Page 16 of 23
IM11.{14-15,22-24} | Diabetic Emergencies — SDL Guide
Learning Objectives
- Recognise the presentation of hypoglycaemia and outline the principles of its therapy including the counter-regulatory hormone response and causes
- Recognise the presentation of DKA and HHS (diabetic emergencies) and outline the principles of therapy
- Enumerate the causes of hypoglycaemia and describe the counter-regulatory hormone response and initial approach
- Describe the precipitating causes, pathophysiology, recognition, clinical features, diagnosis, stabilisation, and management of diabetic ketoacidosis
- Describe the precipitating causes, pathophysiology, recognition, clinical features, diagnosis, stabilisation, and management of hyperosmolar hyperglycaemic state
INSTRUCTIONS
Diabetic emergencies are immediately life-threatening conditions requiring rapid recognition and structured resuscitation. This module covers the three principal emergencies — hypoglycaemia, DKA, and HHS — with a focus on pathophysiology, diagnostic criteria, and step-by-step management protocols that must be executed correctly under time pressure.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 404 — Diabetic Ketoacidosis and Hyperosmolar State (textbook)
- API Textbook of Medicine, 10th ed., Ch. 51 — Diabetic Emergencies (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 21 — Emergencies in Diabetes (textbook)
- Joint British Diabetes Societies Inpatient Care Group — Management of Diabetic Ketoacidosis in Adults, 2021 (guideline)
- American Diabetes Association — Hyperglycemic Crises in Adult Patients with Diabetes (Position Statement), 2009 (updated 2021) (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 am in the medical casualty. Three patients arrive within 30 minutes. Patient 1 is a 22-year-old T1DM woman brought by her flatmate, confused and diaphoretic, blood glucose 38 mg/dL on the triage glucometer. She was fine at 11 pm. Patient 2 is a 78-year-old man with known T2DM found semi-conscious at home by his neighbour; blood glucose 720 mg/dL, serum sodium 152 mEq/L, urine ketones negative, and his breathing is normal. Patient 3 is a 19-year-old boy with new-onset T1DM, brought by his parents after 3 days of vomiting and abdominal pain; blood glucose 420 mg/dL, deep laboured breathing, urine ketones 4+, arterial pH 7.18. Three different metabolic crises — each potentially fatal, each requiring a different immediate treatment. The intern on call has 5 minutes to initiate appropriate resuscitation before the senior arrives. Do you know what to do for each patient right now? This module builds that knowledge.
WHY THIS MATTERS
Diabetic emergencies are among the most common medical emergencies encountered in Indian hospitals. DKA mortality in India ranges from 3–10% in tertiary centres and higher in resource-limited settings — predominantly from late presentation, missed precipitants (particularly infections and undiagnosed new T1DM), and errors in fluid and potassium management. HHS carries a mortality of up to 20% in published series, driven by the severity of dehydration and neurological impairment in elderly comorbid patients. Severe hypoglycaemia causes permanent neurological injury and death if not reversed within minutes. The NMC competencies IM11.14, 11.15, 11.22, 11.23, and 11.24 require you to know the causes, presentations, diagnostic criteria, and management of all three emergencies in sufficient detail to initiate resuscitation independently as a first-year intern.
RECALL
Before proceeding, recall the four biochemical pathways linking insulin deficiency to the abnormalities seen in diabetic emergencies. (1) Glucose metabolism: Without insulin, GLUT-4-dependent glucose uptake by muscle and fat is abolished, and hepatic glucose output is unrestrained — causing hyperglycaemia. (2) Lipolysis and ketogenesis: Without insulin, adipose lipase is unrestrained — free fatty acids flood the liver, are oxidised to acetyl-CoA, and are converted to ketone bodies (acetoacetate, beta-hydroxybutyrate, acetone) — causing ketoacidosis in states of absolute insulin deficiency (DKA). (3) Osmotic diuresis: Glucose above the renal threshold (~180 mg/dL) spills into urine, carrying water and electrolytes (especially sodium and potassium) — causing polyuria, dehydration, and electrolyte depletion. (4) Counter-regulatory response: As glucose falls below ~65 mg/dL (in hypoglycaemia), glucagon, adrenaline, cortisol, and growth hormone are released to restore normoglycaemia. These four pathways underpin all three emergencies covered in this module.
Hypoglycaemia: Causes, Counter-Regulatory Response, and Clinical Presentation
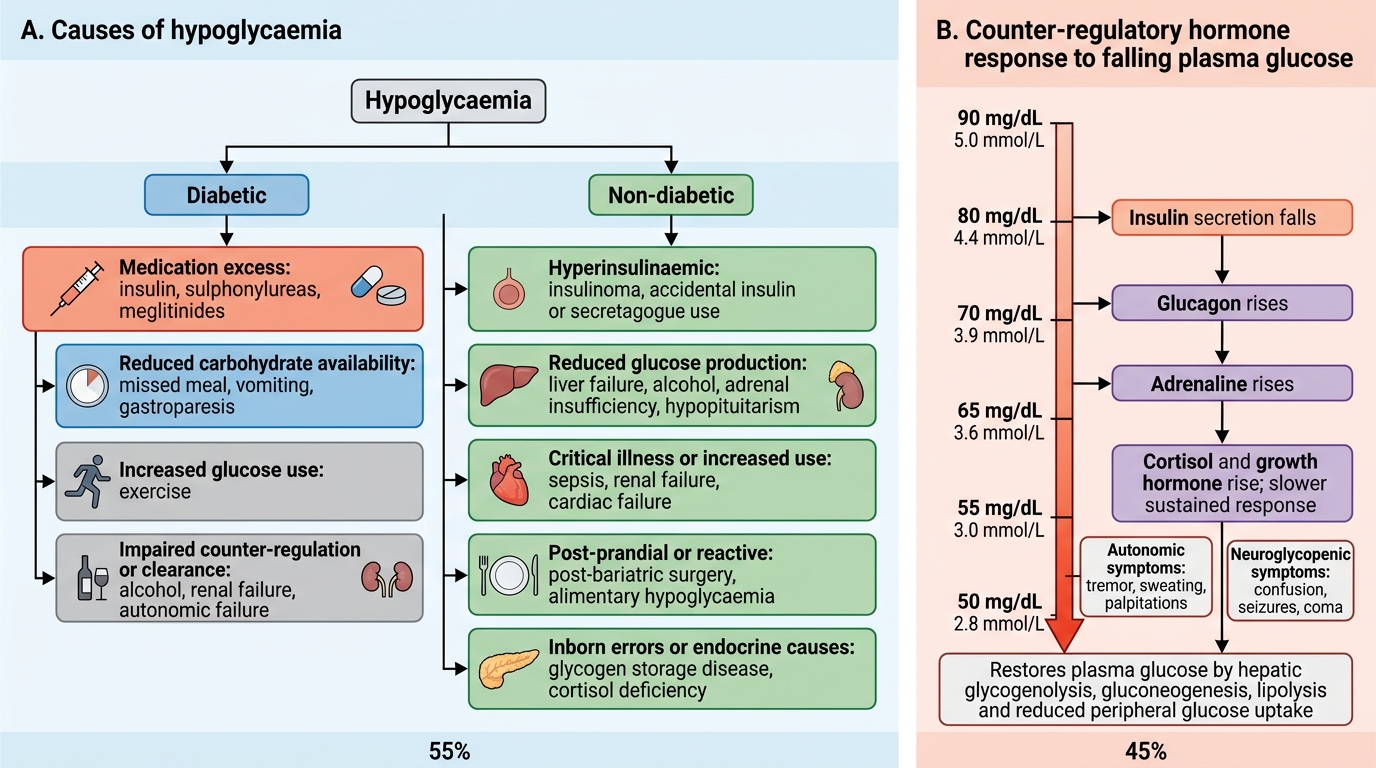
Hypoglycaemia is defined as a blood glucose level low enough to cause symptoms or signs. The clinical threshold commonly cited is <70 mg/dL (3.9 mmol/L) as the 'alert value' requiring action in treated diabetes; <54 mg/dL (3.0 mmol/L) represents serious clinically significant hypoglycaemia; and <40 mg/dL represents severe neuroglycopenic hypoglycaemia with risk of permanent neurological injury. In non-diabetic individuals, spontaneous hypoglycaemia is far less common and the Whipple's triad must be demonstrated: (1) symptoms consistent with hypoglycaemia, (2) low blood glucose, and (3) relief of symptoms with glucose administration. Understanding the causes of hypoglycaemia is essential because the correct treatment and the urgency of hospital admission depend on the underlying mechanism — insulin excess, sulphonylurea accumulation, alcohol, and endogenous causes each have distinct management pathways that cannot be conflated.
Causes of Hypoglycaemia — Classified:
In diabetic patients (the most common setting):
- Insulin excess: Too high a dose; inappropriate timing relative to meals; using the wrong type (rapid vs basal confusion); injection into lipohypertrophic area then correction to normal tissue
- Sulphonylurea excess: Especially glibenclamide (prolonged action, renally cleared — accumulates in CKD); dose error; interaction with other drugs
- Missed, delayed, or inadequate meal after insulin or SU dose
- Unplanned exercise: Physical activity dramatically increases glucose utilisation; insulin-treated patients are at high risk if they exercise without reducing dose or increasing carbohydrate intake
- Alcohol: Inhibits hepatic gluconeogenesis (glycogen stores become depleted); nocturnal or delayed hypoglycaemia common after evening alcohol intake in insulin/SU users
- Renal failure: Reduces insulin clearance (insulin is partly metabolised in the kidney) and impairs gluconeogenesis
- Intercurrent illness, particularly gastroenteritis: Vomiting/diarrhoea reduces carbohydrate absorption; if insulin dose not adjusted, hypoglycaemia results
In non-diabetic patients:
- Insulinoma: Autonomous insulin secretion from a pancreatic beta-cell tumour; Whipple's triad present; non-suppressible C-peptide and insulin during hypoglycaemia
- Adrenal insufficiency (Addison's disease): Cortisol is a key counter-regulatory hormone; its absence reduces gluconeogenesis and glycogen mobilisation; hypoglycaemia is fasting and exercise-induced
- Severe hepatic failure: The liver is the primary source of gluconeogenesis; when liver function is critically impaired, fasting hypoglycaemia occurs
- Reactive hypoglycaemia (postprandial): 2–4 hours after a high-carbohydrate meal, exaggerated insulin response causes transient hypoglycaemia; seen post-gastric bypass surgery (dumping syndrome variant)
- Factitious hypoglycaemia: Exogenous insulin or SU administration; C-peptide is suppressed (exogenous insulin) or urine SU screen positive
- Sepsis: Increased peripheral glucose utilisation and impaired gluconeogenesis
The Counter-Regulatory Hormone Response:
As blood glucose falls below approximately 65 mg/dL, a hierarchical counter-regulatory response is activated. Glucagon (secreted from alpha cells) is the primary counter-regulatory hormone — it stimulates hepatic glycogenolysis and gluconeogenesis within minutes, rapidly restoring blood glucose. Adrenaline (epinephrine) is the second line — it reinforces glucagon's effect, stimulates glycogenolysis in muscle, and simultaneously triggers the adrenergic symptoms that serve as the clinical warning of hypoglycaemia. Cortisol and growth hormone contribute over longer timeframes (hours) by promoting gluconeogenesis and reducing peripheral glucose utilisation. In patients with longstanding T1DM, glucagon secretion in response to hypoglycaemia becomes progressively impaired, making adrenaline the primary counter-regulatory defence — but adrenaline response also diminishes with recurrent hypoglycaemia (hypoglycaemia unawareness). This loss of physiological defence makes severe hypoglycaemia particularly dangerous in T1DM of long duration.
Clinical Presentation:
Symptoms are classified by mechanism:
- Adrenergic (autonomic) symptoms (triggered at ~60–65 mg/dL): sweating, tremor, palpitations, tachycardia, pallor, hunger, anxiety — these are the warning symptoms that allow the patient to self-treat
- Neuroglycopenic symptoms (triggered at <50 mg/dL, progressing with lower glucose): difficulty concentrating, confusion, slurred speech, visual disturbances, focal neurological signs, seizures, coma
- Severe hypoglycaemia: Defined as requiring assistance from another person; the patient is unable to self-treat; risk of permanent neurological injury if prolonged (>30 minutes of glucose <40 mg/dL)
Hypoglycaemia: Causes and Counter-Regulatory Response
Hypoglycaemia: Diagnosis and Management
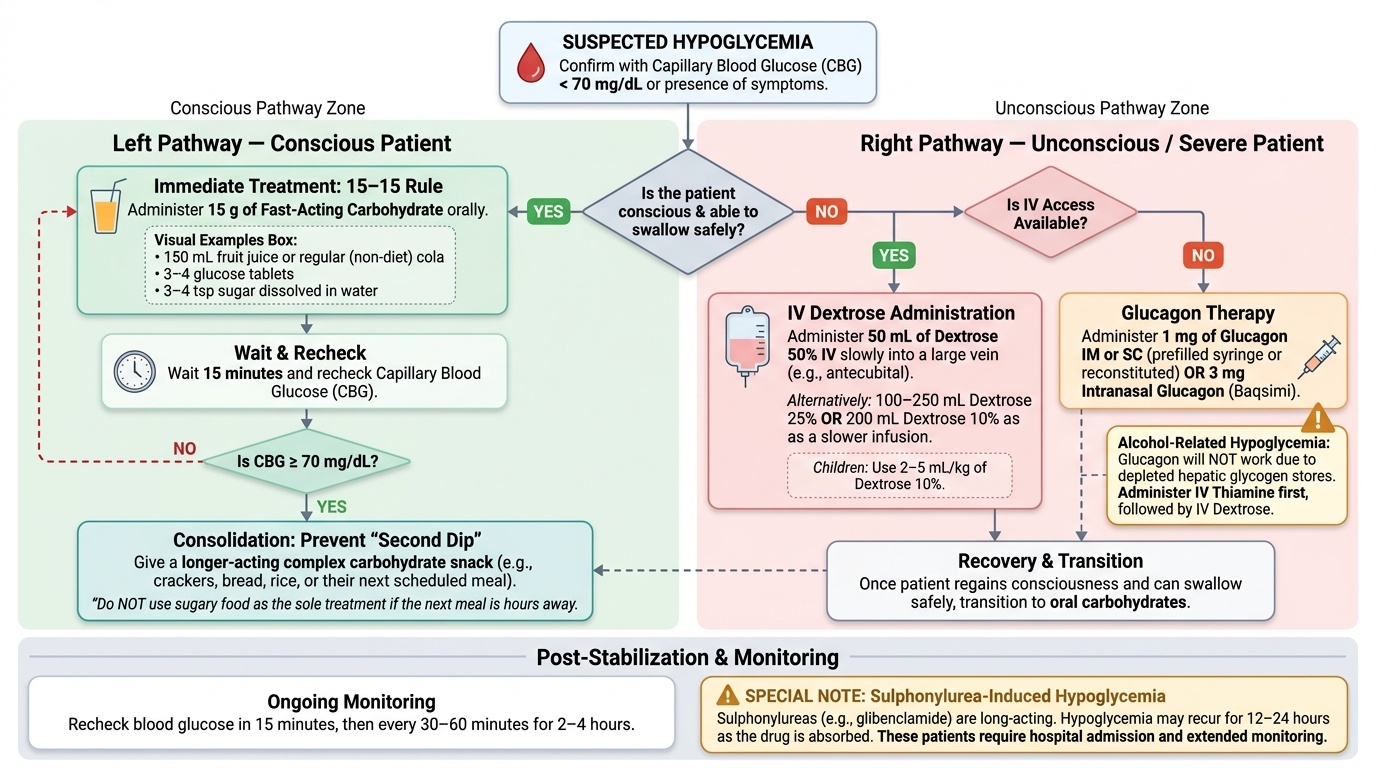
The diagnosis of hypoglycaemia is confirmed by a blood glucose measurement below the threshold. In a conscious symptomatic patient, bedside capillary blood glucose (CBG) is sufficient to guide immediate treatment — laboratory confirmation can follow. In an unconscious patient, CBG must be obtained within the first minute of assessment, as the differential diagnosis of coma is wide and hypoglycaemia is both common and immediately reversible if treated promptly. Do not wait for laboratory glucose in a comatose patient on insulin or sulphonylurea.
Provided image
Principles of Management:
Mild-moderate hypoglycaemia (conscious patient):
Apply the 15–15 Rule: administer 15 g of fast-acting carbohydrate orally — 150 mL of fruit juice, 150 mL of regular (non-diet) cola, 3–4 glucose tablets (each approximately 4–5 g), or 3–4 teaspoons of sugar dissolved in water. Recheck blood glucose after 15 minutes. If glucose is still <70 mg/dL, repeat the 15 g carbohydrate. Once glucose is ≥70 mg/dL and the patient is stable, give a longer-acting carbohydrate snack (crackers, bread, rice) to prevent recurrence. Do NOT give sugary food as the sole treatment if the next meal is hours away — longer-acting starch + protein prevents the 'second dip.'
Severe hypoglycaemia (unconscious or unable to swallow — the most critical scenario):
- If IV access is available: Give 50 mL of 50% dextrose (dextrose 50%) IV (= 25 g glucose), injected slowly into a large vein (irritant — avoid peripheral small veins; use antecubital or larger). Alternatively, 100–250 mL of 25% dextrose or 200 mL of 10% dextrose as a slower infusion. Children: use 2–5 mL/kg of 10% dextrose.
- If IV access is NOT available: Administer 1 mg of glucagon IM or SC (available as a pre-filled syringe; reconstitute from powder if kit-form). Glucagon stimulates hepatic glycogenolysis — it will NOT work if glycogen stores are depleted (alcohol-related hypoglycaemia, prolonged fasting). An intranasal glucagon preparation (Baqsimi, 3 mg) is an alternative where available.
- Once conscious, give oral carbohydrate as above.
- Recheck glucose in 15 minutes and every 30–60 minutes for 2–4 hours, especially in sulphonylurea-induced hypoglycaemia (SU is still being absorbed and hypoglycaemia may recur for 12–24 hours with long-acting agents like glibenclamide — these patients require hospital admission and glucose infusion monitoring).
Specific considerations:
- Sulphonylurea-induced hypoglycaemia in the elderly: Must NEVER be discharged after a single glucose correction — glibenclamide's active metabolites persist for 24+ hours, and recurrent life-threatening hypoglycaemia is common. Admit, start 10% dextrose infusion, and monitor glucose 2-hourly.
- Alcoholic hypoglycaemia: Glucagon is INEFFECTIVE (depleted glycogen stores). IV dextrose is the only treatment. Also give IV thiamine (Vitamin B1) before dextrose in alcohol-related hypoglycaemia to prevent precipitating Wernicke's encephalopathy.
- Investigation after non-diabetic hypoglycaemia: Supervise a diagnostic fast (supervised 72-hour fast under observation) if insulinoma or other endogenous cause is suspected; measure glucose, insulin, C-peptide, and beta-hydroxybutyrate simultaneously at the time of hypoglycaemia.
SELF-CHECK
A 68-year-old woman on glibenclamide 5 mg twice daily is brought to casualty with a blood glucose of 44 mg/dL. She is confused but responds to commands. You give her a glass of orange juice (15 g glucose) and her glucose rises to 78 mg/dL, and she becomes alert. You are about to discharge her when her daughter asks if she can go home. What is the MOST appropriate decision?
A. Discharge with advice to eat a larger meal and halve her glibenclamide dose immediately
B. Admit for at least 24 hours with IV dextrose infusion and 2-hourly glucose monitoring
C. Discharge after 2 more hours of observation if glucose remains above 70 mg/dL
D. Stop glibenclamide completely and discharge with a new prescription for metformin
Reveal Answer
Answer: B. Admit for at least 24 hours with IV dextrose infusion and 2-hourly glucose monitoring
Glibenclamide is a long-acting sulphonylurea with active metabolites that are renally cleared. In elderly patients (often with some degree of impaired renal clearance even with a 'normal' creatinine), glibenclamide's active metabolites persist for 24 hours or more. Correcting the glucose with a short-acting carbohydrate does not eliminate the ongoing insulinotropic stimulus from the circulating SU. The glucose will recur — often more severely — within hours. This patient must be admitted, started on a 10% dextrose infusion, and monitored with 2-hourly capillary glucose testing. Discharge after juice alone risks potentially fatal recurrent hypoglycaemia in the next 12–24 hours. Stopping the drug is appropriate as a long-term decision but does not protect her tonight.
Diabetic Ketoacidosis: Pathophysiology and Clinical Recognition
Diabetic ketoacidosis (DKA) is an acute, life-threatening metabolic complication of diabetes characterised by the triad of hyperglycaemia, ketonaemia/ketonuria, and metabolic acidosis. It occurs predominantly in T1DM (where absolute insulin deficiency is the norm) but can also occur in T2DM in the context of severe physiological stress, in LADA (latent autoimmune diabetes in adults), in ketosis-prone T2DM (a variant more common in Black African and South Asian patients), and in patients with T2DM on SGLT2 inhibitors — the so-called euglycaemic DKA, where blood glucose may be <250 mg/dL despite active ketoacidosis, a diagnostic pitfall that has caused fatal delays in treatment. Recognising which clinical contexts trigger DKA, and understanding the dual pathophysiological defect (absolute insulin deficiency combined with counter-regulatory hormone excess) that drives all three metabolic crises simultaneously, is the foundation of competent management.
Precipitating Factors:
A precipitating event is identifiable in over 80% of DKA cases. The most important precipitants:
- Infection — the single most common precipitant in all series; pneumonia, urinary tract infection, and soft tissue infection are most frequent; infection dramatically increases counter-regulatory hormones (cortisol, glucagon, adrenaline) and increases insulin requirements
- Missed or inadequate insulin dose — including deliberate omission (insulin omission for weight loss, known as 'diabulimia', is increasingly recognised, especially in young women with T1DM)
- New-onset T1DM — DKA is the presenting event in 20–40% of new T1DM diagnoses in India
- Acute myocardial infarction (can be silent in diabetes — always check ECG and troponin in DKA)
- Stroke, pancreatitis, trauma, surgery
- SGLT2 inhibitor use — euglycaemic DKA; blood glucose may be <250 mg/dL
- Drugs — high-dose steroids, antipsychotics, sympathomimetics
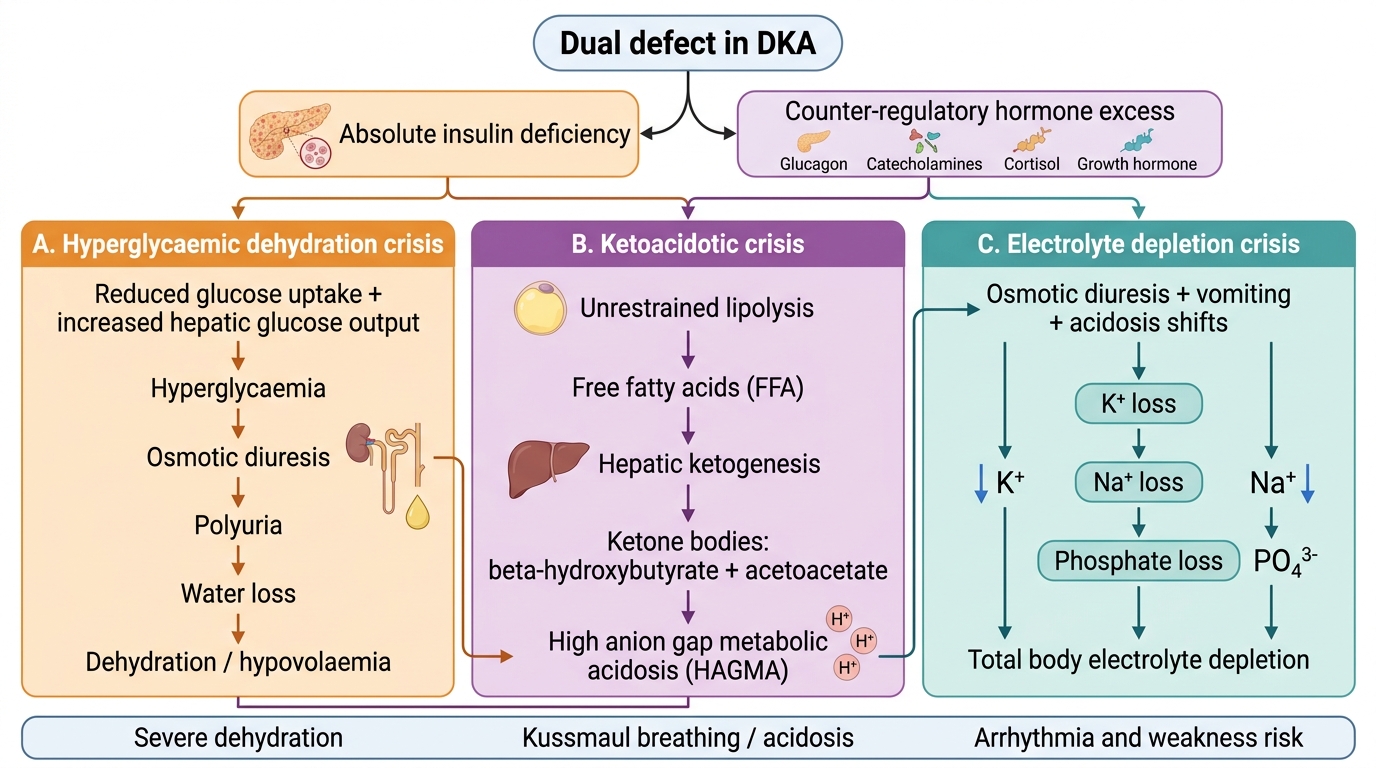
Pathophysiology of DKA:
The core defect is absolute insulin deficiency (or severe relative deficiency) combined with excess counter-regulatory hormones. This dual defect produces three parallel metabolic crises:
1. Hyperglycaemia: Hepatic glucose output (both glycogenolysis and gluconeogenesis) is unrestrained; glucose uptake by muscle and fat is negligible. Blood glucose rises, often exceeding 300–400 mg/dL, causing osmotic diuresis with profound water and electrolyte loss.
2. Ketogenesis: Without insulin to inhibit adipose lipase, lipolysis is unrestrained — free fatty acids flood the liver and are converted to ketone bodies (acetoacetate and beta-hydroxybutyrate) at a rate exceeding peripheral utilisation. Beta-hydroxybutyrate is the dominant ketone in DKA (BHB:acetoacetate ratio 3–10:1). The resulting high anion gap metabolic acidosis (HAGMA) is characterised by pH <7.3 and bicarbonate <18 mEq/L.
3. Dehydration and electrolyte depletion: Osmotic diuresis from glucose and ketones causes total body water deficit of 3–5 L. Total body potassium is depleted by 3–5 mEq/kg (equivalent to 200–400 mEq), despite the fact that serum K+ is often normal or elevated at presentation (due to insulin deficiency causing intracellular K+ to shift extracellularly, and acidosis further worsening this shift). This is the most treacherous aspect of DKA electrolyte management: the serum K+ appears adequate but the patient is actually profoundly K+-depleted, and giving insulin will drive K+ back into cells, potentially causing fatal hypokalaemia.
Diagnostic Criteria for DKA (American Diabetes Association):
- Blood glucose >250 mg/dL (though euglycaemic DKA <250 mg/dL in SGLT2i users)
- Arterial pH <7.3 (mild: 7.25–7.30; moderate: 7.00–7.24; severe: <7.00)
- Serum bicarbonate <18 mEq/L (mild: 15–18; moderate: 10–14; severe: <10)
- Positive serum or urine ketones (≥2+ on dipstick; blood BHB >3.0 mmol/L)
- Anion gap >12 mEq/L (typically >20 in DKA)
Clinical Recognition:
The clinical picture of DKA: Young T1DM patient (or stressed T2DM); history of polyuria, polydipsia, and nausea/vomiting over hours to 2 days; preceding illness or missed insulin history. On examination: dehydrated (dry mucous membranes, reduced skin turgor, sunken eyes, tachycardia, hypotension in severe cases); Kussmaul breathing (deep, regular, slightly increased rate — the single most pathognomonic clinical sign); acetone breath (sweet, fruity odour); abdominal pain and tenderness (may mimic acute abdomen — typically abdominal pain in DKA is metabolic; always check amylase/lipase to exclude pancreatitis as precipitant; perform abdominal examination after resuscitation begins). Altered consciousness in severe DKA (pH <7.0): drowsy → stuporous → comatose.
Pathophysiology of Diabetic Ketoacidosis