Page 17 of 23
IM11.{14-15,22-24} | Diabetic Emergencies — SDL Guide (Part 2)
Diabetic Ketoacidosis: Management Protocol
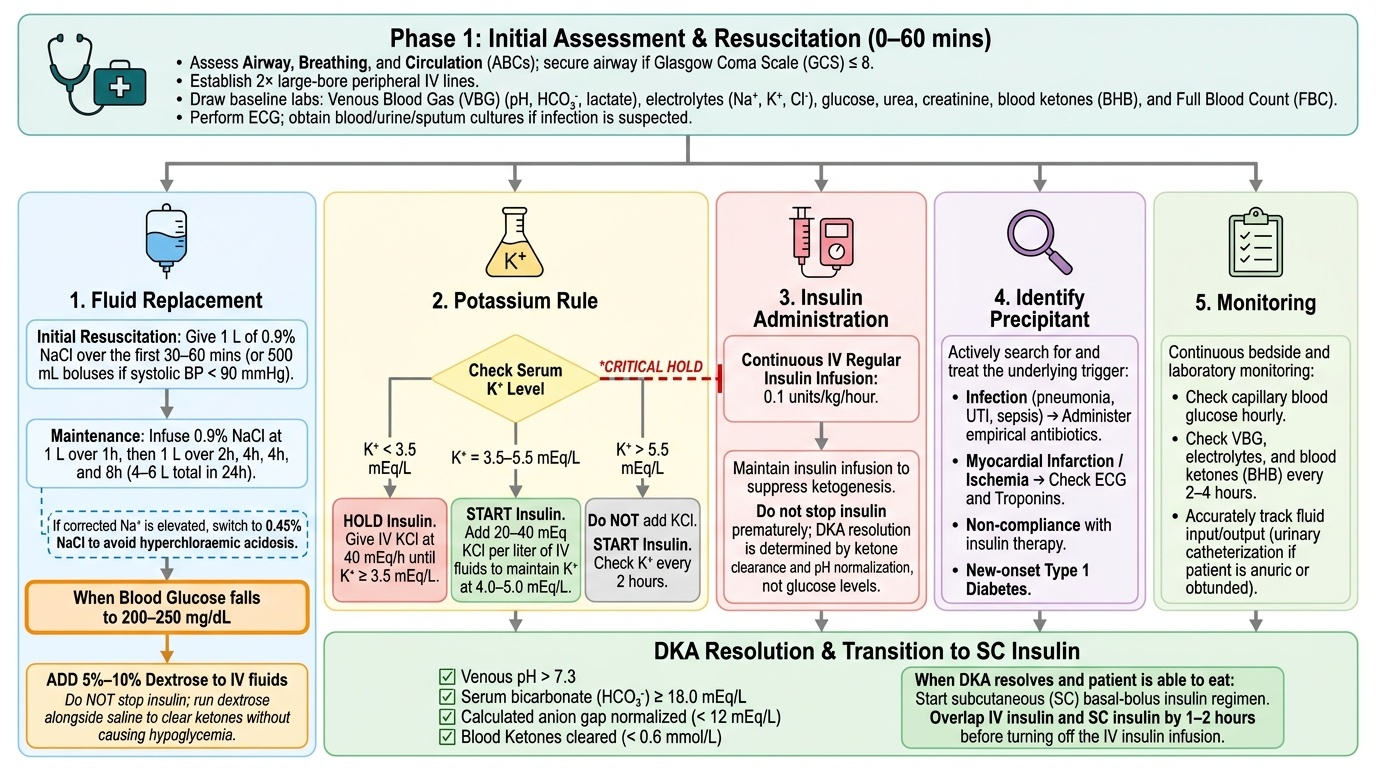
The management of DKA follows a structured protocol addressing the five parallel derangements simultaneously: fluid replacement, insulin administration, potassium replacement, management of the precipitating cause, and monitoring and resolution criteria. Getting the sequence and timing right is critical — particularly the K+ rule before insulin, and the decision to add dextrose to IV fluids when glucose falls.
Provided image
Step 1 — Initial Assessment and Resuscitation (0–60 minutes):
Airway, Breathing, Circulation — if GCS ≤8, protect airway. Two large-bore peripheral IV cannulae. Baseline blood tests: venous blood gas (pH, bicarbonate, lactate), serum glucose, electrolytes (Na+, K+, Cl−, HCO₃−), urea, creatinine, eGFR, full blood count (leucocytosis is expected in DKA even without infection — WBC up to 25,000/mm³ is not diagnostic of infection alone), blood cultures if febrile, blood ketones (BHB), urine dipstick, ECG, and urine/throat/sputum cultures to identify precipitant. Urinary catheterisation if anuric or obtunded (to accurately measure urine output).
Step 2 — Fluids (the most important initial intervention):
Fluid resuscitation corrects hypovolaemia, restores renal perfusion (which enhances glucose and ketone excretion), and dilutes circulating glucose and ketones. Standard protocol:
- 0.9% Sodium chloride (normal saline): 1 L in the first 30 minutes (if haemodynamically compromised, give 500 mL boluses until systolic BP ≥90 mmHg)
- Then: 1 L over 1 hour, 1 L over 2 hours, 1 L over 4 hours, 1 L over 4 hours, 1 L over 8 hours
- Total fluid in the first 24 hours: typically 4–6 L
- Switch to 0.45% NaCl (half-normal saline) if corrected sodium is high-normal or elevated (to avoid hyperchloraemic acidosis from excess 0.9% NaCl — this is a frequent management pitfall)
- When blood glucose falls to 200–250 mg/dL: add 5–10% dextrose to IV fluids (typically run alongside normal saline, not replacing it) to prevent hypoglycaemia while insulin infusion is continued to clear ketones. Do NOT stop insulin prematurely — DKA is resolved when KETONES are cleared, not when glucose normalises.
Step 3 — Potassium Replacement (CRITICAL before insulin):
Check serum K+ BEFORE starting insulin:
- K+ <3.5 mEq/L: HOLD insulin; give IV KCl at 40 mEq/hour until K+ ≥3.5 mEq/L, then start insulin
- K+ 3.5–5.5 mEq/L: Start insulin; add KCl 20–40 mEq/L to IV fluids
- K+ >5.5 mEq/L: Start insulin; hold K+ replacement; recheck K+ in 2 hours
Rationale: Insulin drives K+ into cells. If serum K+ is already low or borderline before insulin starts, the insulin-mediated intracellular shift will cause fatal hypokalaemia (cardiac arrhythmias, ventricular fibrillation). Monitor K+ every 1–2 hours during DKA treatment.
Step 4 — Insulin:
Fixed-rate intravenous insulin infusion (FRIII): 0.1 units/kg/hour (50 units of short-acting/regular insulin in 50 mL 0.9% NaCl — a 1 unit/mL solution; infused at rate = patient weight in kg × 0.1 mL/hour). Do NOT give an insulin bolus at the start — bolus doses cause rapid K+ shift without improving outcome. Continue insulin infusion until DKA is resolved (see resolution criteria below). Do NOT use long-acting insulin analogues during the acute phase. Subcutaneous insulin is not used in moderate/severe DKA (absorption is erratic due to poor peripheral perfusion).
Step 5 — Treating the Precipitant:
Search for and treat infection (blood and urine cultures, start empirical broad-spectrum antibiotics if infection suspected); check ECG and troponin for silent MI; check amylase/lipase for pancreatitis; review insulin prescriptions for missed doses.
Step 6 — Bicarbonate:
Sodium bicarbonate is NOT routinely given in DKA. It is reserved for life-threatening acidosis: pH <6.9 AND bicarbonate <5 mEq/L with haemodynamic instability (50–100 mEq/L 8.4% NaHCO₃ over 60 minutes). Risks of routine bicarbonate: paradoxical CNS acidosis (CO₂ crosses blood-brain barrier faster than bicarbonate), hypokalaemia (bicarbonate shifts K+ into cells), and delayed ketosis resolution.
Resolution Criteria (all three must be met):
- Blood glucose <200 mg/dL
- Serum bicarbonate ≥15 mEq/L (or blood pH ≥7.3)
- Blood BHB <0.6 mmol/L (or urine ketones ≤1+, accepting the limitation of dipstick BHB-blindness)
When resolution criteria are met: transition to subcutaneous insulin. Give SC basal insulin 30–60 minutes BEFORE stopping IV insulin infusion (avoid the gap that would cause ketosis recurrence).
SELF-CHECK
A 24-year-old T1DM patient is admitted with DKA. Initial investigations: glucose 440 mg/dL, pH 7.22, bicarbonate 11 mEq/L, potassium 3.2 mEq/L, sodium 134 mEq/L, blood BHB 6.4 mmol/L. You are about to start management. Which action should be performed FIRST?
A. Start IV insulin infusion at 0.1 units/kg/hour immediately to reduce ketone production
B. Give sodium bicarbonate because the pH is <7.3 and the patient has moderate DKA
C. Start IV potassium replacement and HOLD insulin until K+ rises to at least 3.5 mEq/L
D. Give an IV insulin bolus of 10 units to rapidly reduce blood glucose
Reveal Answer
Answer: C. Start IV potassium replacement and HOLD insulin until K+ rises to at least 3.5 mEq/L
The serum K+ is 3.2 mEq/L — below the threshold of 3.5 mEq/L. Insulin drives K+ into cells; starting insulin now will cause the K+ to fall further, potentially causing fatal cardiac arrhythmias. The protocol is unambiguous: if K+ <3.5 mEq/L, hold insulin and give IV KCl at 40 mEq/hour until K+ reaches ≥3.5 mEq/L, then start insulin. Bicarbonate is not indicated at pH 7.22 (reserved for pH <6.9 with haemodynamic instability). An insulin bolus is also contraindicated in DKA management — fixed-rate infusion only. Fluids (0.9% NaCl) should also be started simultaneously, but the critical gate before insulin is confirming adequate K+.
Hyperosmolar Hyperglycaemic State: Pathophysiology, Recognition, and Management
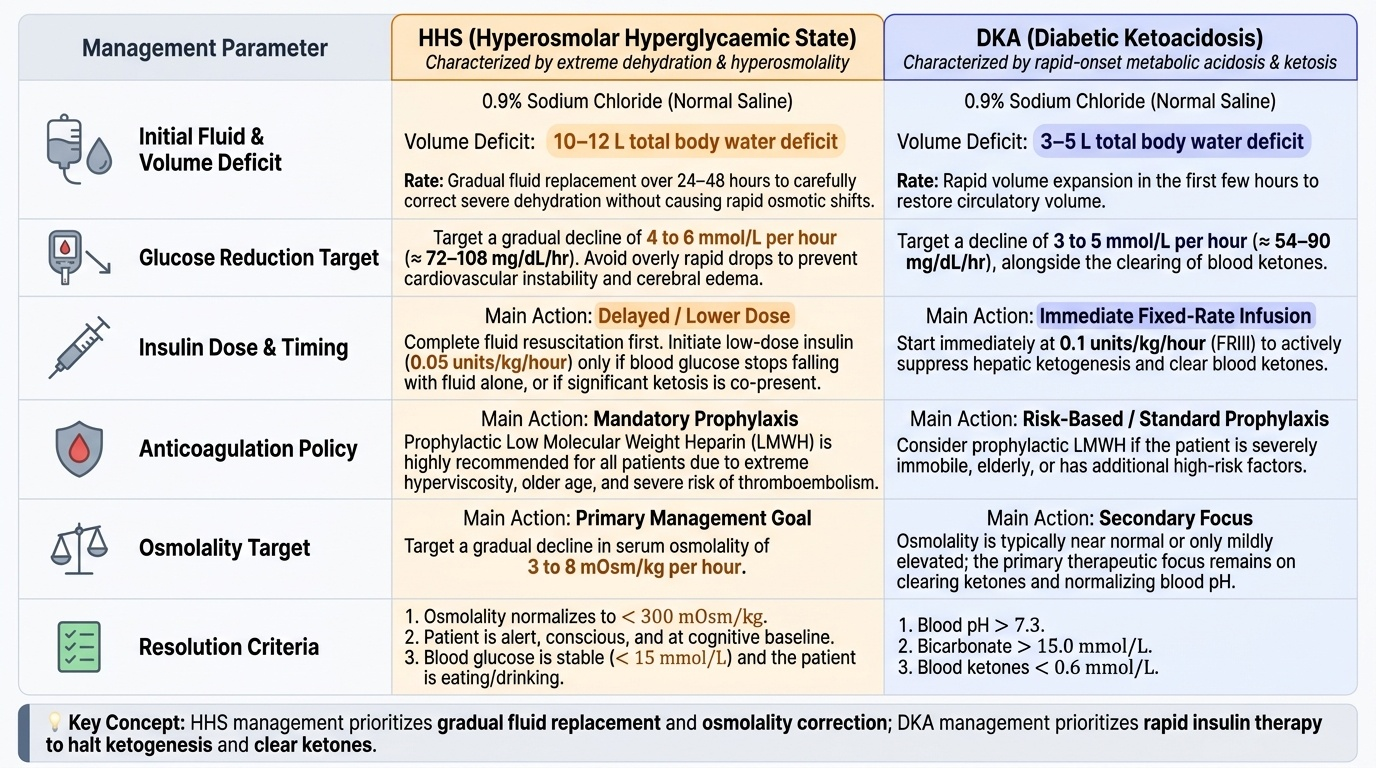
Hyperosmolar hyperglycaemic state (HHS) — formerly called hyperosmolar non-ketotic coma (HONK) — is an acute hyperglycaemic emergency characterised by extreme hyperglycaemia, profound hyperosmolality, severe dehydration, and neurological impairment, with minimal or absent ketosis. It occurs predominantly in elderly patients with T2DM, often as the first presentation of previously undiagnosed diabetes, and carries a mortality of 10–20% — substantially higher than DKA — because the patients are older, more comorbid, and the dehydration is far more extreme (10–12 L total body water deficit compared to 3–5 L in DKA). A critical concept that separates HHS from DKA is the reason ketosis does not develop: residual beta-cell insulin secretion in T2DM is sufficient to suppress adipose lipase and thereby prevent significant ketogenesis, even though the same residual secretion is entirely inadequate to prevent severe hyperglycaemia and osmotic diuresis. Understanding this distinction explains why the management priorities differ — fluid replacement and osmolality correction, not ketone clearance, are the primary targets in HHS.
Provided image
Precipitating Factors:
HHS has a prolonged prodrome (days to a week of worsening hyperglycaemia and osmotic symptoms before presentation) compared to DKA's more acute evolution. Common precipitants:
- Infection (particularly pneumonia, UTI, and cellulitis) — the most common precipitant, as in DKA
- Acute MI, stroke, or other acute illness triggering severe physiological stress
- Dialysis (peritoneal or haemodialysis) with high glucose content dialysate
- Medications: Corticosteroids, thiazide diuretics, olanzapine, phenytoin
- Failure of fluid intake (poor oral intake, inability to access water — particularly in cognitively impaired, institutionalised, or physically frail elderly patients)
- New-onset undiagnosed T2DM — the first presentation in a previously undiagnosed elderly diabetic
Pathophysiology:
In T2DM, residual insulin secretion is sufficient to suppress hepatic ketogenesis (the threshold for ketogenesis suppression is lower than for glucose control), explaining why HHS lacks significant ketosis despite extreme hyperglycaemia. The pathological process is primarily one of osmotic diuresis from severe sustained hyperglycaemia causing massive free water loss. The resulting extreme hyperosmolality (calculated serum osmolality = 2 × [Na+] + [glucose]/18 + [BUN]/2.8; diagnostic threshold >320 mOsm/kg) causes cerebral cellular dehydration, explaining the neurological features that dominate HHS. Total body water deficit in HHS is 10–12 L (compared to 3–5 L in DKA) — the most profound dehydration in clinical medicine. Total body K+ depletion is also severe (3–5 mEq/kg), though serum K+ may be elevated initially as in DKA.
Diagnostic Criteria for HHS:
- Blood glucose >600 mg/dL (typically 600–1200 mg/dL)
- Serum osmolality >320 mOsm/kg
- Absent or minimal ketonaemia (blood BHB <3.0 mmol/L; urine ketones negative or trace)
- Normal or near-normal pH (>7.3)
- Normal or elevated bicarbonate (>15 mEq/L)
- Marked neurological impairment (confusion → stupor → coma; focal deficits, seizures)
Management of HHS:
The management principles differ from DKA in important ways:
Fluids — the cornerstone of HHS management:
The fluid deficit is much larger (10–12 L). Use 0.9% NaCl for the first 1–2 litres to restore intravascular volume; if corrected sodium is >145 mEq/L (hypernatraemia), switch to 0.45% NaCl (half-normal saline) or even 5% dextrose in water to replace the free water deficit. The aim is to reduce osmolality gradually — no faster than 3–4 mOsm/kg/hour (too rapid reduction risks cerebral oedema). Typical fluid replacement: 0.5–1 L/hour for the first 4 hours, then slower. Total replacement over 24–48 hours. Correct sodium using the formula: corrected Na = measured Na + 1.6 × (glucose − 100)/100 mg/dL.
Insulin — used more cautiously than in DKA:
Low-dose insulin infusion (0.05 units/kg/hour, not 0.1) once fluids have been running for 1–2 hours and volume status is improving. In HHS, fluids alone reduce glucose significantly (by increasing renal glucose excretion once circulation is restored); premature high-dose insulin can cause dangerously rapid osmolality reduction. If glucose is falling adequately on fluids alone (>3–4 mmol/L/hour = approximately 54–72 mg/dL/hour), insulin may not need to be initiated immediately. Check K+ before insulin (same rules as DKA — hold if K+ <3.5 mEq/L).
Anticoagulation:
HHS confers extremely high risk of venous thromboembolism (VTE) — the combination of hyperviscosity, dehydration, reduced mobility, and vascular endothelial activation makes DVT and PE major causes of death. Low molecular weight heparin (LMWH) prophylaxis (enoxaparin 40 mg SC daily) should be started from admission unless active bleeding or contraindication. Full anticoagulation may be needed if DVT or PE is confirmed.
Identifying and treating the precipitant:
Investigate and treat the precipitating illness (cultures, ECG, troponin, CT brain if new focal deficits or fever with meningism). Neurological features (seizures, focal deficits) may be directly caused by hyperosmolality and often resolve with rehydration — do not attribute to stroke without imaging.
SELF-CHECK
A 72-year-old man with T2DM is admitted with blood glucose 840 mg/dL, serum osmolality 348 mOsm/kg, sodium 156 mEq/L, pH 7.38, bicarbonate 22 mEq/L, potassium 4.2 mEq/L, urine ketones negative. He is confused and not responding to commands. You start IV fluids (0.9% NaCl at 1 L/hour). After 2 hours of fluid resuscitation, blood glucose has fallen to 680 mg/dL and osmolality to 338 mOsm/kg. What is the NEXT most appropriate step?
A. Start insulin infusion at 0.1 units/kg/hour — the glucose is still very high
B. Switch IV fluid to 0.45% NaCl and start low-dose insulin at 0.05 units/kg/hour
C. Give sodium bicarbonate because bicarbonate of 22 is still slightly below normal
D. Perform immediate CT brain — the confusion may be due to a concurrent stroke
Reveal Answer
Answer: B. Switch IV fluid to 0.45% NaCl and start low-dose insulin at 0.05 units/kg/hour
In HHS, the sodium is high (156 mEq/L) confirming free water deficit relative to solutes. Continuing 0.9% NaCl will add sodium to a patient who is already hypernatraemic — switch to 0.45% NaCl (or 5% dextrose once glucose falls to 300 mg/dL) to replace the free water deficit and reduce osmolality gradually. Start low-dose insulin at 0.05 units/kg/hour (not the 0.1 used in DKA) now that initial fluid resuscitation has begun. Full-dose insulin (0.1 units/kg/hr) risks too rapid an osmolality drop, which can cause cerebral oedema. Bicarbonate is normal (22 mEq/L) — no indication for NaHCO₃. CT brain is reasonable to consider but is not the immediate priority over continued resuscitation; neurological features in HHS are often directly caused by hyperosmolality and typically improve with rehydration.
Self-Assessment: Managing Diabetic Emergencies Under Pressure
The three diabetic emergencies — hypoglycaemia, DKA, and HHS — each require rapid decision-making under pressure. The scenarios below test your ability to apply the management protocols correctly when complications arise mid-treatment, as they inevitably do in real patients. Work through each scenario before reading the analysis.
Scenario A — DKA Developing Hypokalaemia During Treatment:
A 28-year-old T1DM patient with DKA is receiving IV insulin infusion at 0.1 units/kg/hour and 0.9% NaCl with 40 mEq/L KCl. Serial electrolytes at 2-hourly intervals show: K+ at admission 4.8 → at 2h 3.8 → at 4h 3.1 mEq/L. Blood glucose is 310 mg/dL, pH has improved to 7.28. The patient's ECG now shows T-wave flattening with U waves in precordial leads. What do you do?
Analysis: The K+ trend is alarming: 4.8 → 3.8 → 3.1 mEq/L over 4 hours of insulin infusion, now with ECG evidence of hypokalaemia (T-wave flattening, U waves). Immediate action: (1) Increase IV K+ replacement to 40 mEq/hour (maximum safe peripheral rate); (2) Slow or pause insulin infusion until K+ is ≥3.5 mEq/L — this is the same K+ rule applied during initial assessment, but it must also be applied mid-treatment; (3) Continuous cardiac monitoring; (4) Recheck K+ in 1 hour. The pH is still mildly acidotic (7.28) but improving, so insulin can be resumed once K+ is corrected. The ECG changes are a warning — do not dismiss them as expected electrolyte variation.
Scenario B — DKA in Pregnancy:
A 26-year-old G2P1 woman at 28 weeks gestation with T1DM presents with DKA (glucose 310 mg/dL, pH 7.21, BHB 5.2 mmol/L). She has been vomiting for 24 hours. Why does DKA present at a lower glucose threshold in pregnancy, and what is the priority in management?
Analysis: In pregnancy, several factors lower the DKA threshold: (1) normal physiological respiratory alkalosis lowers baseline bicarbonate, so a smaller ketone load produces a proportionally greater pH change; (2) insulin requirements increase dramatically in the second and third trimester (by 50–100% compared to pre-pregnancy) due to placental hormones (hCG, progesterone, human placental lactogen) causing insulin resistance — a patient who missed even one dose may decompensate rapidly; (3) vomiting reduces carbohydrate intake, while nausea may have reduced insulin doses. DKA in pregnancy is a fetal emergency as well as a maternal one — fetal mortality is 9–36% in published series. Management priority: aggressive maternal resuscitation (fluids, insulin, K+ as per standard protocol) takes precedence — fetal outcome is directly dependent on maternal acid-base correction. Involve obstetrics and intensive care immediately. Monitor fetal heart rate continuously.
Scenario C — Mixed DKA-HHS:
An 80-year-old man with T2DM is admitted with glucose 680 mg/dL, osmolality 334 mOsm/kg, pH 7.24, bicarbonate 12 mEq/L, ketones (blood BHB) 4.1 mmol/L. He has a 5-day history of worsening confusion and vomiting. How do you classify this presentation and how does it affect management?
Analysis: This patient has a mixed DKA-HHS picture — both hyperglycaemia with ketonaemia/acidosis (DKA criteria: pH <7.3, BHB >3.0 mmol/L) AND features of HHS (glucose >600, osmolality >320, prolonged history). Approximately 30% of hyperglycaemic emergencies have mixed features. Management: follow DKA protocol for the acidosis and ketosis (IV normal saline, insulin infusion, K+ rule); but also apply HHS principles for fluid management (switch to half-normal saline once volume-replete and sodium is stable, to correct the free water deficit and avoid hypernatraemia); anticoagulate (HHS component); monitor osmolality and ensure it does not fall too rapidly. This scenario illustrates that the DKA/HHS categorisation is clinically useful but not exclusive — mixed cases require management elements from both protocols.
Diabetic Emergencies: Bedside Decision Card
CLINICAL PEARL
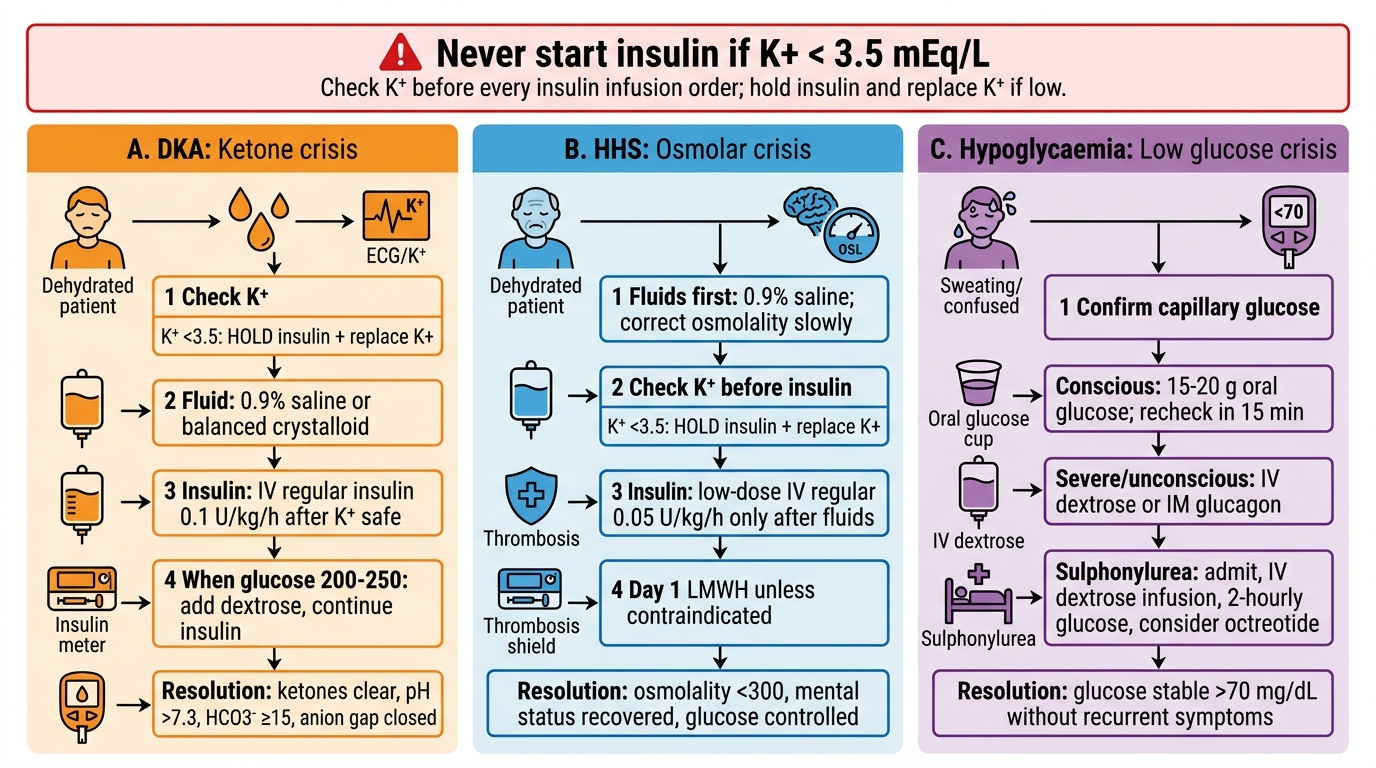
Four non-negotiable rules for diabetic emergencies that must be memorised:
- K+ <3.5 mEq/L = HOLD insulin. This is the most important safety rule in DKA management. Starting insulin with a low K+ can cause fatal cardiac arrhythmias within minutes. Check K+ before every insulin infusion order. Apply the same rule mid-treatment if K+ falls below 3.5.
- In DKA, stop insulin when KETONES clear — not when glucose normalises. When blood glucose falls to 200–250 mg/dL, add dextrose to IV fluids and continue insulin infusion at the same rate. Stopping insulin because glucose is 'normal' while BHB remains elevated causes ketosis to rebound (J-shaped glucose-BHB resolution curves).
- HHS has the highest VTE risk of any medical admission. Start LMWH on day one unless contraindicated. HHS-associated DVT and PE cause a significant fraction of HHS deaths.
- Sulphonylurea hypoglycaemia must be hospitalised. A single correction of blood glucose with juice and sending the patient home is a potentially fatal management error. Glibenclamide and other long-acting SUs cause recurrent hypoglycaemia for 12–24+ hours — the patient needs IV dextrose infusion and 2-hourly monitoring until the drug is metabolised.