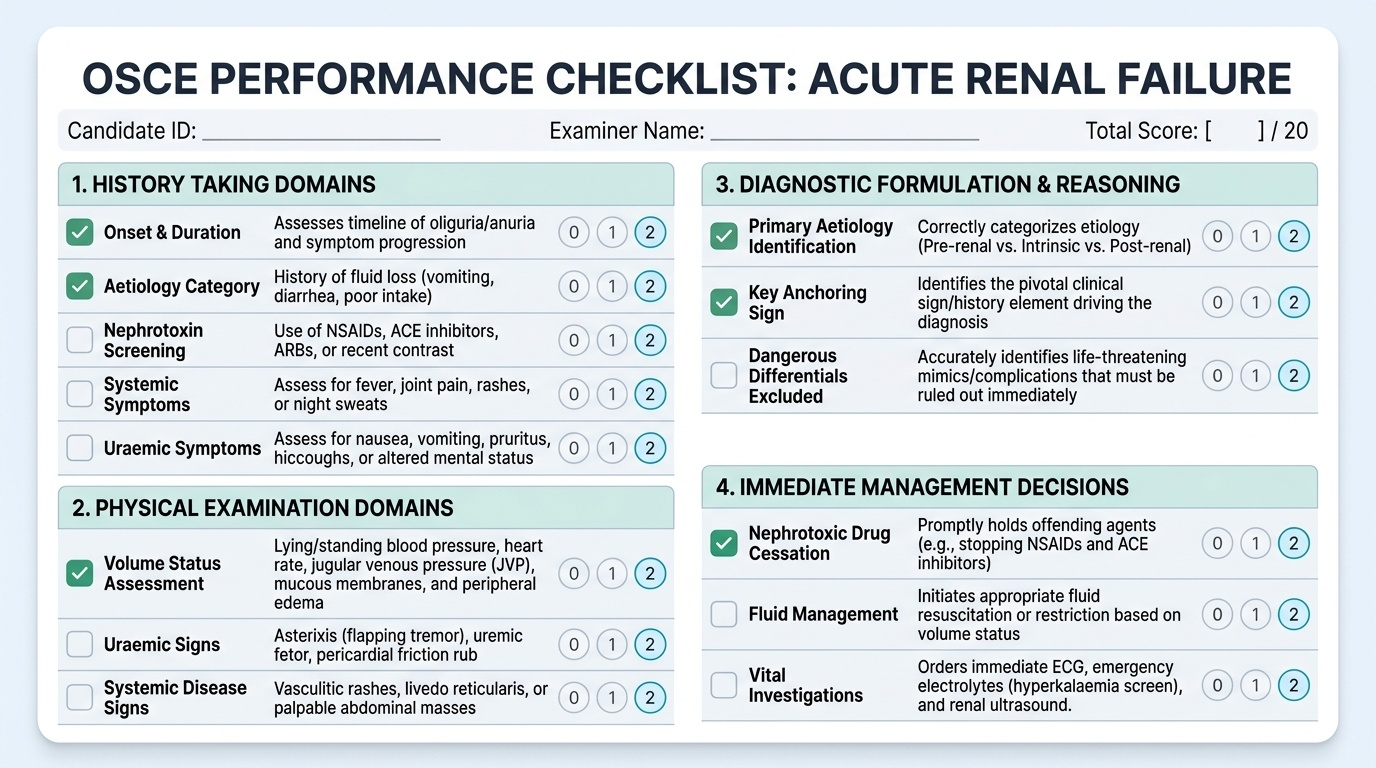
The self-assessment below presents three clinical evaluation vignettes that span the range of presentations tested in the IM10.9–10.11 competency domain. For each scenario, you are asked to: (1) identify the most likely aetiology category, (2) state the key history element or physical sign that anchors your diagnosis, and (3) identify the most dangerous differential that must be excluded. Work through your reasoning before reading the analysis. The scenarios are designed to test pattern recognition under time pressure, mirroring the real clinical encounter where the differential must be generated before the investigations are ordered — because the investigation order itself depends on the differential. In examinations at the final-year level, viva examiners consistently probe for the ability to generate a prioritised differential from clinical findings alone, not simply to list every possible cause of AKI.
Provided image
Scenario A: A 45-year-old man presents with 3 days of vomiting, inability to keep down fluids, and reduced urine for 2 days. He is a known hypertensive on perindopril and ibuprofen (self-prescribed for back pain). On examination: pulse 104/min, BP 94/60 mmHg lying, 78/52 sitting. Mucous membranes dry. JVP not visible. No peripheral oedema. Abdomen soft. Creatinine: 3.1 mg/dL (baseline 1.0).
Analysis: (1) Pre-renal AKI from combined vomiting-induced volume depletion AND nephrotoxic drug contribution (ibuprofen blocks prostaglandin-mediated afferent arteriolar dilation; perindopril reduces efferent arteriolar tone). Both drugs should be stopped immediately. (2) Anchoring sign: postural hypotension, tachycardia, invisible JVP = definite volume depletion. (3) Most dangerous differential to exclude: intrinsic AKI from ATN if the hypotension is prolonged — check for granular casts on urinalysis; if present, ATN has already supervened and recovery may take weeks, not hours.
Scenario B: A 38-year-old woman is referred with creatinine 2.8 mg/dL discovered on routine testing. She has no symptoms. BP is 168/102 mmHg. On examination: bilateral periorbital puffiness, 2+ pitting oedema of ankles. Urine dipstick: 3+ protein, 2+ blood. The GP reports no prior creatinine measurement available.
Analysis: (1) Acute glomerulonephritis — new hypertension, haematuria, and nephrotic-range proteinuria in a young woman with periorbital oedema. Most likely diagnosis: lupus nephritis (age, sex; ask for malar rash, joint pains, photosensitivity) or IgA nephropathy. (2) Anchoring finding: haematuria + heavy proteinuria together on dipstick = glomerulonephritis signature. (3) Most dangerous differential: rapidly progressive glomerulonephritis (RPGN) — requires urgent renal biopsy and immunosuppression; missing this can result in permanent renal failure within weeks.
Scenario C: A 70-year-old man with type 2 diabetes and BPH presents with confusion, nausea, and 24-hour anuria. Creatinine is 9.2 mg/dL. On abdominal examination: suprapubic dullness up to 5 cm above the symphysis pubis, tender on percussion, patient restless. JVP normal, no oedema.
Analysis: (1) Post-renal AKI from bladder outlet obstruction — complete urinary retention from BPH. (2) Anchoring sign: palpable and percussible bladder (suprapubic dullness), 24-hour anuria in a man with BPH. (3) Most dangerous differential: This creatinine of 9.2 mg/dL also raises the possibility of superimposed ATN from the prolonged obstruction; the confusion may represent uraemic encephalopathy. Immediate catheterisation is the first step — if creatinine does not improve within 48–72 hours after relief of obstruction, consider ATN from obstructive uropathy + underlying CKD from diabetes.