Page 16 of 23
IM10.23-24 | Renal Replacement Therapy Ethics and Quality of Life — SDL Guide
Learning Objectives
- Describe and communicate the ethical and legal issues involved in renal replacement therapy
- Recognise the impact of CKD on patient quality of life, wellbeing, work, and family, and incorporate patient preferences into CKD care
INSTRUCTIONS
This module addresses the human dimensions of kidney failure — the ethical frameworks governing RRT decisions, the legal structures that apply in India, and the patient-centred perspective of living with CKD. These competencies at the KH level require synthesis of medical knowledge with communication skills, ethical reasoning, and cultural awareness.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 308 — CKD: Ethical Issues in ESRD (textbook)
- API Textbook of Medicine, 10th ed., Ch. Nephrology — Ethical Aspects of Renal Replacement Therapy (textbook)
- Transplantation of Human Organs Act, India, 1994, amended 2011 (guideline)
- KDIGO 2012 CKD Guideline — Chapter on Preparation for Kidney Failure Treatment (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Gopalakrishnan is a 68-year-old retired government officer with ESRD from long-standing hypertensive nephropathy. He is intelligent, articulate, and deeply religious. His nephrologist has explained that haemodialysis three times a week is now medically necessary. But Gopalakrishnan sits in front of you with a quiet, resolute expression: 'Doctor, I have seen what dialysis does to people. My brother spent his last two years attached to a machine, unable to travel to see our grandchildren's births. I want to live my remaining years as I choose, not as a machine requires. I want to discuss stopping.' Now consider a second patient: Priya, a 42-year-old nurse with IgA nephropathy and ESRD, who has two teenage daughters. She wants everything possible done — aggressive dialysis, transplant listing, experimental therapies. She has heard about a living-unrelated donor. She knows someone who 'arranged' a commercial kidney. She does not understand why the system has rules about who can donate. Both patients have ESRD. Both have clear preferences. But the ethical and legal landscape in which you must support their decisions is complex, and the clinician who has not thought through these questions will be poorly equipped to help them well.
WHY THIS MATTERS
For the NMC competencies IM10.23 (KH) and IM10.24 (KH), final-year students must understand the ethical and legal framework governing RRT decisions in India, including the Transplantation of Human Organs Act, and must be able to recognise and incorporate patient quality-of-life considerations and preferences into the care plan. These competencies are assessed in long cases, vivas, and professionalism-focused written examinations. They require integration of bioethics principles, Indian legal frameworks, cultural sensitivity, and patient communication skills — a distinctive blend that goes beyond biomedical knowledge.
RECALL
Recall the four principles of biomedical ethics from your earlier studies: autonomy (the patient's right to make informed decisions about their own care), beneficence (the obligation to act in the patient's best interest), non-maleficence (the duty to avoid harm), and justice (fair allocation of healthcare resources). Recall also from the management module that the RRT modalities are IHD (intermittent haemodialysis), PD (peritoneal dialysis), CRRT (for acute/ICU settings), and kidney transplantation. And recall that ESRD imposes a lifetime commitment to treatment — dialysis three times a week for life, unless transplanted. The ethical issues arise precisely because this treatment burden is large, the choices are irreversible in some respects, and the patient's preferences may differ from what the clinician believes is medically optimal.
Clinical Indication — When Ethical and QoL Issues Arise in RRT
Ethical and quality-of-life considerations become clinically operative at specific decision points in the trajectory of CKD and ESRD management. Recognising these junctures — and initiating the appropriate conversations before a crisis forces the decision — is the defining characteristic of proactive, patient-centred renal care. The physician who waits until the patient is uraemic before discussing RRT options has failed in their responsibility to support autonomous decision-making.
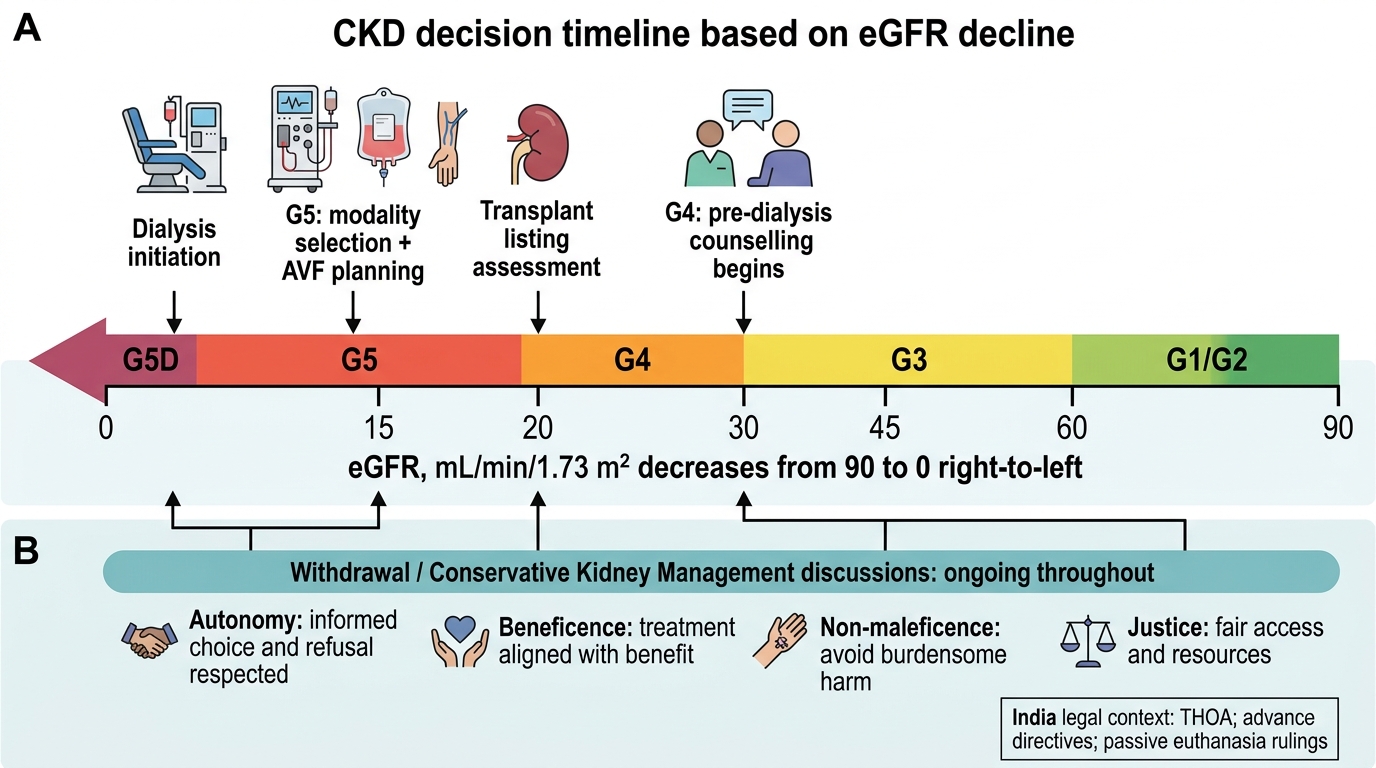
The key ethical decision points in the CKD-ESRD trajectory are: (1) Pre-dialysis counselling (ideally when eGFR reaches 15–20 mL/min, and no later than G4) — presentation of all RRT modality options (IHD, PD, home haemodialysis, transplant), each with honest information about burden, benefits, outcomes, and lifestyle implications; (2) Modality selection — the patient chooses a modality based on their values, lifestyle, home situation, and health status; this must be a genuine choice, not a physician-directed assignment; (3) Transplant candidacy assessment — who is eligible, what the waiting list means in practice, and the distinction between living-related, living-unrelated (authorised), and deceased-donor donation; (4) Withholding or withdrawing dialysis — when a patient refuses to start dialysis, requests withdrawal of ongoing dialysis, or when the clinician believes dialysis is medically futile; (5) End-of-life care — conservative kidney management (CKM) as an alternative to dialysis in elderly or frail patients who prioritise quality over quantity of life; and (6) Resource allocation decisions — when dialysis infrastructure is limited and access decisions must be made.
Each of these junctures requires the clinician to navigate the competing obligations of beneficence (doing good medically), autonomy (respecting the patient's right to refuse or choose), non-maleficence (avoiding treatments that prolong suffering without benefit), and justice (fair access to scarce resources). In the Indian context, these decisions are further shaped by family-centred decision-making, economic constraints, religious beliefs, and the legal framework of the Transplantation of Human Organs Act.
CKD Decision Timeline and Ethical Checkpoints
Governing Principles — Bioethics and Legal Framework in India
The ethical analysis of RRT decisions rests on the four principles of biomedical ethics and is enacted within the legal framework established by the Transplantation of Human Organs Act (THOA) of India.
The Four Principles of Biomedical Ethics (Beauchamp and Childress) applied to RRT:
Autonomy is the foundational principle in all RRT decisions. A capacitous adult patient has the right to accept or refuse any medical treatment, including dialysis, even if refusing will result in death. This right is legally enshrined in Indian law (following Supreme Court rulings including Aruna Shanbaug vs Union of India, 2011, and Common Cause vs Union of India, 2018, which recognised passive euthanasia and advance directives). Autonomy requires that the patient receives clear, honest, balanced information — not information shaped by the clinician's preferred modality — and that the decision is made free from coercion. A patient who is offered only haemodialysis without mention of peritoneal dialysis or conservative management has not been given a truly autonomous choice. For patients who lack decision-making capacity (uraemic encephalopathy, dementia, coma), a surrogate decision-maker (typically the nearest relative) acts in the patient's best interest, ideally guided by previously expressed wishes.
Beneficence requires that the clinician recommends the modality most likely to extend good-quality survival, prevent complications, and support the patient's life goals. The evidence base for RRT is generally positive — dialysis and transplantation extend life significantly compared to no treatment in ESRD. However, in very elderly, frail, or multimorbid patients, the evidence that dialysis significantly extends good-quality life is less compelling — several studies (including Germain et al. and the UK REIN registry) suggest that elderly patients with multiple comorbidities may have similar survival on conservative kidney management (CKM) compared to dialysis, with better quality of life (fewer hospital days, more time at home). In these patients, beneficence may support CKM rather than dialysis.
Non-maleficence requires the clinician to weigh the burdens of RRT — the time and effort of dialysis sessions, the risk of vascular access complications (infections, thrombosis), dietary restrictions, loss of employment, and psychological burden — against the benefits. For a patient with a predicted survival of 3–6 months on dialysis despite advanced age and multiple comorbidities, non-maleficence may argue against initiating dialysis. The concept of medical futility — a treatment is futile when it cannot achieve its intended physiological goal or when it can prolong only unconsciousness or a state from which the patient could never benefit — applies when dialysis would prolong dying without meaningful improvement in quality of life.
Justice in the context of RRT encompasses fair access to dialysis and transplantation, equitable allocation of deceased-donor organs, and the societal question of RRT funding. In India, haemodialysis is expensive (approximately Rs 1,000–2,000 per session × 3/week = Rs 12,000–24,000/month), creating profound inequity between patients who can afford it and those who cannot. Government schemes (PMJAY, various state health missions) provide partial coverage in some states. The National Organ and Tissue Transplant Organisation (NOTTO) coordinates deceased-donor organ allocation nationally, with regional ZTCCs (Zonal Transplant Coordination Committees) managing the waitlist. Allocation criteria include compatibility (blood group, HLA matching), time on waitlist, urgency, and paediatric priority — designed to be medically rational and equitable rather than based on wealth or social status.
The Transplantation of Human Organs Act (THOA), India 1994, amended 2011:
The THOA is the primary legislation governing organ donation and transplantation in India. Key provisions:
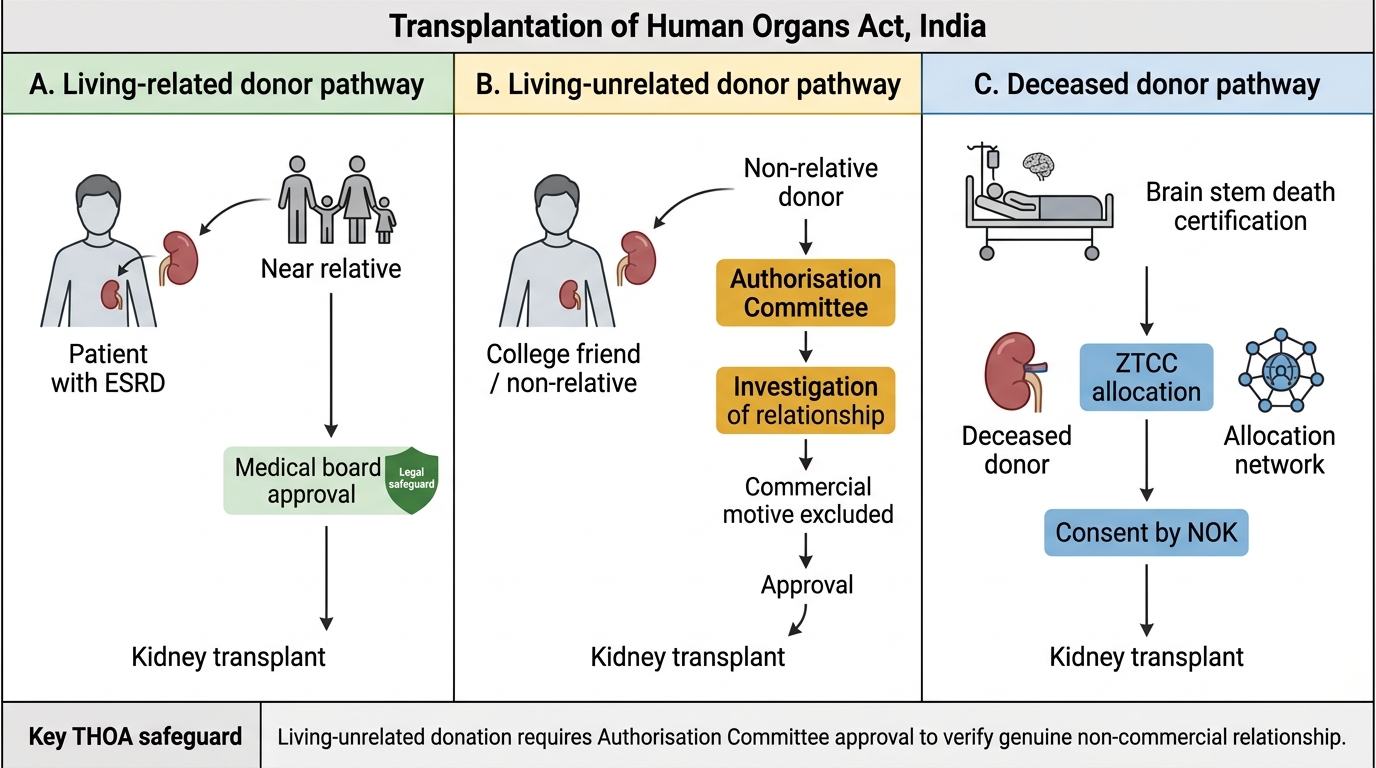
- Deceased-donor donation: Brain stem death (BSD) is legally recognised as death in India under THOA. BSD certification requires two physicians (at least one a specialist) who are not members of the transplant team. Following certification, organs may be harvested with consent of the next of kin and coordination through the ZTCC/NOTTO. The family cannot demand prolongation of ventilation for an objectively brain-dead patient, but they must consent to organ donation.
- Living-related donor: A donor who is a near relative (spouse, parents, children, siblings, grandparents, grandchildren) may donate a kidney after the hospital's medical board approval. No payment may be made. The donor must be informed of risks (operative risk ~0.1–0.3%, reduced life expectancy if single kidney fails) and the consent must be genuinely voluntary.
- Living-unrelated donor: A donor who is not a near relative (e.g., a friend) must obtain approval from the state-level Authorisation Committee (comprising medical, legal, and social work members), which investigates the genuineness of the relationship and excludes commercial motivation. This is the legal safeguard against commercial kidney trade.
- Prohibition of commercial dealing: The buying, selling, or brokering of human organs is a criminal offence under THOA — punishable by imprisonment up to 7–10 years and heavy fines. This prohibition applies to all parties: the donor, recipient, hospital, and broker. Priya's question about a 'commercial kidney' must be addressed directly: it is illegal, the vendor risks exploitation and long-term health consequences, and the purchased kidney may not be adequately matched or evaluated.
- Presumed consent vs opt-in: India currently uses an opt-in system — deceased-donor donation requires explicit consent. Several committees and expert groups have debated moving to opt-out ('presumed consent') to increase organ availability, but this has not yet been legislated nationally (Spain, UK, and other countries have adopted opt-out models).
THOA Kidney Donor Pathways
SELF-CHECK
A 45-year-old patient with ESRD wants to receive a kidney from his college friend who is willing to donate. The friend is not a blood relative. Under the Transplantation of Human Organs Act (India), what is the CORRECT legal pathway?
A. The friend may donate freely as a living unrelated donor after hospital consent forms are signed
B. The donation is not permitted as THOA only allows living-related donors
C. The friend must obtain approval from the state-level Authorisation Committee, which investigates the relationship and excludes commercial motivation
D. The friend may donate if the hospital's ethics committee approves, without state-level oversight
Reveal Answer
Answer: C. The friend must obtain approval from the state-level Authorisation Committee, which investigates the relationship and excludes commercial motivation
Under THOA, a living unrelated donor (not a near relative) must obtain approval from the state-level Authorisation Committee — a body comprising medical, legal, and social work members — which investigates the genuineness of the non-commercial relationship. This is the legal safeguard against commercial organ trafficking. Living-related donation requires hospital medical board approval but not the Authorisation Committee. Direct donation by a friend without Authorisation Committee approval is not legal under THOA. Hospital ethics committee approval alone is insufficient for living unrelated donation.
Procedure — Communicating Ethical Issues and Incorporating Patient Preferences
The procedural skill for IM10.23–10.24 is structured communication — the ability to navigate ethically complex conversations with empathy, clarity, and respect for the patient's values. These conversations differ from standard medical consultations in that the clinical facts alone do not determine the 'right answer'; the patient's values, preferences, goals, and lived experience are co-equal inputs to the decision. Communication failures in pre-dialysis counselling — providing only one option, using jargon the patient does not understand, holding the conversation only when the patient is already uraemic and cannot think clearly, or allowing the family to dominate when the patient has not authorised this — directly compromise patient autonomy and lead to decisions that do not reflect the patient's genuine preferences. The physician who is technically skilled in nephrology but poor at this conversation will impose dialysis on patients who would have preferred palliative care, or will fail to offer a patient the transplant route they would have chosen. Communication is therefore not a soft skill alongside medicine — it is the mechanism by which the ethical framework is enacted at the bedside.
The framework for pre-dialysis counselling (the core RRT conversation) follows a structured approach that should be rehearsed and internalised:
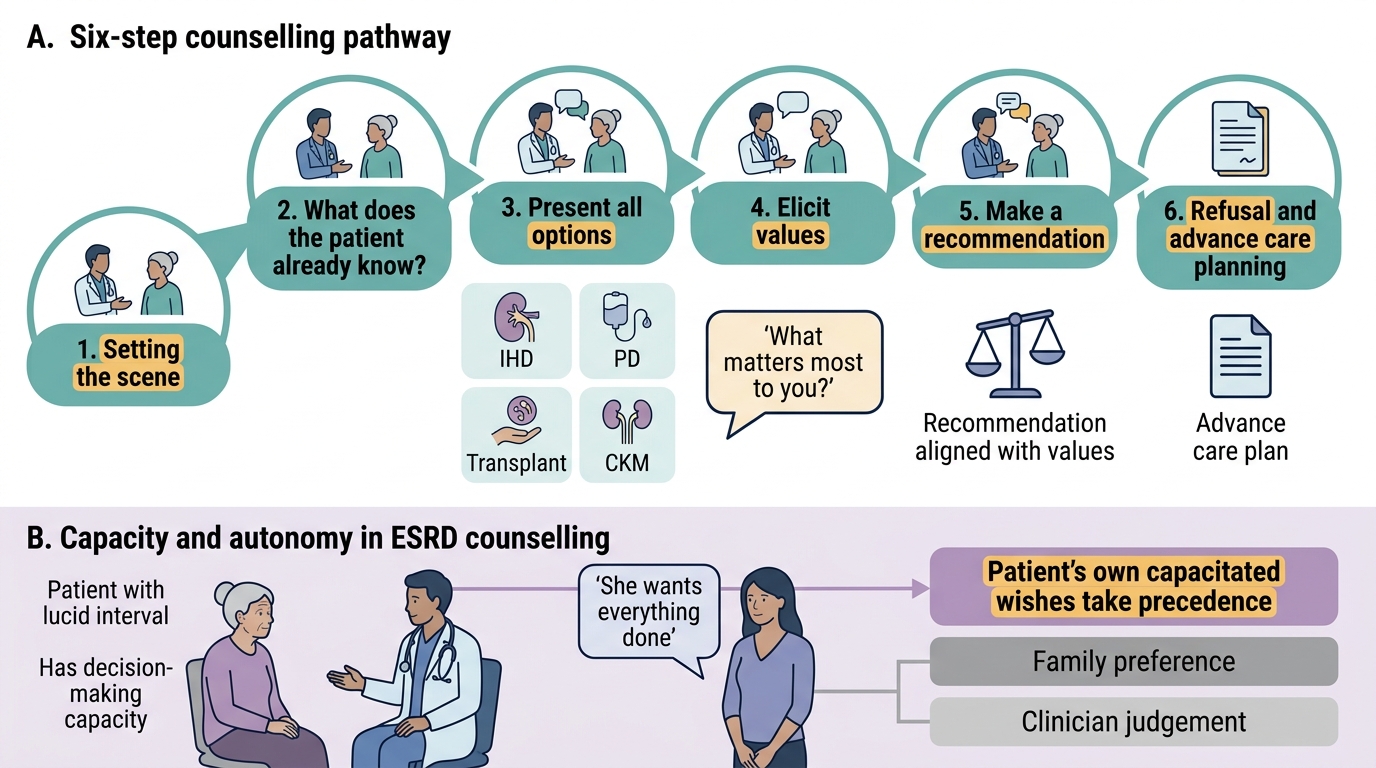
- Setting: Private space, adequate time (30–45 minutes minimum), family present if the patient wishes, interpreter if needed, no distractions. The consultation is not done at a bedside or in a corridor.
- Opening: Invite the patient to share what they already know and what concerns them most. 'Tell me what you understand about how your kidneys are doing.' 'What has been worrying you most about this?' This activates the patient's narrative and prevents the physician from making incorrect assumptions about the patient's knowledge level or emotional readiness.
- Information provision — balanced and complete: Present all realistic options: IHD (the hours, the frequency, the access procedure), PD (home-based, overnight, less restrictive), transplant (waiting list, living-donor options, eligibility criteria, realistic timelines in India — deceased-donor wait can be years), and conservative kidney management (CKM — treatment of symptoms and complications without dialysis, focusing on quality of remaining life). Present the outcomes for each option honestly but without catastrophising. Acknowledge uncertainty: 'No one can tell you exactly how long you will live on dialysis or on conservative management — but these are the ranges we typically see.'
- Elicit values and preferences: 'What matters most to you in your daily life?' 'How important is it to you to be able to travel / continue working / be present for your family?' 'Are there things you would not want to happen to you if your condition worsened — for example, being kept on machines if there were no chance of recovery?' These questions — structured around the patient's life goals rather than medical metrics — are the essence of patient-centred care in ESRD.
- Incorporate the response: The patient's values are folded into the recommendation. A patient who prioritises independence and travel may choose PD over IHD. A patient who is elderly and frail and values time at home over extended life may choose CKM. A patient who is young with good social support and a willing related donor should be discussed for early transplantation. The recommendation is then: 'Based on what you've told me, I think [option] would align best with your goals — but this is your decision, and I want you to take time to think about it and talk to your family.'
- Handling refusal of dialysis: A capacitous patient who refuses dialysis is exercising a legal right. The correct response is NOT to override the refusal, but to: ensure the patient understands the consequences (they will become increasingly uraemic and die without dialysis), check that the decision is based on adequate information and not on misconceptions or treatable depression, involve a palliative care team, and provide CKM with the goal of maximising comfort and quality of life. Document the conversation, the decision, and the patient's capacity in the notes. If capacity is doubtful, involve a psychiatrist and follow the hospital's mental capacity assessment protocol.
- Advance care planning: All patients with ESRD should be supported in creating an advance care plan — documenting their wishes for cardiopulmonary resuscitation, ventilatory support, and dialysis continuation in circumstances where they are no longer able to express preferences. The 2018 Supreme Court ruling in Common Cause vs Union of India has given legal recognition to advance directives in India — they are legally valid and must be honoured by treating physicians.
Pre-Dialysis Counselling: Six-Step Framework
SELF-CHECK
A 72-year-old woman with ESRD from diabetic nephropathy and multiple comorbidities (COPD, ischaemic heart disease, moderate dementia) is assessed for dialysis. Her daughter says she 'wants everything done.' The patient herself, when assessed during a lucid interval, says she 'doesn't want to be kept alive on machines.' Which principle takes precedence?
A. The daughter's wishes, as she is the next of kin and is legally the decision-maker
B. The physician's clinical judgement that dialysis would not be medically beneficial
C. The patient's own expressed wishes, as she has demonstrated capacity during a lucid interval
D. The hospital ethics committee decision, which overrides all individual preferences
Reveal Answer
Answer: C. The patient's own expressed wishes, as she has demonstrated capacity during a lucid interval
Autonomy is the foundational principle. A patient with dementia may have fluctuating capacity — during a lucid interval, if she demonstrates the ability to understand information, appreciate its relevance to her situation, reason about the options, and communicate a decision, she has decision-making capacity for that decision. Her expressed preference during a lucid interval has priority over the family's or physician's preferences. The daughter's wishes matter as a supportive resource but she is NOT the legal decision-maker when the patient herself has capacity. The physician's judgement about futility is relevant to the recommendation but does not override patient autonomy. The ethics committee provides guidance, not a binding override of patient preferences.