Page 5 of 21
IM13.7-10 | Cancer Clinical Evaluation — SDL Guide (Part 2)
Rectal Examination Technique
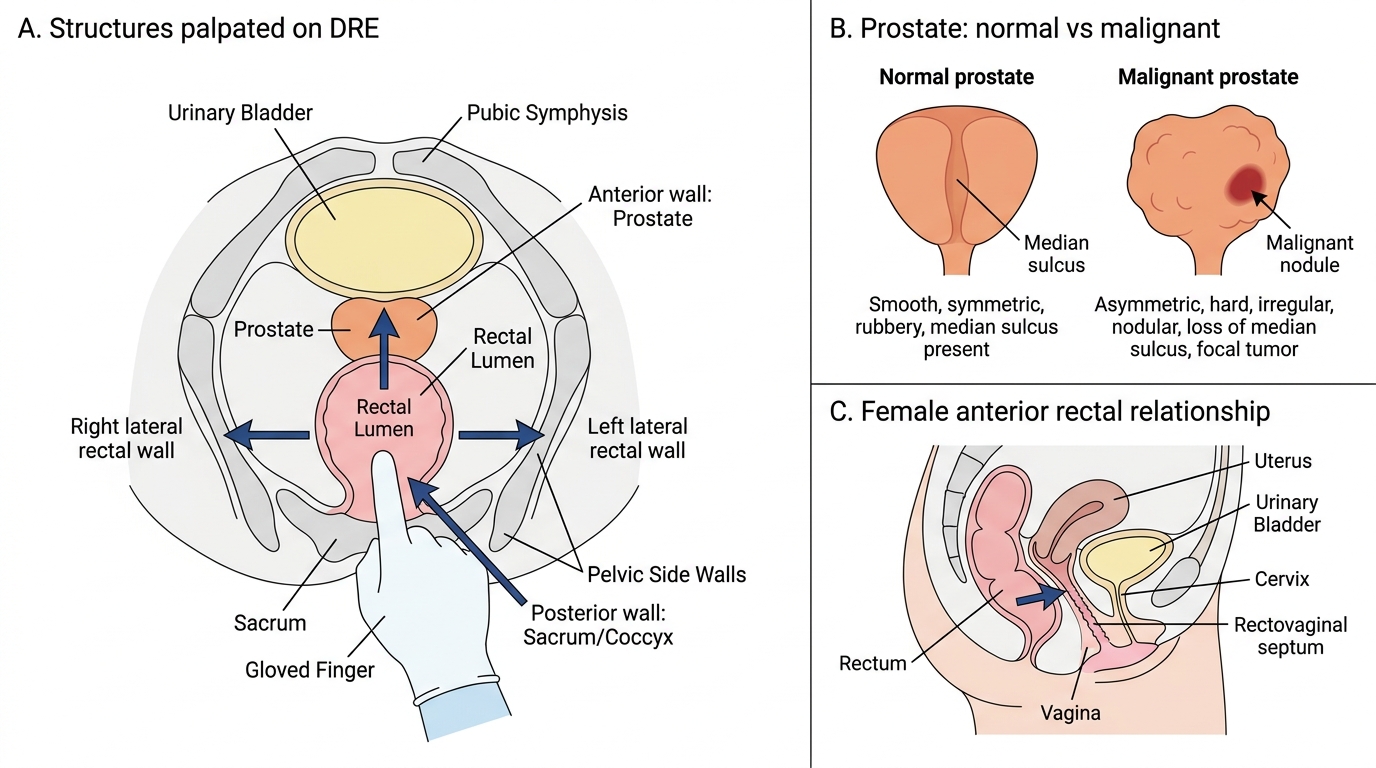
Digital rectal examination (DRE) is one of the most information-dense examinations in clinical medicine — it allows assessment of the anal canal, rectal mucosa, the posterior rectal wall to approximately 8–10 cm from the anal verge, the prostate gland (anteriorly), the rectovaginal septum and cervix (in women), and detects blood, mucus, or mass lesions. The NMC competency IM13.9 expects proficiency on a mannequin.
Equipment required: non-sterile gloves, lubricant gel, absorbent paper or towel. Position: the left lateral (Sims') position is standard — the patient lies on the left side, hips and knees flexed, with the buttocks at the edge of the examination table. The dorsal lithotomy position or knee-chest position may alternatively be used. Verbal explanation and consent are essential before proceeding.
Inspection first (before any digital insertion): inspect the perianal skin for skin tags, haemorrhoidal prolapse, anal fissure (look at 6 and 12 o'clock — midline positions), perianal abscess, fistula openings, or ulceration (anal cancer presents as an ulcer or exophytic mass at the anal margin — examine carefully before proceeding). Ask the patient to strain gently — prolapsing haemorrhoids or early rectal prolapse may become visible.
Digital insertion: apply generous lubricant to the gloved index finger. Apply the finger pad to the anal margin at the 6 o'clock position and maintain gentle constant pressure — the external sphincter will relax after 15–20 seconds. Do NOT push against resistance. Once inserted, rotate the finger through 360 degrees, palpating the rectal wall systematically (anterior, posterior, left lateral, right lateral). Note: tone of the external sphincter (lax = neurological cause, e.g., cauda equina syndrome; hypertonic and tender = anal fissure); any nodule, mass, or induration in the rectal wall; consistency and surface of the prostate anteriorly (normal = smooth, rubbery, median sulcus palpable, non-tender; malignant = hard, irregular, nodular, loss of median sulcus — but benign prostatic hyperplasia gives a smoothly enlarged gland); any boggy fluctuance suggesting abscess. On withdrawal, inspect the glove for: blood (rectal cancer, haemorrhoids, polyp), mucus (mucus-secreting adenocarcinoma of the rectum, inflammatory bowel disease), or stool colour (melaena = upper GI bleeding if tarry-black; haematochezia = left colon or rectal bleeding if bright red).
IMPORTANT CLINICAL POINTS: DRE has a sensitivity of only 50–60% for rectal cancer (tumours not reached by the examining finger are missed; colonoscopy or flexible sigmoidoscopy is definitive). Prostate-specific antigen (PSA) should be checked BEFORE DRE, as the examination transiently elevates PSA by mechanical manipulation. In a patient with known or suspected prostate cancer, document whether the median sulcus is palpable, whether the lateral lobes are symmetrical, and whether the upper margin of the gland is reachable (a non-reachable upper margin suggests extra-prostatic extension).
Digital Rectal Examination: Palpable Pelvic Structures and Prostate Cancer Findings
SELF-CHECK
During digital rectal examination of a 65-year-old man presenting with hesitancy and nocturia, you palpate the prostate and find an irregular, hard, nodular mass with loss of the median sulcus. What is the most concerning interpretation of this finding?
A. Benign prostatic hyperplasia (BPH)
B. Acute prostatitis
C. Prostate cancer
D. Prostatic abscess
Reveal Answer
Answer: C. Prostate cancer
An irregular, hard, nodular prostate with loss of the median sulcus is the classic DRE finding of prostate cancer. BPH produces a uniformly enlarged, smooth, rubbery gland with a preserved or widened median sulcus. Acute prostatitis produces a warm, exquisitely tender, boggy gland (examination should be gentle to avoid bacteraemia). Prostatic abscess produces fluctuance. Hardness and irregularity strongly suggest malignancy; this finding mandates serum PSA measurement and referral for transrectal ultrasound-guided biopsy.
Cervical Examination and Pap Smear Technique
Cervical examination with Pap smear collection is a procedural skill with dual clinical purposes: (1) gynaecological screening for cervical cancer precursors (cervical intraepithelial neoplasia, CIN) and (2) investigation of symptomatic women with intermenstrual or postcoital bleeding, vaginal discharge, or visible cervical lesion. NMC competency IM13.9 requires competent demonstration on a mannequin.
Equipment: disposable cusco (bivalve) speculum, adequate lighting, cervical brush (Cervex-Brush or Ayre's spatula and endocervical brush), fixative spray (for conventional Pap smear) or liquid-based cytology (LBC) vial, microscope slide. Position: dorsal lithotomy — patient supine, hips and knees flexed, heels in stirrups or feet flat, buttocks at the edge of the table. Verbal consent and chaperone are mandatory.
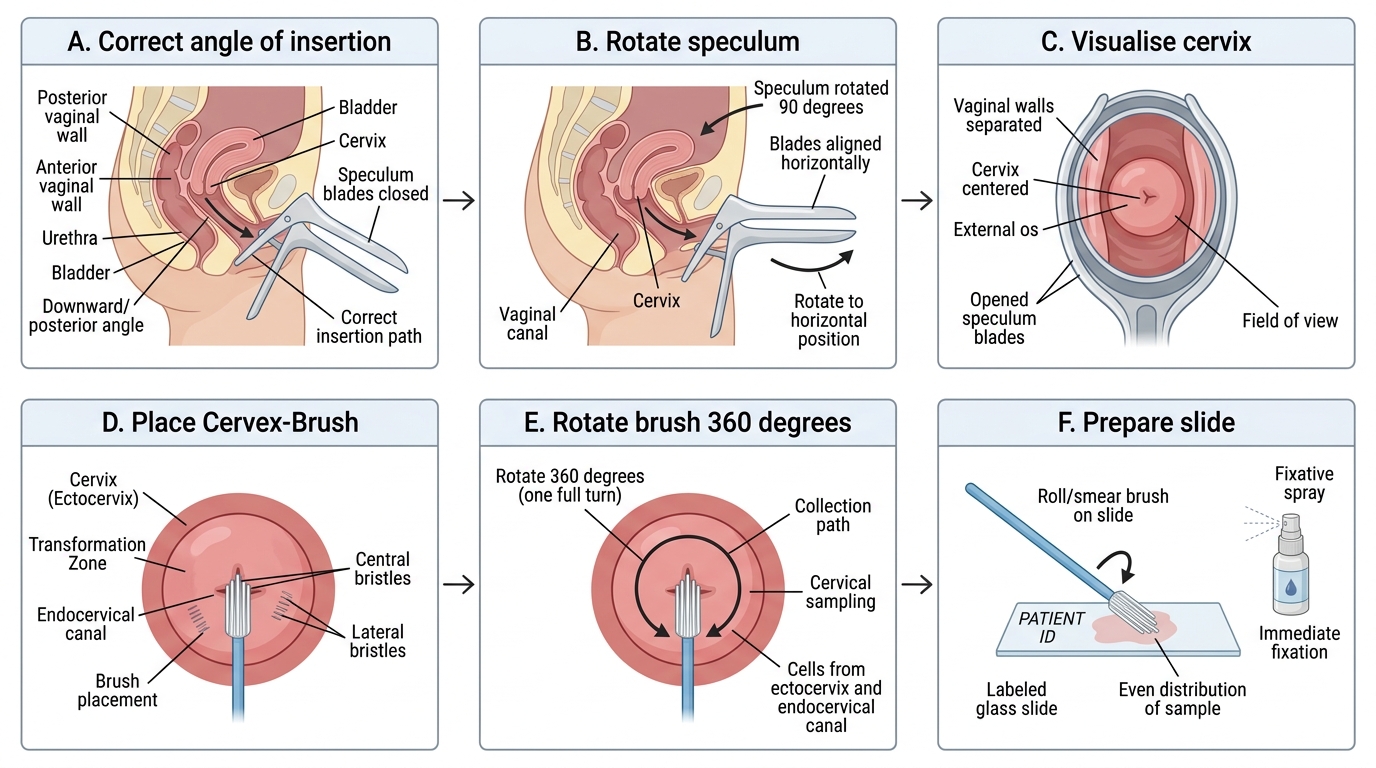
Speculum examination: warm the speculum blade with warm water (do not use lubricant — it interferes with cytology). Insert the speculum with the blades closed in the vertical (sagittal) plane, tilting slightly posteriorly to follow the vaginal axis (directed toward the sacrum, not the bladder). Rotate to the horizontal plane as you advance past the introitus, and open the blades to visualise the cervix. Lock the speculum open. Systematically inspect: the ectocervix (squamous epithelium — normally smooth and pink; epithelial disruption, ulceration, exophytic or friable tissue, or contact bleeding on speculum insertion all suggest malignancy or significant CIN); the transformation zone (the squamo-columnar junction — the area of greatest CIN and cancer risk, where columnar epithelium undergoes squamous metaplasia; visible as an area of acetowhite change after VIA or as a demarcated zone on colposcopy); any discharge in the vaginal vault; vaginal walls for obvious lesions.
Pap smear collection: use a cervical brush (Cervex-Brush) — insert the central bristles into the endocervical canal and rotate 5 times in a clockwise direction to sample both the ectocervix and the endocervical canal simultaneously. For conventional cytology, roll the brush onto a glass slide in a single stroke (do not swipe back and forth — this damages cells), then immediately fix with spray fixative within 20–30 seconds to prevent air drying artefact (a common cause of inadequate smears). For liquid-based cytology (LBC), swirl or rinse the brush into the LBC vial. Label the slide/vial with: patient name, date of birth, date of collection, and the location of sampling (ectocervical vs. combined). Document the indication and any abnormal clinical findings.
After speculum withdrawal, perform bimanual vaginal examination: two gloved fingers in the vagina, other hand on the lower abdomen. Assess the cervix (mobility — a fixed, immobile, hard cervix suggests parametrial invasion in advanced cervical cancer), uterus (size, position, consistency, mobility, tenderness), and adnexa (palpate each fornix for mass, tenderness, or nodularity). In a woman with cervical cancer, parametrial nodularity ('barrel-shaped' cervix or thickened paracervical tissues) indicates Stage IIB or greater disease.
Speculum Insertion and Pap Smear Collection
Generating a Differential Diagnosis in Oncology
Generating a differential diagnosis in oncology requires integrating the history and examination findings into a systematic clinical reasoning framework. The final-year student must move beyond memorised lists and instead apply structured diagnostic reasoning: the VINDICATE or MIDNIGHTS framework adapted for oncological thinking, or the pragmatic site-age-sex-risk factor matrix.
The practical approach at the bedside follows three iterative steps: (1) Identify the presenting syndrome — lump, bleeding, change in organ function, constitutional symptoms, or an incidental finding; (2) Apply epidemiological priors — for a 55-year-old male smoker with haemoptysis, the pre-test probability for lung cancer is very high; for a 25-year-old non-smoker with haemoptysis, infectious causes (TB, bronchiectasis) dominate; (3) Narrow by examination pattern — the examination findings either corroborate the leading hypothesis or introduce a new dominant clue (e.g., the Virchow's node that shifts the differential from a lung primary to an abdominal primary).
For each presenting complaint, the clinician should mentally work through: primary tumour site (what are the 3–5 most common cancers at this anatomical location?), benign mimics (a hard breast lump is cancer until proven otherwise but fat necrosis, fibroadenoma, and abscess are on the list), inflammatory conditions (TB lymphadenitis is the most common cause of cervical lymphadenopathy in India — always include it before malignancy in young patients from endemic backgrounds), and non-oncological systemic diseases (hypothyroidism presenting as weight gain vs. cachexia in cancer; SVC syndrome from a mediastinal goitre vs. from lung cancer).
Key differential diagnostic patterns for common presentations:
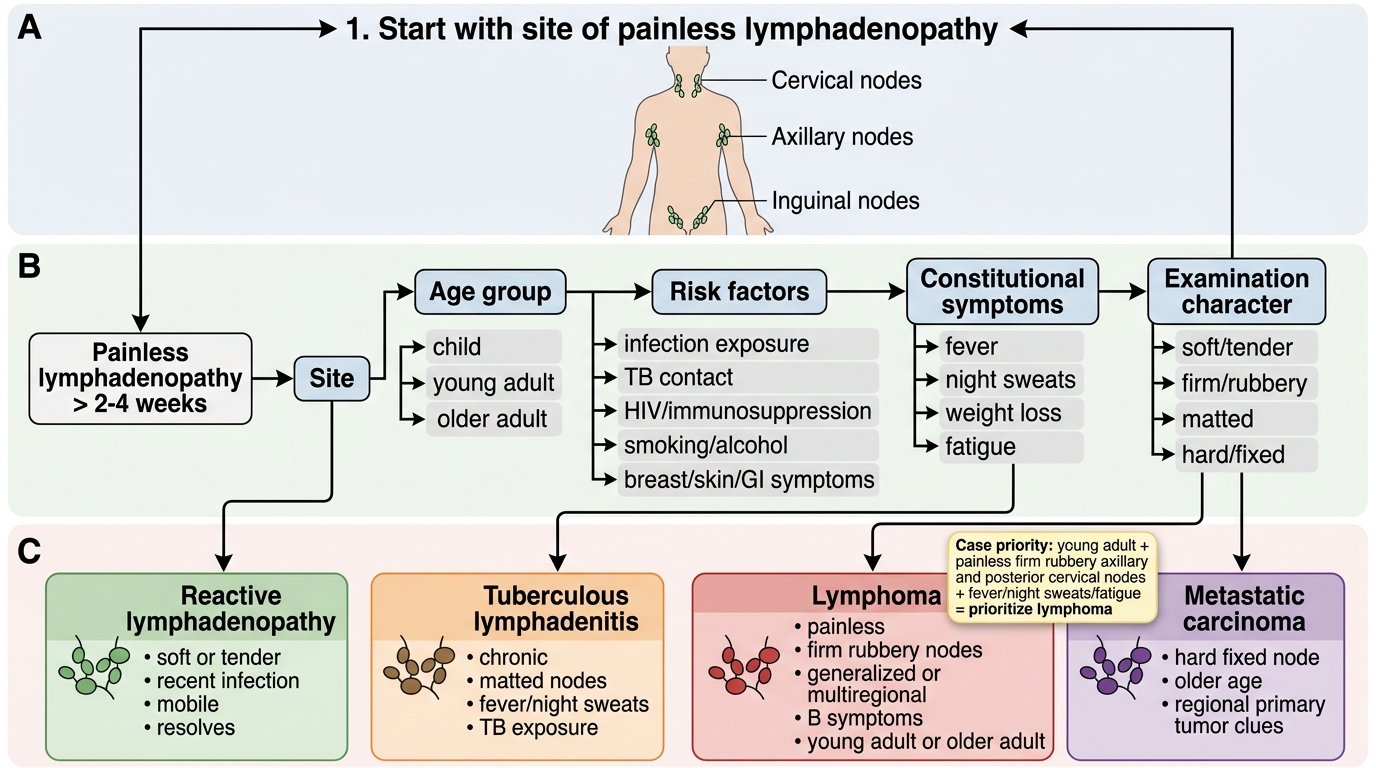
- Painless neck swelling: reactive lymphadenopathy (URTI) vs. TB lymphadenitis vs. lymphoma vs. metastatic carcinoma (from oral cavity, thyroid, nasopharynx, stomach — depending on nodal level)
- Haemoptysis: TB (most common in India), bronchiectasis, lung cancer, pulmonary embolism, mitral stenosis (haemoptysis from pulmonary hypertension)
- Altered bowel habit + rectal bleeding: colorectal cancer vs. inflammatory bowel disease vs. haemorrhoids vs. polyps — always investigate to exclude cancer in a patient >40 years
- Unilateral pleural effusion: malignant effusion (lung cancer, breast cancer, lymphoma, mesothelioma) vs. parapneumonic effusion vs. TB pleural effusion — exudate on Light's criteria requires cytology and pleural biopsy
- Unexplained weight loss >10% body weight over 6 months: malignancy in any organ system, TB, HIV, hyperthyroidism, uncontrolled diabetes, severe depression — a systematic review of all organ systems is required
Identifying the most likely diagnosis requires weighting the differential by probability given ALL the available data. A 60-year-old male with 50-pack-year smoking history, weight loss, and a right hilar mass on CXR has a >90% pre-test probability of lung cancer — the differential still includes TB and sarcoidosis, but the clinical approach must prioritise tissue diagnosis of the dominant hypothesis first.
Approach to Painless Lymphadenopathy
SELF-CHECK
A 28-year-old woman presents with a 6-week history of painless right axillary swelling. She has been feeling fatigued with mild fever and night sweats for the past 4 weeks. On examination, you find a 3 cm firm, non-tender, rubbery lymph node in the right axilla and two smaller similar nodes in the right posterior cervical chain. There is no skin lesion, breast mass, or hand/arm pathology. What is the MOST likely diagnosis to prioritise in your differential?
A. Reactive lymphadenopathy from a viral upper respiratory infection
B. Lymphoma (Hodgkin or non-Hodgkin)
C. Metastatic breast cancer
D. Cat scratch disease (Bartonella henselae infection)
Reveal Answer
Answer: B. Lymphoma (Hodgkin or non-Hodgkin)
The combination of painless, firm, rubbery bilateral lymphadenopathy (axillary + posterior cervical), constitutional B symptoms (fever, night sweats, fatigue), and a young adult presentation is the classic presentation of lymphoma — particularly Hodgkin lymphoma in this age group. Reactive lymphadenopathy is typically tender and resolves quickly. Metastatic breast cancer would require a primary breast lesion to be found. Cat scratch disease produces tender axillary nodes after cat exposure. The B symptoms (fever, drenching night sweats, weight loss >10%) are part of the Ann Arbor staging system and have important prognostic implications in lymphoma — their presence upgrades from A to B (e.g., Stage IIA vs. Stage IIB).