Page 8 of 21
IM13.11-12 | Cancer Diagnostic Testing — SDL Guide
Learning Objectives
- Order and interpret diagnostic tests in a cancer patient, including CBC, stool occult blood, and prostate-specific antigen (PSA)
- Describe the indications and interpret the results of chest X-ray, mammogram, skin and tissue biopsies, and tumour markers used in common cancers
INSTRUCTIONS
Accurate cancer diagnosis requires a systematic approach to laboratory, imaging, and tissue investigations — each selected and interpreted in the context of the clinical question. This module teaches you to choose the right test, understand its limitations, and apply results to clinical decision-making.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 69 — Diagnosis and Staging of Cancer (textbook)
- API Textbook of Medicine, 10th ed., Cancer Diagnostics section (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 11 — Investigation of the Cancer Patient (textbook)
- WHO Classification of Tumours (Blue Book series), 5th edition (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are reviewing laboratory results for three patients admitted overnight. Patient A: a 65-year-old man with a haemoglobin of 8.2 g/dL, MCV 72 fL, and a peripheral blood film showing hypochromic microcytic red cells — his stool occult blood test is strongly positive. Patient B: a 70-year-old man referred with a PSA of 18 ng/mL and a hard, nodular prostate on DRE. Patient C: a 55-year-old woman with a persistent right upper lobe opacity on chest X-ray requested for a 6-week cough with haemoptysis; she has a 40 pack-year smoking history. Three diagnostic questions, three different test batteries, three different interpretive frameworks. By the end of this module, you will know not just what these results mean, but how to act on them — what to order next, when biopsy is required, and what the results do and do not rule in or out.
WHY THIS MATTERS
Diagnostic testing is the bridge between clinical suspicion and confirmed diagnosis. Over-investigation wastes resources and causes patient anxiety; under-investigation delays diagnosis and reduces survival. NMC competencies IM13.11 and IM13.12 require you to operate at the KH (Knowledge with Understanding and Application) level — meaning you must not only know which tests to order but be able to interpret results in clinical context, understand their limitations, and know when to escalate to tissue biopsy. Every investigation discussed in this module is accessible at the district hospital level, making these skills directly applicable across all Indian healthcare settings.
RECALL
Recall your prior knowledge of laboratory haematology: the components of the complete blood count (CBC/FBC), the morphological features of iron-deficiency anaemia (microcytic, hypochromic, elevated RDW, low ferritin), and the leucoerythroblastic blood film that signals bone marrow infiltration (circulating nucleated red cells, teardrop cells, and immature white cells). From radiology basics, recall how to assess an opacity on a CXR — location, density, shape, margins, associated features. From biochemistry, recall that PSA is a serine protease produced by prostate epithelium and that it is prostate-specific, not cancer-specific — BPH, prostatitis, and DRE all elevate PSA. These foundations prepare you for the interpretive nuances this module builds.
Complete Blood Count, Stool Occult Blood, and PSA Testing
The complete blood count (CBC) is often the first diagnostic clue pointing toward a haematological or solid malignancy, even when it was ordered for an unrelated indication. Interpreting the CBC with a cancer-specific lens requires attention to each cell line and their morphological context.
Haemoglobin and red cell indices: iron-deficiency anaemia (Hb <13 g/dL male, <12 g/dL female; MCV <80 fL; MCH <27 pg; elevated RDW) in a patient over 40 years without an obvious dietary cause mandates investigation to exclude colorectal or gastric cancer as a source of chronic occult gastrointestinal blood loss. The hypochromic, microcytic pattern in such a patient is presumed to be from GI tract cancer until endoscopy proves otherwise. Conversely, a normocytic anaemia with elevated reticulocyte count suggests haemolysis (possible in lymphoma, autoimmune haemolytic anaemia in CLL); a normocytic, normochromic anaemia with a leucoerythroblastic blood film (circulating nucleated red cells + immature white cells + teardrops + leukoerythroblasts) is the hallmark of bone marrow infiltration — by metastatic carcinoma (breast, lung, prostate, stomach), lymphoma, leukaemia, or myelofibrosis; this requires urgent bone marrow biopsy.
White cell count and differential: a markedly elevated total WBC (>100 × 10⁹/L) suggests a myeloproliferative disorder or acute/chronic leukaemia. A left shift (band forms, metamyelocytes, myelocytes in the peripheral blood) without infection may indicate a leukaemoid reaction from solid tumour metastases. Lymphocytosis with small, mature lymphocytes and 'smear cells' (Gumprecht shadows) on the film is the classical finding of chronic lymphocytic leukaemia (CLL). Blast cells in the peripheral blood (undifferentiated cells with prominent nucleoli, high nuclear-to-cytoplasm ratio, and Auer rods — pathognomonic for AML) signal acute leukaemia requiring urgent haematology referral and bone marrow aspiration.
Platelet count: thrombocytopenia in cancer may result from bone marrow infiltration, hypersplenism (in lymphoma with splenomegaly), autoimmune destruction (ITP secondary to CLL), or chemotherapy-induced myelosuppression. Paradoxically, thrombocytosis (reactive thrombocythaemia) occurs in some solid tumours — particularly lung, ovarian, and colorectal cancer — as a paraneoplastic phenomenon mediated by tumour-derived interleukin-6 driving thrombopoietin production.
Stool occult blood testing (FOBT/FIT): the faecal immunochemical test (FIT) has replaced the older guaiac-based FOBT as the preferred method due to its higher specificity for human haemoglobin and the absence of dietary restrictions. FIT detects haemoglobin in stool from the lower gastrointestinal tract. A positive FIT result mandates colonoscopy — the sensitivity of FIT for colorectal cancer is approximately 75–80% and for advanced adenoma is approximately 25–35%, meaning a negative test does NOT exclude colorectal cancer in a symptomatic patient. In a symptomatic patient with rectal bleeding or iron-deficiency anaemia, proceed directly to colonoscopy without waiting for an FOBT result. FIT screening is most valuable in the asymptomatic screening population; it is not a replacement for colonoscopy in symptomatic patients. Factors that cause false-positive FOBT (guaiac-based): red meat, certain vegetables (peroxidase activity); FIT is human haemoglobin-specific and avoids these dietary false-positives.
Prostate-specific antigen (PSA): PSA is a serine protease produced by prostate epithelial cells; it liquefies seminal coagulum. Its concentration in serum is elevated in prostate cancer but also in benign prostatic hyperplasia (BPH), prostatitis, urinary tract infection, and urological instrumentation (including DRE, which transiently elevates PSA by ~0.4 ng/mL — therefore, PSA must always be drawn BEFORE DRE). Key reference values and their clinical interpretation:
| PSA (ng/mL) | Interpretation | Action |
|---|---|---|
| <4.0 | Normal range (conventional) | Routine follow-up; repeat if symptoms present |
| 4.0–10.0 | 'Grey zone' — BPH and early cancer overlap | TRUS-guided biopsy if DRE abnormal or risk factors |
| >10.0 | High probability of cancer | TRUS-guided biopsy regardless of DRE |
| >100 | Very high — likely metastatic disease | Isotope bone scan + biopsy for staging |
Important interpretive caveats: (1) PSA velocity (rate of rise in ng/mL per year) >0.75 ng/mL/year carries high specificity for cancer even within the grey zone; (2) PSA density (PSA ÷ prostate volume) >0.15 ng/mL/cm³ suggests cancer rather than BPH as the cause of elevation; (3) free PSA ratio (free/total PSA) <10–15% is associated with cancer, while >25% suggests BPH; (4) 5-alpha-reductase inhibitors (finasteride, dutasteride) halve PSA — multiply the measured PSA by 2 when interpreting in a patient on these medications.
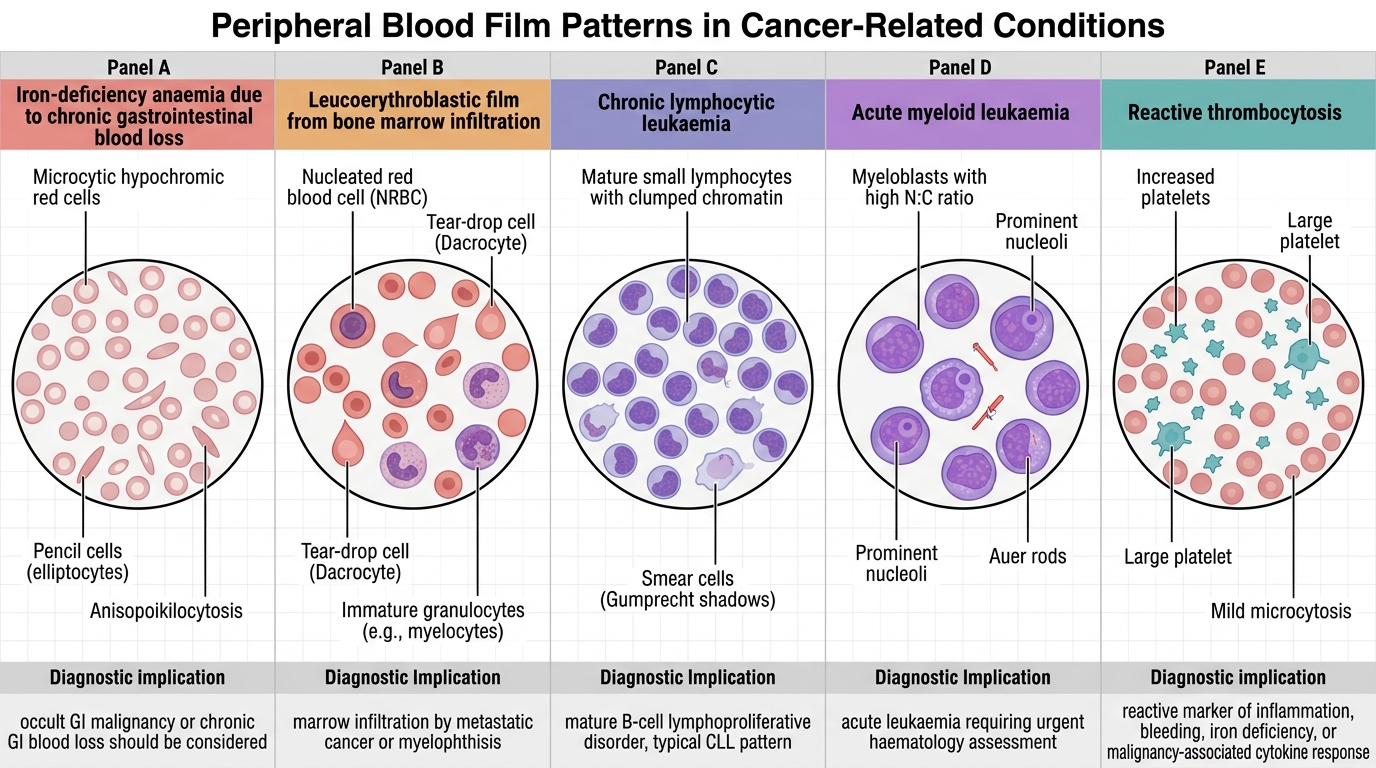
Peripheral Blood Film Clues in Cancer-Related Conditions
SELF-CHECK
A 72-year-old man with a PSA of 24 ng/mL had his PSA drawn 30 minutes AFTER a digital rectal examination. His prostate on DRE was enlarged, smooth, and rubbery with a preserved median sulcus. What is the most appropriate interpretation and immediate next step?
A. PSA is elevated due to DRE manipulation — repeat PSA in 4–6 weeks before deciding on biopsy
B. PSA >10 ng/mL always indicates prostate cancer — arrange biopsy urgently
C. PSA is within normal limits for a 72-year-old — no action needed
D. The smooth DRE rules out prostate cancer — reassure and discharge
Reveal Answer
Answer: A. PSA is elevated due to DRE manipulation — repeat PSA in 4–6 weeks before deciding on biopsy
PSA must be drawn BEFORE digital rectal examination because DRE transiently elevates PSA. A PSA of 24 ng/mL drawn post-DRE may be falsely elevated. The DRE findings (smooth, rubbery, preserved median sulcus) suggest BPH rather than cancer. The correct approach is to repeat PSA in 4–6 weeks, drawn before any urological examination. If the PSA remains >10 ng/mL on repeat, transrectal ultrasound-guided biopsy should be arranged. Arranging urgent biopsy on the basis of a post-DRE PSA would be premature. However, if the repeat PSA remains elevated, action is clearly required — benign appearance on DRE does not exclude malignancy.
Chest X-Ray Interpretation in Cancer
The chest X-ray (CXR) is the first-line imaging investigation for respiratory symptoms and a critical component of cancer staging across multiple tumour types. Systematic interpretation using a structured approach prevents missed findings — use the mnemonic ABCDE (Airway, Breathing/lung fields, Cardiac, Diaphragm/abdomen, Everything else/bones, extras) or RIPE (Review areas, Inflation, Parenchyma, Extras).
For cancer-specific CXR interpretation, the key findings and their differential diagnoses are:
Solitary pulmonary nodule (SPN): an opacity <3 cm in diameter, surrounded by lung, with no associated atelectasis or lymphadenopathy. The probability of malignancy depends on size (>8 mm requires investigation), age, smoking history, and morphology. Features strongly suggesting malignancy: spiculated margins (corona radiata appearance — spicules represent local lymphatic and vascular invasion), lobulated border, upper lobe location, and rapid growth. Features suggesting benign aetiology: central calcification (popcorn calcification = hamartoma; diffuse or stippled calcification = granuloma from old TB; laminated calcification = old infection), smooth margins, and slow or no growth over 2 years. Any spiculated nodule in a smoker >50 years is lung cancer until proven otherwise on CT.
Pulmonary mass: an opacity >3 cm — by definition more likely to be malignant than benign. Lung cancer masses: squamous cell carcinoma tends to be central (hilar mass ± obstructive collapse/consolidation), while adenocarcinoma tends to be peripheral. Small cell lung cancer (SCLC) appears as a central bulky hilar/mediastinal mass. A peripheral mass with cavitation (irregular thick-walled cavity) represents either squamous cell carcinoma (most common cavitating lung malignancy), or infection (TB, lung abscess — typically smooth-walled cavity with air-fluid level).
Hilar enlargement: bilateral symmetrical hilar adenopathy — the classic 'bat's wing' or 'potato node' pattern — is characteristic of sarcoidosis. Unilateral hilar enlargement, or bilateral asymmetrical enlargement, in a smoker raises strong concern for lung cancer with mediastinal nodal involvement. Bilateral hilar enlargement with mediastinal widening in a young patient suggests lymphoma.
Pleural effusion: a unilateral pleural effusion (especially right-sided) that is large, bloodstained (haemothorax), or associated with an ipsilateral mass should be considered malignant until proven otherwise. Malignant pleural effusions are exudates by Light's criteria (pleural fluid protein/serum protein >0.5; pleural fluid LDH/serum LDH >0.6; pleural fluid LDH >2/3 upper limit of serum LDH). Cytology of pleural aspirate: if positive for malignant cells, staging implications (M1a in NSCLC — unresectable). If cytology negative but effusion is clinically suspected malignant, pleural biopsy (Abrams' needle or thoracoscopic) is required.
Mediastinal widening: superior mediastinal widening in a young patient with anterior mass — consider lymphoma (Hodgkin, commonest cause of anterior mediastinal mass in young adults) vs. thymoma, teratoma, thyroid mass (the 4Ts of anterior mediastinum). Posterior mediastinal mass: neurogenic tumour (schwannoma, neurofibroma). Middle mediastinum: bronchogenic cyst, oesophageal cancer.
Bone lesions on CXR: rib destruction from lung cancer, breast metastasis, or multiple myeloma (multiple 'punched-out' lytic lesions in ribs and vertebrae on CXR — raindrop skull pattern on skull X-ray in myeloma). Sclerotic rib lesions suggest metastatic prostate cancer.
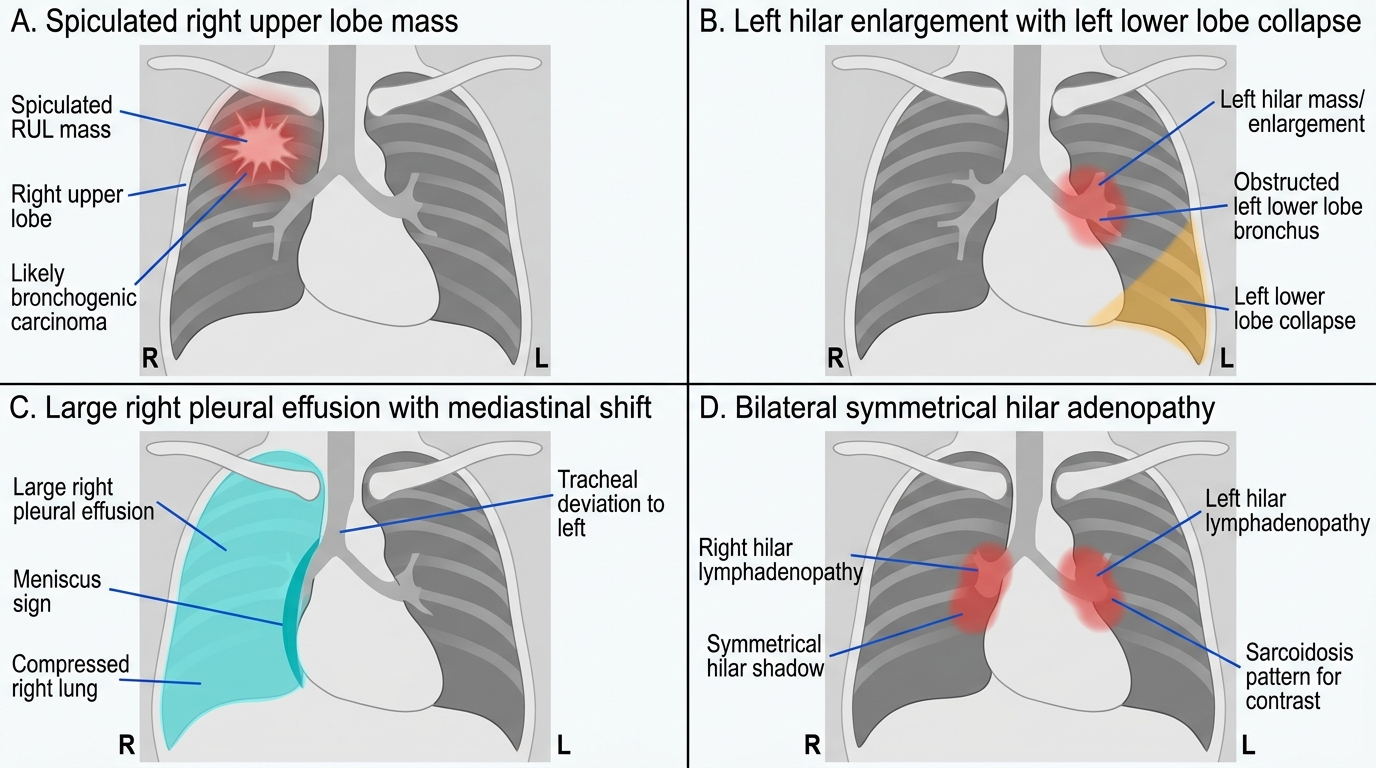
Annotated CXR Patterns in Thoracic Malignancy and Mimics
Mammography, Tissue Biopsy, and Tumour Markers
Mammography is the gold-standard screening and diagnostic imaging modality for breast cancer. It uses low-dose X-rays to image the breast tissue at very low radiation doses — typically 0.1–0.2 mSv per two-view study — and is capable of detecting tumours as small as 2–3 mm, well before they become palpable clinically. In the diagnostic context, mammography is used to characterise a symptomatic breast lump (alongside breast ultrasound in women under 35 years, where the high fibroglandular density of the breast reduces mammographic sensitivity), to assess the contralateral breast in a known cancer patient, and to guide stereotactic biopsy of non-palpable lesions. Mammographic findings are standardised and communicated using the ACR BIRADS (Breast Imaging Reporting and Data System) classification, which assigns a category 0–6 to each finding, with explicit action recommendations that ensure the radiologist and the clinical team are using a shared decision framework. Understanding BIRADS is essential because the treating clinician must be able to interpret the radiologist's report and decide whether biopsy, follow-up, or reassurance is appropriate — a BIRADS 3 'probably benign' lesion does not require immediate biopsy but does require structured 6-month follow-up, while a BIRADS 5 finding requires biopsy before any surgical planning. Mammographic screening every 1–2 years in women aged 40–74 (or 45–74 in some guidelines) reduces breast cancer mortality by approximately 20% in randomised controlled trials; in India, ICMR guidelines recommend clinical breast examination as the primary tool and mammography where radiological infrastructure permits. Mammography has limitations: it has a false-negative rate of approximately 10–20%, rising to 30–40% in dense (ACR Type C or D) breasts, where supplemental ultrasound significantly increases cancer detection rates. It is reported using the ACR BIRADS (Breast Imaging Reporting and Data System) classification (0–6):
| BIRADS Category | Finding | Recommended Action |
|---|---|---|
| 0 | Incomplete — needs additional imaging | Recall for further imaging (USG, additional views) |
| 1 | Negative — no abnormality | Routine screening interval |
| 2 | Benign finding (cyst, calcified fibroadenoma, etc.) | Routine screening interval |
| 3 | Probably benign (<2% malignancy risk) | Short interval follow-up at 6 months |
| 4 | Suspicious (2–95% malignancy) | Tissue sampling (biopsy) recommended |
| 5 | Highly suggestive of malignancy (>95%) | Biopsy required |
| 6 | Known biopsy-proven malignancy | Staging/treatment planning |
Key mammographic features of malignancy: (1) spiculated mass (irregular margin with radiating spicules — highest positive predictive value for cancer); (2) microcalcifications — particularly linear/branching (casting) or clustered pleomorphic calcifications, which represent calcified debris in necrotic ductal carcinoma in situ (DCIS); (3) asymmetric density (new or changing compared to prior study); (4) architectural distortion (normal breast architecture disrupted without a visible mass — may represent sclerosing adenosis, radial scar, or infiltrating cancer). Dense breast parenchyma (ACR Type C or D) limits mammographic sensitivity — supplemental ultrasound is recommended for dense breasts.
Skin biopsy is the definitive diagnostic procedure for suspicious skin lesions. Types of skin biopsy:
- Punch biopsy: a cylindrical core (3–6 mm diameter) removed with a punch instrument under local anaesthetic — suitable for most pigmented lesions, lichenoid lesions, suspected melanoma (avoid if complete excision preferred), and inflammatory dermatoses; provides full-thickness dermis for depth measurement
- Shave biopsy: superficial tangential shave — avoids full depth assessment, inadequate for melanoma staging (Breslow thickness cannot be measured accurately); suitable for exophytic benign lesions
- Excisional biopsy: complete elliptical excision with a 2–5 mm clinical margin — preferred for suspected melanoma (allows accurate Breslow depth measurement across the entire lesion), small suspicious lesions, and lesions where margin assessment is critical
- Incisional biopsy: partial excision — used for large lesions where complete excision is not feasible upfront
Breslow thickness is the single most important prognostic factor for cutaneous melanoma: measured in millimetres from the granular cell layer to the deepest invasive tumour cell. Breslow <0.8 mm = low risk; 0.8–4.0 mm = intermediate; >4.0 mm = high risk. Clark's level (I–V, depth of invasion through skin layers) is an older system now superseded by Breslow thickness but still encountered in practice.
Tissue biopsy for solid tumours — selecting the right technique:
- Fine needle aspiration cytology (FNAC): a 22–25G needle aspirates cells; provides cytological diagnosis (cannot assess tissue architecture or grade); useful for palpable lymph nodes, thyroid, salivary gland, breast; rapid, cheap, minimal trauma; limited when a tissue microenvironment assessment is needed (e.g., lymphoma subtyping)
- Core needle biopsy (CNB): a cutting needle (14–18G, spring-loaded or vacuum-assisted) extracts a 1–2 cm core of tissue; provides histological diagnosis with tissue architecture, grade, and immunohistochemistry (ER, PR, HER2 in breast cancer; CD markers in lymphoma); preferred for solid tumours requiring receptor testing
- Image-guided biopsy: CT-guided or ultrasound-guided core biopsy for deep lesions (lung, liver, retroperitoneum, bone); increases accuracy for small or inaccessible lesions
- Incisional or excisional surgical biopsy: reserved for lesions inaccessible to percutaneous biopsy or when prior percutaneous biopsies are non-diagnostic
- Endoscopic biopsy: bronchoscopic biopsy (endobronchial or transbronchial) for central airway lesions; colonoscopic biopsy for colorectal lesions; gastroscopic biopsy for gastric or oesophageal lesions; ERCP-guided or EUS-guided biopsy for biliary and pancreatic lesions
Tumour markers — clinical indications and interpretation: Tumour markers are serum or tissue-based proteins that indicate the presence, severity, or treatment response of a malignancy. No marker is perfectly sensitive or specific; they are used primarily for monitoring, not for diagnosis or screening (with a few exceptions).
| Marker | Primary Cancers | Notes |
|---|---|---|
| AFP | HCC (diagnostic in cirrhosis + US), testicular NSGCT | >400 ng/mL + cirrhosis + arterialised nodule = HCC (no biopsy needed per guidelines) |
| β-hCG | Gestational trophoblastic neoplasia (GTN), testicular NSGCT | Sole marker that is curative-level sensitive; monitored weekly in GTN |
| PSA | Prostate cancer | Not cancer-specific; PSA density, velocity, free:total ratio refine interpretation |
| CA 125 | Epithelial ovarian cancer | Elevated in >80% advanced ovarian cancer; false positives: endometriosis, PID, cirrhosis, pregnancy |
| CA 19-9 | Pancreatic cancer, cholangiocarcinoma | Monitoring only; cannot screen (low specificity); cannot be produced if patient is Lewis antigen negative (15% of population) |
| CEA | Colorectal cancer | Pre-operative level predicts prognosis; post-operative surveillance for recurrence; NOT for screening |
| CA 15-3 | Breast cancer monitoring | No role in diagnosis; used to monitor metastatic breast cancer treatment response |
| LDH | Lymphoma, testicular cancer, SCLC | Non-specific but elevated LDH correlates with tumour bulk and prognosis in lymphoma; International Prognostic Index includes LDH |
| Thyroglobulin | Post-thyroidectomy differentiated thyroid cancer | Detectable thyroglobulin after total thyroidectomy = recurrent or metastatic disease |
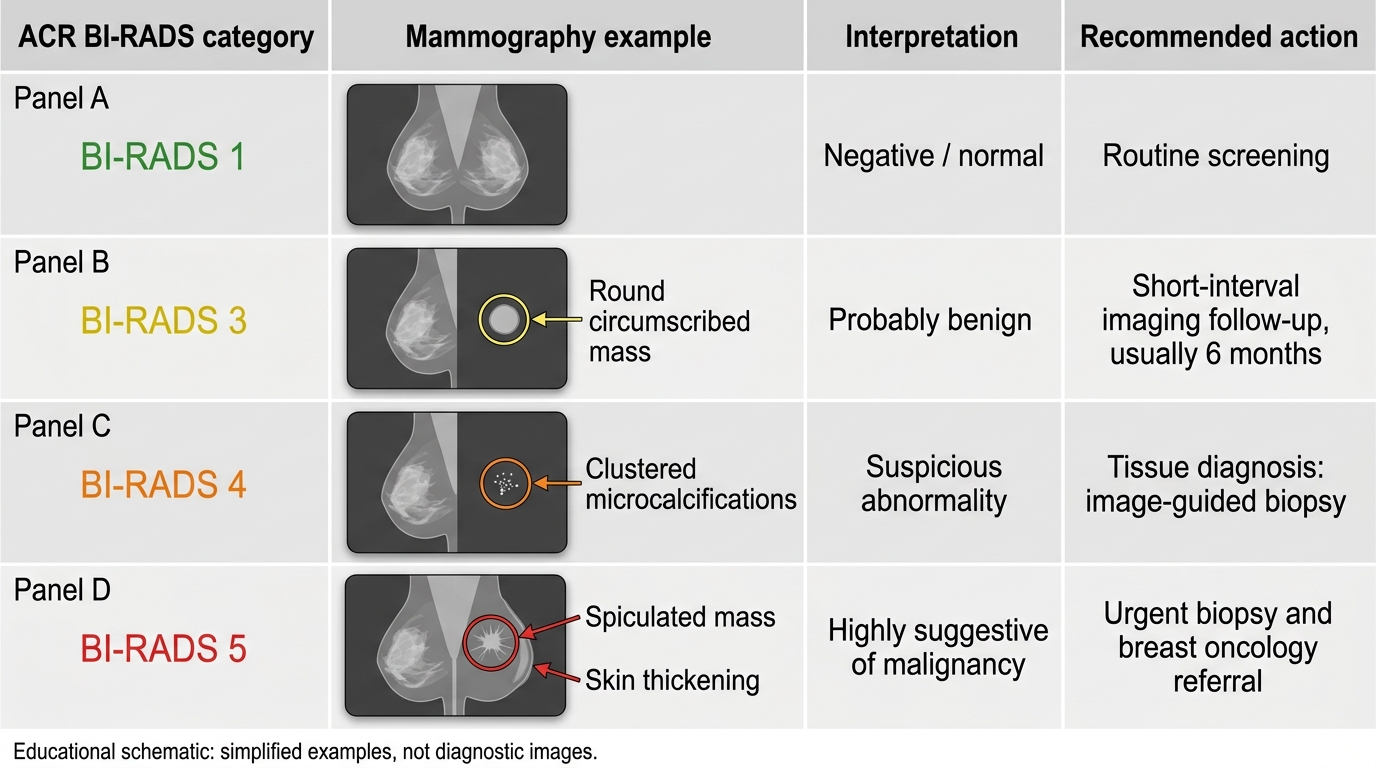
ACR BI-RADS Categories: Mammography Examples and Actions
SELF-CHECK
A 55-year-old woman with cirrhosis from chronic hepatitis B undergoes 6-monthly surveillance with AFP and liver ultrasound. Her AFP rises from 32 ng/mL to 420 ng/mL over 3 months. Ultrasound shows a new 2 cm hepatic nodule with arterial enhancement and portal venous washout on contrast-enhanced CT. What is the most appropriate next step in management?
A. Repeat AFP in 3 months before acting
B. Percutaneous liver biopsy to confirm the diagnosis histologically
C. Diagnose HCC without biopsy and refer for hepatology/surgical assessment for treatment
D. Start empirical antiviral therapy and reassess in 6 months
Reveal Answer
Answer: C. Diagnose HCC without biopsy and refer for hepatology/surgical assessment for treatment
According to AASLD and EASL guidelines, hepatocellular carcinoma (HCC) can be diagnosed without histological confirmation in cirrhotic patients when a hepatic nodule ≥1 cm demonstrates the hallmark vascular pattern on contrast CT or MRI: arterial phase enhancement (HCC is hypervascular, deriving from the hepatic artery) followed by portal venous washout. This radiological diagnosis is accepted because the combination of cirrhosis + typical vascular pattern has a specificity >90% for HCC, and biopsy in this setting carries risks of tumour seeding and sampling error. The AFP >400 ng/mL further strengthens the diagnosis. Biopsy is reserved for atypical radiological presentations. Antiviral therapy does not treat established HCC.