Page 6 of 21
IM13.7-10 | Cancer Clinical Evaluation — SDL Guide (Part 3)
Applied Practice: Integrating History, Examination, and Differential
Clinical evaluation in oncology is only meaningful when its outputs drive the next decision — the differential diagnosis must be operationalised into a management plan. In this applied practice section, we work through two complete clinical evaluation cases to consolidate the skills taught in this module.
Case 1: Breast lump in a 48-year-old woman
History: Ms. K presents with a 3-month history of a lump in her right breast noticed while bathing. She describes it as painless, non-tender, and 'growing slightly'. She has no nipple discharge, no skin changes noticed, and no B symptoms. Family history: her mother had breast cancer at age 56. She is nulliparous, used the combined OCP for 8 years, and had her first period aged 11. Menopause status: pre-menopausal.
Examination: Inspection reveals subtle skin dimpling over the right upper outer quadrant at the 2 o'clock position. Palpation reveals a 2.5 cm hard, irregular, non-tender mass at 2 o'clock, 4 cm from the nipple, with fixation to the overlying skin. The nipple is deviated slightly upward. No nipple discharge on expression. Axilla: two firm, non-tender, 1 cm lymph nodes in the right anterior axillary group. Contralateral breast and axilla normal. No supraclavicular lymphadenopathy.
Differential diagnosis and most likely diagnosis: The triple assessment for breast disease integrates clinical examination (E), imaging (I), and histopathology (H) — known as the triple assessment or triple test. On clinical assessment alone: hard, irregular, skin-tethered, axillary-node-positive lump in a 48-year-old with family history and early menarche = carcinoma of the breast is the leading diagnosis with high pre-test probability. Differential includes: fibroadenoma (but fibroadenomas are typically mobile, smooth, and non-tender — 'breast mouse'), fat necrosis (post-traumatic, often with skin tethering but history of trauma), phyllodes tumour, abscess (tender, febrile). The skin tethering and axillary nodal involvement make carcinoma the most likely diagnosis. Next step: bilateral mammography + USS + core biopsy (to complete triple assessment).
Case 2: Change in bowel habit in a 62-year-old man
History: Mr. D reports 4 months of increasing constipation alternating with loose stools, a sense of incomplete evacuation after defecation (tenesmus), and intermittent bright red blood mixed in the stool. He has lost 7 kg in weight. He has no family history of colorectal cancer, no prior colonoscopy, and has not been screened. He is a non-smoker.
Examination: Pallor (mucosal). Abdomen: mild left iliac fossa tenderness on palpation; a vaguely palpable non-tender mass in the left iliac fossa. No hepatomegaly. Digital rectal examination: normal sphincter tone, a hard, irregular mass is palpable on the posterior wall of the rectum at approximately 6 cm from the anal verge, with mucosal irregularity and contact bleeding on the examining finger. Glove stained with dark red blood on withdrawal.
Differential and most likely diagnosis: Hard, irregular, friable rectal mass with PR blood, weight loss, altered bowel habit in a 62-year-old = rectal adenocarcinoma is the leading diagnosis. Differential includes: villous adenoma (soft, secretory, causes mucorrhoea), large haemorrhoid (soft, prolapsing), Crohn's disease (granulomatous mass, but usually with other inflammatory features), or a retrorectal mass. Clinical examination has already reached the mass directly — the diagnosis is almost certain, pending histopathology from colonoscopy-directed biopsy. Next step: CT chest/abdomen/pelvis (staging), CEA level (baseline), colonoscopy + biopsy, MRI rectum (for local staging — T and N stage).
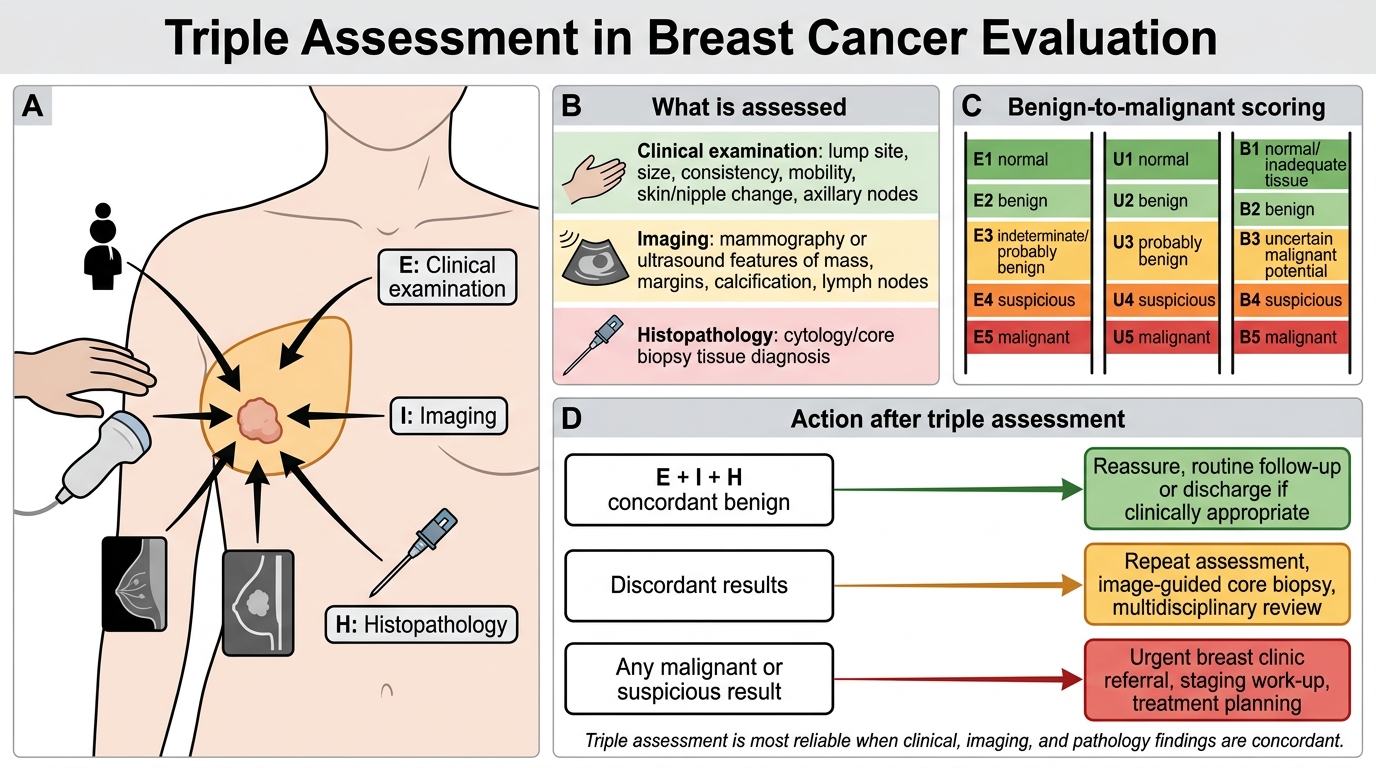
Triple Assessment in Breast Cancer Evaluation
Self-Assessment: Clinical Evaluation Competencies
This section consolidates your self-assessment of the clinical evaluation skills covered in this module. The NMC competencies IM13.7–13.10 span from history-taking (K) to physical examination (SH) — meaning both knowledge recall and practical skill performance are assessed. The following self-assessment scenarios are designed to reinforce reasoning and identify gaps before your clinical skills examination.
Self-assessment checklist — breast examination:
Can you describe and perform: (1) three inspection positions and what each reveals; (2) the correct palpation technique (flat of fingers, systematic pattern, tail of Spence); (3) the six descriptors of a breast lump (site, size, shape, surface, consistency, mobility); (4) the four components of axillary node assessment; (5) the triple assessment concept (E + I + H)?
Self-assessment checklist — rectal examination:
Can you describe and perform: (1) correct patient positioning (Sims'); (2) perianal inspection for fissure/fistula/mass; (3) systematic 360-degree palpation of the rectal wall; (4) prostate characterisation on DRE (normal vs. BPH vs. malignant); (5) interpretation of glove findings (blood, mucus, stool character)?
Self-assessment checklist — Pap smear:
Can you describe and perform: (1) speculum selection, warming, and insertion technique; (2) correct brush placement and rotation (5 clockwise turns into endocervical canal); (3) immediate fixation of conventional smear (within 20–30 sec of spreading); (4) visual inspection of the cervix for transformation zone and abnormal lesions; (5) bimanual examination to assess cervical mobility and uterine size?
Rapid review questions:
- An ECOG performance status of 3 means the patient is confined to bed or chair for more than 50% of waking hours but is capable of some self-care. Would this patient typically be offered full-dose cytotoxic chemotherapy? (Answer: No — ECOG PS ≥2 is typically the threshold for reduced-dose or supportive-only approaches; PS 3–4 patients are generally managed with best supportive care.)
- A patient has a 35 pack-year tobacco history. She smoked 20 cigarettes per day for 25 years. Is this calculation correct? (Answer: 20 cigarettes/day ÷ 20 = 1 pack/day × 25 years = 25 pack-years — not 35. A 35 pack-year history requires either more cigarettes per day or a longer duration.)
- You palpate a hard, fixed, non-tender, 3 cm supraclavicular lymph node on the LEFT side. You find no mass on breast or neck examination. Where is the primary tumour most likely to be? (Answer: The left supraclavicular fossa receives lymphatic drainage from the entire abdomen and pelvis via the thoracic duct — the most common primary sites are stomach, pancreas, colon, or other upper abdominal organs. However, left lung/mediastinal tumours also drain here.)
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
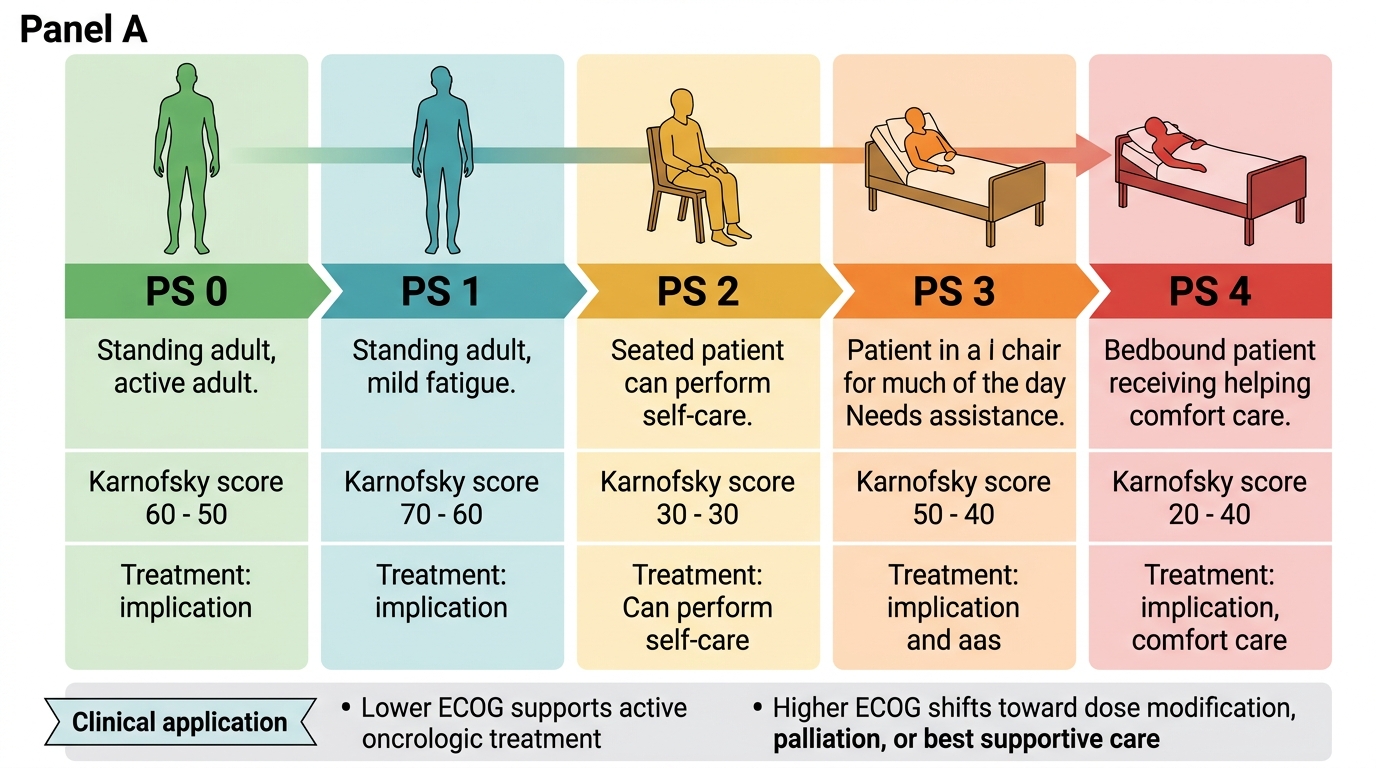
ECOG Performance Status Scale
CLINICAL PEARL
Two high-yield clinical pearls for cancer clinical evaluation:
First, the triple assessment principle in breast lumps: never rely on clinical examination alone to reassure a patient that a breast lump is benign. The triple assessment (clinical E + imaging I + histopathology H) requires concordance from all three components for a benign verdict. A clinically suspicious (E4 or E5) lump with a 'probably benign' ultrasound (U3) result should still be biopsied — discordance mandates tissue diagnosis. Hundreds of cancers are missed each year by clinicians who discharge patients on the basis of a single negative test.
Second, tenesmus is a red-flag symptom of rectal cancer: the sensation of incomplete rectal emptying after defecation — caused by a rectal mass maintaining the urge-to-defecate reflex — is a specific indicator that a mass is present in the rectum or rectosigmoid junction. Any patient over 40 presenting with tenesmus, especially combined with rectal bleeding, change in stool calibre (ribbon stools from partial obstruction), or weight loss, must be investigated for colorectal malignancy with colonoscopy.