Page 17 of 23
IM10.23-24 | Renal Replacement Therapy Ethics and Quality of Life — SDL Guide (Part 2)
Interpretation — Understanding QoL Impact and Patient Experience
The impact of CKD and dialysis on quality of life is profound, multi-dimensional, and often under-appreciated by clinicians who see the patient for brief consultations and focus on laboratory parameters. IM10.24 specifically requires the physician to recognise this impact and to incorporate it into care planning — not as an afterthought but as a central clinical concern.
Physical dimensions of CKD-related QoL impairment: Even before dialysis, CKD impairs physical function through anaemia (fatigue, reduced exercise tolerance), peripheral neuropathy (pain, falls risk), uraemic pruritus (disturbed sleep, psychological distress), and fluid restriction (thirst, social difficulties at meals). Dialysis itself adds physical burden: the access procedure (surgery for AVF or PD catheter insertion), the fatigue that follows each session (post-dialysis fatigue affects approximately 70% of patients and may last 6–12 hours, severely limiting the day's activities), the dietary and fluid restrictions, and the risk of recurrent infections.
Psychological dimensions: Depression affects 20–30% of dialysis patients — significantly higher than the general population — driven by loss of autonomy, uncertainty about the future, repeated hospitalisations, and the chronic stress of a life-threatening illness managed by machine. Anxiety about vascular access failure, dialysis adequacy, and transplant prospects is nearly universal. Body image disruption is particularly significant in younger patients who undergo AVF creation (the visible, palpable 'thrill' of the fistula), PD catheter placement, or nephrectomy for a polycystic kidney. Cognitive impairment affects up to 40% of dialysis patients from cerebrovascular disease, uraemic effects, and chronic inflammation — this complicates consent processes, medication adherence, and self-management.
Social and occupational dimensions: In India, the burden of dialysis on family life is substantial because of the caregiver model of healthcare — a dialysis patient typically requires a family member to accompany them to sessions three times a week, impacting the caregiver's employment and wellbeing. Occupational impact is severe: patients on IHD three times per week have difficulty maintaining full-time employment (sessions consume 4–6 hours including travel), and many patients experience loss of income, occupational identity, and social role. PD offers greater flexibility and is often preferred by working-age patients. Many dialysis patients report feeling 'trapped' by their treatment schedule and unable to travel, attend social or religious events, or maintain family roles. Marital and sexual dysfunction (from uraemia, medication side effects, psychological factors, and body image changes) is common and rarely addressed by treating physicians.
Spiritual and existential dimensions: Many patients with ESRD, particularly in the Indian context, experience existential distress — questions about the meaning of their illness, the limits of medical treatment, and the approach of death. Religious and spiritual resources are central to coping for many patients; clinicians who engage with this dimension (asking about the patient's spiritual beliefs and resources without imposing their own) provide more holistic care. Gopalakrishnan's statement — 'I want to live my remaining years as I choose, not as a machine requires' — is precisely this kind of existential priority statement, and it deserves a clinical response that is far more than persuasion to start dialysis.
Incorporating patient preferences into care: Tools for systematically assessing patient preferences and QoL include validated questionnaires (KDQOL-SF: Kidney Disease Quality of Life Short Form, covering physical, mental, and kidney-disease-specific domains), structured goals-of-care conversations, and palliative care involvement for patients with advanced CKD or those considering CKM. A management plan that achieves excellent laboratory control while ignoring the patient's inability to work, maintain relationships, or sleep through the night is a medically successful but humanistically incomplete plan.
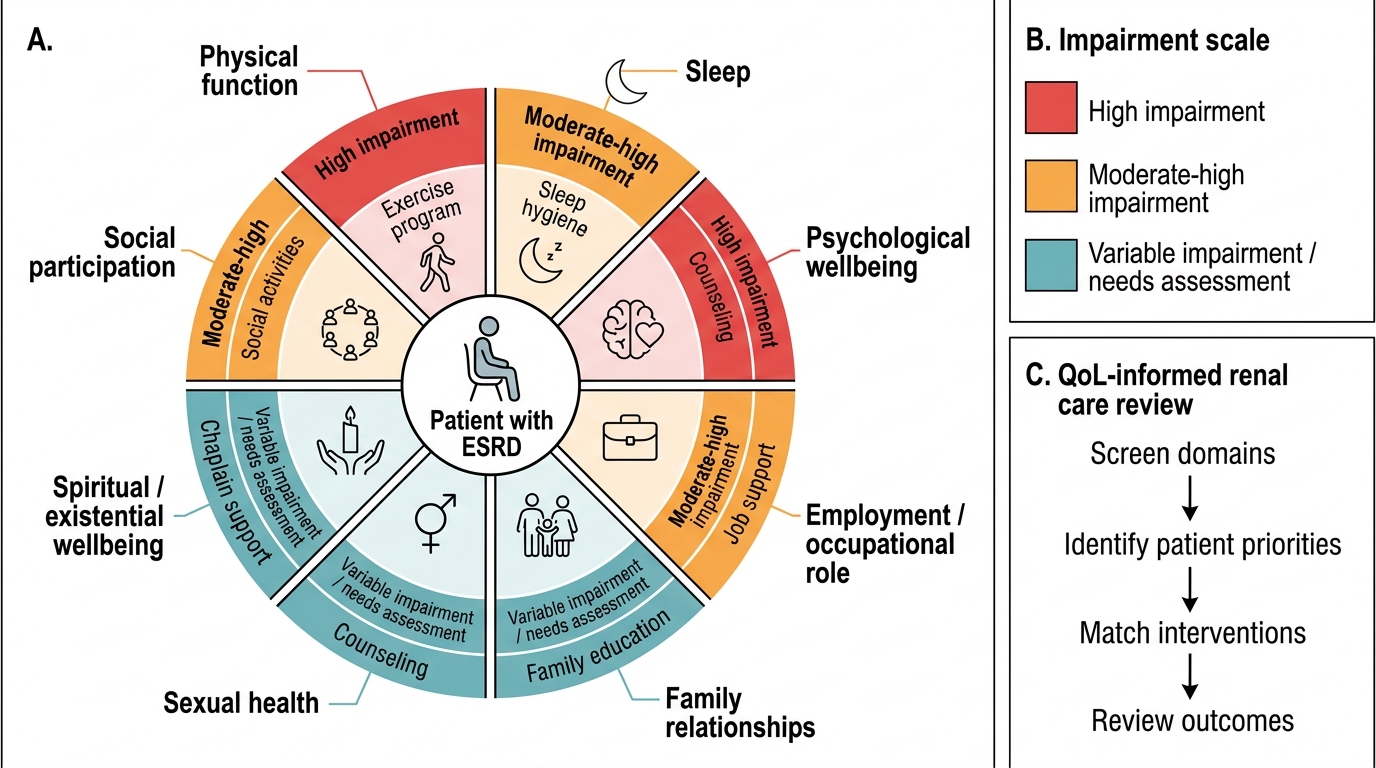
Quality-of-Life Domains in ESRD
Applied Practice — Ethics and QoL in Clinical Encounters
The applied skill in IM10.23–10.24 is the ability to identify and navigate ethically complex moments in the clinical encounter with a renal patient and to take a QoL-informed approach to care planning. Three applied practice areas are developed here: recognising and responding to commercial donation requests, navigating withdrawal of dialysis, and conducting a QoL-informed care planning review.
Responding to a request for commercial organ donation (Priya's scenario): When a patient reveals knowledge of or intention to pursue a commercial kidney purchase, the physician must respond without moralising but with clarity about the legal, medical, and ethical dimensions. Legal: commercial organ trading is a criminal offence under THOA (both donor and recipient may face prosecution). Medical: commercially obtained kidneys may not be adequately HLA-typed, donors may be medically unsuitable (unrecognised diabetes, hypertension, infections such as HIV or hepatitis B/C), and the post-operative follow-up for the donor may be absent — with life-threatening consequences. Ethical: the vendor (typically a poor, coerced individual) is being exploited; the power imbalance between a desperately ill patient willing to pay and a financially desperate potential donor undermines the voluntariness of the 'consent'. The clinical response is to: (1) acknowledge the patient's desperation and wish to live; (2) explain the legal, medical, and ethical concerns clearly; (3) redirect to the legitimate pathways (living-related donation through THOA, NOTTO waitlist for deceased-donor, assessment for peritoneal dialysis as a bridge); (4) document the conversation. The physician should not participate in facilitating a commercial transplant under any circumstances.
Navigating a request to withdraw dialysis (Gopalakrishnan's scenario): When a capacitous patient requests withdrawal of life-sustaining treatment, the clinical response must honour autonomy while ensuring the decision is informed and free from treatable causes. The steps are: (1) ensure the request is not driven by untreated depression, pain, or financial crisis — these are potentially reversible and should be addressed; (2) ensure the patient understands the trajectory without dialysis (increasing uraemia over days to weeks, ultimately fatal); (3) document the conversation and the patient's capacity; (4) involve a palliative care team who can provide symptom management and psychosocial support; (5) involve the family with the patient's consent (not to override the patient's decision but to support the family's adjustment); (6) continue all treatments that improve comfort while withdrawing dialysis. There is no ethical or legal obligation to continue dialysis in a capacitous patient who refuses it.
Conducting a QoL-informed care planning review: At every CKD clinic visit, in addition to reviewing laboratory parameters and medications, the clinician should briefly screen for QoL domains: 'How is your energy?' (anaemia, uraemia), 'How is your sleep?' (restless legs, pruritus, anxiety), 'Are you able to work?' (occupational function), 'How is your family managing?' (caregiver burden), 'Are there things you are no longer able to do that matter to you?' (social participation, religious practice). These brief inquiries take 2–3 minutes and reveal problems that blood tests cannot — they allow the clinician to identify untreated depression for referral, inadequate pain management for adjustment, or family crisis for social work involvement. QoL assessment is not a luxury but a clinical responsibility.
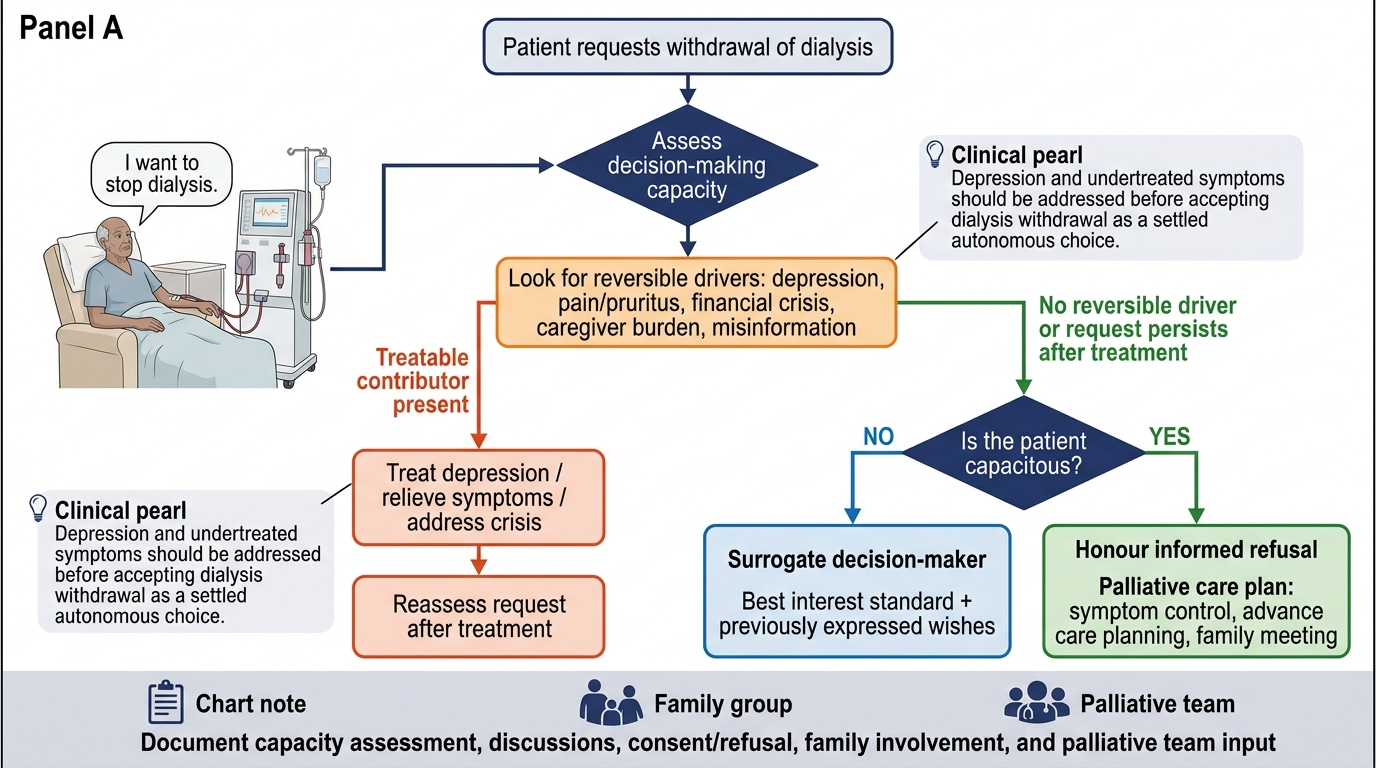
Ethical Flowchart for Withdrawal of Dialysis Request
SELF-CHECK
A 65-year-old man on maintenance haemodialysis for 3 years says he wants to stop dialysis because he is 'tired of living like this.' Assessment reveals moderate depression (PHQ-9 score 14) and poorly controlled pruritus. He has full decision-making capacity. Which is the MOST appropriate initial response?
A. Respect his autonomy immediately and begin withdrawal of dialysis
B. Refer to a psychiatrist and address the pruritus; reassess his wish to withdraw after treatment
C. Ask his family to override his decision as he is depressed
D. Continue dialysis against his wishes as his depression means his decision is invalid
Reveal Answer
Answer: B. Refer to a psychiatrist and address the pruritus; reassess his wish to withdraw after treatment
A patient with depression and undertreated symptoms (pruritus causing distress) may be expressing a wish to withdraw dialysis that is driven by treatable, reversible suffering rather than a settled, autonomous preference. Before honoring a withdrawal request, it is clinically and ethically appropriate to identify and treat potentially reversible contributors — depression (antidepressant therapy, counselling) and pruritus (antihistamine, gabapentin, optimisation of phosphate control). If after adequate treatment the patient persists in the wish to withdraw, that decision should be respected. Overriding the decision of a capacitous patient because of depression is not correct (depression is not the same as lack of capacity, and capacity must be formally assessed). Asking the family to override a capacitous patient's wishes is a violation of autonomy.
CLINICAL PEARL
Conservative kidney management (CKM) is a legitimate, evidence-based, and humane alternative to dialysis for selected patients — typically elderly (>75 years), frail, or multimorbid individuals where dialysis adds burden without meaningful survival benefit. CKM comprises active management of all CKD complications (hypertension, anaemia, hyperphosphataemia, acidosis, fluid overload) combined with symptom-focused palliative care, without dialysis or transplantation. Studies from the UK (Murphy et al., 2016) and Australia show that in carefully selected elderly patients, survival on CKM versus dialysis is similar (median 18–24 months vs 20–30 months), with dramatically fewer hospital days and better reported symptom control for CKM patients. Introducing CKM as an option to all patients — not just those who reject dialysis — is good medical practice. The clinician who presents dialysis as the only option deprives patients of the right to make a genuinely informed choice about how they want to spend the remainder of their life.
Self-Assessment — Ethics and QoL Integration Scenarios
The self-assessment scenarios below test your ability to apply the ethical frameworks, legal knowledge, and QoL-informed clinical thinking covered in this module to realistic patient encounters. For each scenario, identify the core ethical principle at stake, the relevant legal provision under THOA (if applicable), the appropriate clinical response, and any pitfalls to avoid. These scenarios are representative of the type of discussion questions used in final-year long-case examinations and clinical vivas, where examiners specifically probe for ethical reasoning beyond simple factual recall. Work through each scenario carefully before reading the analysis — articulate your reasoning as if you were explaining it to an examiner, because the examination itself will require exactly this level of structured explanation. In all three scenarios, resist the temptation to jump to the most medically obvious action; the ethical dimension requires you to slow down and think through the principles before acting. Good ethical reasoning in renal medicine is not about having a formulaic answer — it is about demonstrating that you have considered the patient's autonomy, the relevant legal framework, the quality-of-life impact, and the alternative clinical options before arriving at a recommendation. That deliberateness is what the examiner is looking for and what the patient deserves.
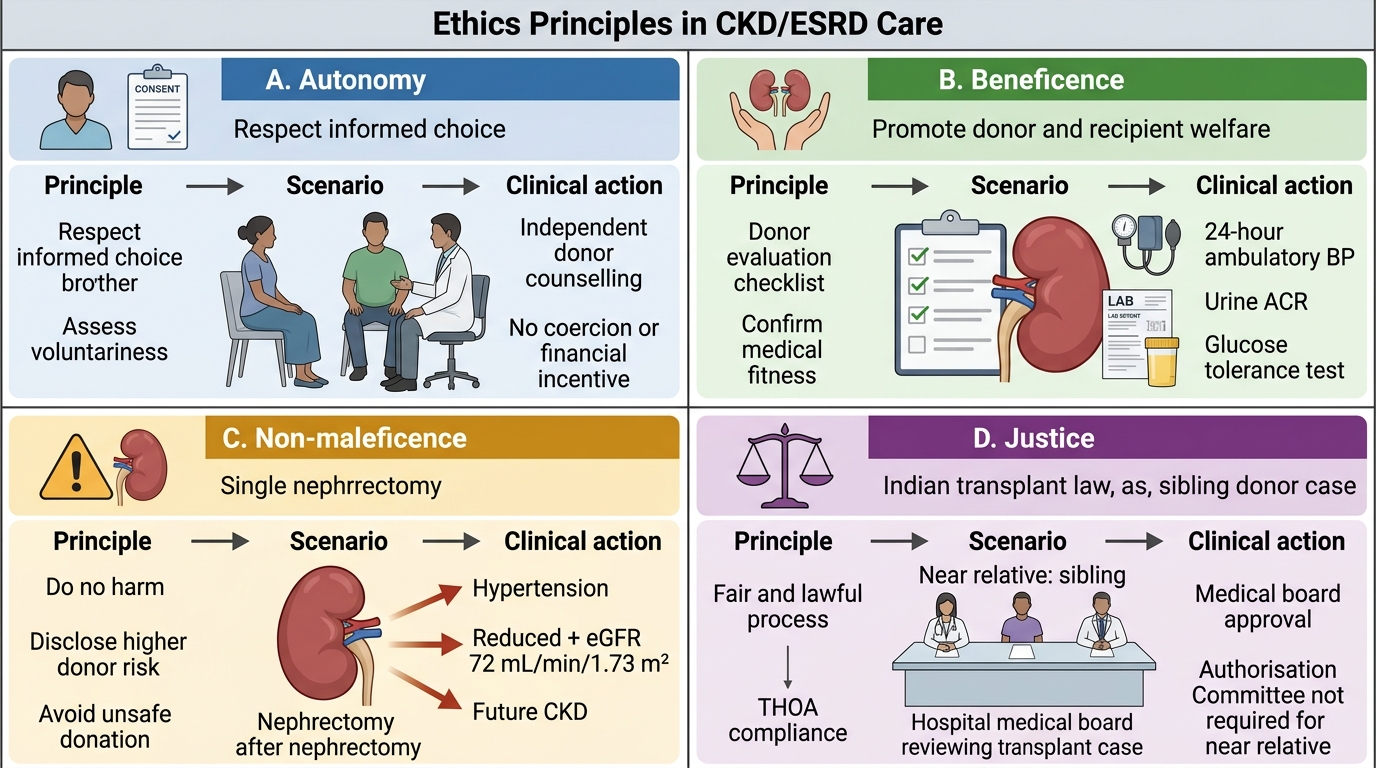
Ethics Principles in CKD/ESRD Living Donation
Scenario A: A 35-year-old woman with ESRD from lupus nephritis has a willing kidney donor — her 28-year-old brother. The brother has mild hypertension controlled on a single medication and eGFR of 72 mL/min/1.73 m². He genuinely wishes to donate. The hospital's medical board has approved the procedure. What ethical and medical concerns should be assessed before proceeding?
Analysis: The ethical framework is living-related donation under THOA (near relative = sibling = near relative, hospital medical board approval sufficient — no Authorisation Committee needed). Ethical concerns: (1) Voluntariness — is the brother's consent genuinely free from family pressure or financial incentive? (2) Informed risk disclosure — a donor with hypertension and eGFR 72 has a higher-than-average risk of progression to CKD themselves following unilateral nephrectomy; this must be disclosed clearly. (3) Donor best interest — medical evaluation should include 24-hour ambulatory BP monitoring, urine ACR (to exclude subclinical proteinuria), glucose tolerance test (diabetes in a donor accelerates decline in the remaining kidney). The brother should be counselled independently (without the recipient present) to ensure freedom from coercion. If eGFR 72 and mild hypertension are the only findings and they are genuinely stable, proceeding after thorough counselling is ethically appropriate.
Scenario B: A 50-year-old man on IHD has not been attending his sessions — he has missed 6 of the last 12 sessions. He arrives at the emergency department with pulmonary oedema and K⁺ 7.1 mEq/L. He says he has been missing dialysis because he cannot afford the Rs 1,800 per session and his wife has lost her job. After emergency treatment, he says he will stop dialysis entirely as he 'cannot burden his family anymore.' What is the priority ethical and clinical response?
Analysis: Two ethical issues: (1) Financial crisis driving treatment non-adherence — this is an access-to-justice issue, not autonomous refusal; the physician must urgently explore government schemes (PMJAY, state health mission dialysis programmes), non-governmental support, and social worker involvement. Many government hospitals provide dialysis at subsidised or no cost; private patients must be helped to access these. (2) The statement about stopping must be assessed — is this a depressed response to a crisis (potentially reversible if financial pressure is relieved), or a settled autonomous preference? Depression screening is mandatory. If the financial crisis is addressed and depression treated, many patients reverse this decision. The ethical error would be to treat this as a simple autonomous refusal and withdraw care without first addressing the underlying crisis.
Scenario C: A 70-year-old woman with ESRD, CKD-MBD, moderate dementia, and ischaemic heart disease is admitted with uraemia. Her family insists on starting haemodialysis. She cannot consistently articulate preferences due to dementia. She grimaces and pulls away from the access needle during prior attempts. What ethical framework guides this decision?
Analysis: This is a surrogate decision-making scenario for a patient without current capacity. The framework is best interest standard — in the absence of a valid advance directive, the surrogate (family) should make decisions that best reflect what the patient would have wanted based on their prior expressed values, personality, and life goals (substituted judgement), combined with the clinical assessment of burdens versus benefits (beneficence/non-maleficence). The family's insistence on dialysis must be weighed against: the patient's behavioural responses (grimacing, withdrawal — suggesting distress from procedures), the limited survival benefit of dialysis in this multimorbid elderly patient, and any prior expressed preferences. An ethics committee or palliative care consultation is appropriate. The physician is not obligated to provide a treatment that is clinically futile or that causes disproportionate suffering — the family's preferences do not override the clinical futility assessment.