Page 9 of 21
IM13.11-12 | Cancer Diagnostic Testing — SDL Guide (Part 2)
Interpretation of Results — Applied Integration
The skill of diagnostic testing in oncology is not just knowing which tests to order but integrating multiple investigation results into a coherent diagnostic and staging assessment. This section works through the three cases from the module hook to model this integrative process.
Patient A (iron-deficiency anaemia with positive FOBT):
CBC: Hb 8.2 g/dL, MCV 72 fL, MCH 24 pg — hypochromic, microcytic anaemia consistent with iron deficiency from chronic blood loss. Stool occult blood: strongly positive. This combination in a 65-year-old man is a red-flag presentation for colorectal cancer until proven otherwise. The correct sequence: (1) confirm iron deficiency with serum ferritin (low), serum iron (low), TIBC (elevated); (2) baseline CEA (for prognosis and monitoring, NOT for diagnosis); (3) CT colonography or directly colonoscopy as the definitive investigation — the positive FOBT and iron-deficiency anaemia together make colonoscopy mandatory, not optional; (4) if colonoscopy reveals a colorectal cancer, staging with CT chest/abdomen/pelvis. Do not attribute iron-deficiency anaemia in a man over 40 to dietary deficiency without endoscopic investigation.
Patient B (elevated PSA, abnormal DRE):
PSA 18 ng/mL with hard, nodular prostate — PSA >10 ng/mL in combination with abnormal DRE has a >60% positive predictive value for prostate cancer. Correct sequence: (1) repeat PSA if drawn post-DRE; (2) transrectal ultrasound-guided (TRUS) multiparametric MRI prostate (mpMRI) — this is now the preferred pre-biopsy test in many centres because it identifies clinically significant cancer targets and reduces over-detection of low-grade cancers; (3) systematic plus targeted core biopsy (TRUS-guided); (4) if prostate cancer confirmed: Gleason grade and risk stratification (PSA, clinical stage, Gleason sum = International Society of Urological Pathology ISUP grade group 1–5); (5) bone scan (if PSA >20 ng/mL or Gleason score ≥8 or symptomatic bone pain) and CT chest/abdomen/pelvis for staging.
Patient C (persistent lung opacity in a smoker):
CXR: right upper lobe opacity with spiculated margin, 3.5 cm diameter, in a 40 pack-year smoker with haemoptysis. This is a lung mass until proven otherwise. Correct sequence: (1) CT chest with contrast is the mandatory next step after CXR — CT characterises the mass (density, margins, calcification, size), assesses mediastinal and hilar nodes, and detects pleural effusion or other lesions; (2) CT-guided percutaneous core biopsy if peripheral mass (>1 cm from pleura); bronchoscopy with bronchoalveolar lavage and transbronchial biopsy if central/endobronchial; endobronchial ultrasound (EBUS)-guided transbronchial needle aspiration (TBNA) for mediastinal/hilar nodes; (3) PET-CT for staging once histological diagnosis obtained — PET-CT is more sensitive than CT alone for mediastinal nodal staging and distant metastasis; (4) if non-small cell lung cancer (NSCLC) confirmed: molecular profiling — test for EGFR mutation, ALK translocation, ROS1 rearrangement, KRAS G12C mutation, PD-L1 expression (all have approved targeted therapies or immunotherapy implications).
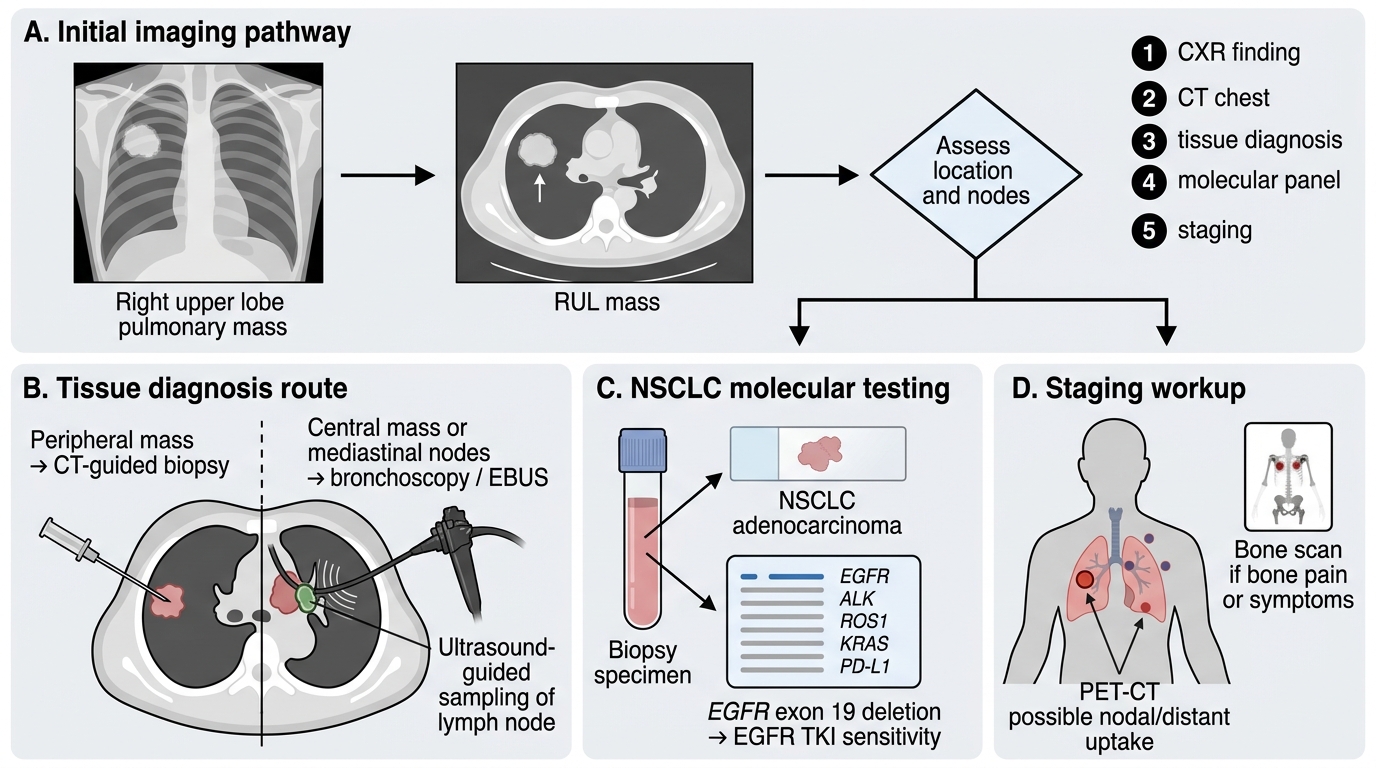
Diagnostic Workup of a Right Upper Lobe Pulmonary Mass
SELF-CHECK
A 45-year-old non-smoker woman is found on CT chest to have a 1.8 cm right lower lobe ground-glass opacity (GGO) with a solid component on a CT done for an unrelated indication. Bronchoscopy biopsy confirms lung adenocarcinoma. Molecular testing shows EGFR exon 19 deletion (a sensitising mutation). What treatment implication does this molecular finding have?
A. The patient should proceed directly to surgical resection without further molecular workup
B. The EGFR mutation makes the tumour resistant to all systemic therapies
C. The patient is likely to respond to EGFR tyrosine kinase inhibitors (e.g., osimertinib) as first-line therapy
D. This mutation indicates the patient should receive bevacizumab (anti-VEGF) targeted therapy
Reveal Answer
Answer: C. The patient is likely to respond to EGFR tyrosine kinase inhibitors (e.g., osimertinib) as first-line therapy
EGFR exon 19 deletions (and exon 21 L858R point mutations) are sensitising mutations that make lung adenocarcinoma cells highly dependent on EGFR signalling. EGFR tyrosine kinase inhibitors (TKIs) — particularly the third-generation osimertinib (preferred first-line) or erlotinib/gefitinib (first-generation) — produce objective response rates of 60–75% in EGFR-mutated NSCLC compared to <10% response rates to first-generation TKIs in EGFR wild-type tumours. Osimertinib is now the preferred first-line agent as it also covers T790M resistance mutations and has CNS penetration. Bevacizumab targets VEGF angiogenesis, not EGFR signalling. Surgical resection alone would not address the driver mutation and would not be appropriate for metastatic disease.
Applied Practice: Selecting and Sequencing Investigations
Mastering diagnostic testing in oncology requires not only knowing the individual tests but practising the decision-making process of selecting and sequencing investigations in the real clinical context. This section provides two applied practice scenarios designed to consolidate your ability to choose the right investigations in the right order — the skill that separates a competent clinician from one who orders tests reflexively.
Applied scenario A: A 65-year-old woman with postmenopausal vaginal bleeding
Presentation: 5 months of intermittent light vaginal bleeding, 13 years after her last period. No abdominal pain. BMI 33. Mild hypertension on amlodipine. No family history of gynaecological cancer. Examination: mildly obese, blood pressure 148/90, no lymphadenopathy. Abdominal examination normal. Pelvic examination: small amount of old blood in the vault; uterus slightly enlarged and firm; no adnexal mass. The clinical suspicion here is endometrial carcinoma — the most common gynaecological malignancy in high-income countries and increasingly prevalent in India as obesity rates rise. Investigation sequence: (1) Transvaginal ultrasound (TVS) — measure endometrial thickness; in a postmenopausal woman, endometrial thickness >4–5 mm is the threshold for further investigation (sensitivity ~96% for endometrial cancer); if thickness ≤4 mm and the patient has low-grade symptoms, endometrial sampling may not be required; (2) Endometrial biopsy — by Pipelle aspirate or hysteroscopy-directed biopsy — if TVS shows thickening or an irregular endometrial stripe; histology is the gold standard and will confirm whether hyperplasia (simple vs. complex, with or without atypia) or carcinoma is present; (3) if carcinoma confirmed on biopsy: MRI pelvis (superior to TVS for myometrial invasion depth and cervical involvement — the two most important staging factors in endometrial cancer), CT chest/abdomen/pelvis for lymph node and distant staging. Note the two-step approach: TVS first, biopsy only if TVS is abnormal — this avoids unnecessary invasive procedures in the majority of women with postmenopausal bleeding who have benign causes (atrophic endometritis, polyps).
Applied scenario B: A 48-year-old man with progressive right upper quadrant pain and a 4 kg weight loss over 3 months
Presentation: background of type 2 diabetes and non-alcoholic fatty liver disease (NAFLD), confirmed on prior ultrasound 2 years ago showing a moderately fatty liver. He now has right upper quadrant dull ache, fatigue, and weight loss. Examination: mild hepatomegaly, liver edge smooth but firm. Mild jaundice. No stigmata of chronic liver disease. AFP: 28 ng/mL (upper limit of normal ~20 ng/mL). Investigation sequence: (1) Abdominal ultrasound — first-line imaging; NAFLD-related cirrhosis or a hepatic mass? A focal lesion should prompt further characterisation; (2) if a focal lesion is found: multiphasic contrast CT or MRI liver — assess for the vascular pattern of HCC (arterial enhancement + venous washout) vs. a metastatic deposit (often peripheral rim enhancement + progressive fill-in for haemangioma; hypo-enhancement throughout for metastatic adenocarcinoma); (3) if vascular pattern consistent with HCC in the context of cirrhosis: apply radiological diagnosis criteria (AASLD/EASL) — biopsy may not be required if lesion ≥1 cm with classic pattern on CT + MRI; (4) if lesion appearance atypical: CT-guided percutaneous core biopsy for histological diagnosis; (5) once HCC confirmed: AFP baseline (for monitoring), liver function tests and Child-Pugh score (determines treatment eligibility — Child-Pugh A/B vs. C affects surgical vs. TACE vs. sorafenib decision), CT chest for lung metastases. The key learning here: AFP is only mildly elevated (28 ng/mL) — normal AFP does not exclude HCC. AFP >20 ng/mL with typical vascular imaging strengthens the clinical diagnosis but the definitive diagnosis in atypical cases requires histology.
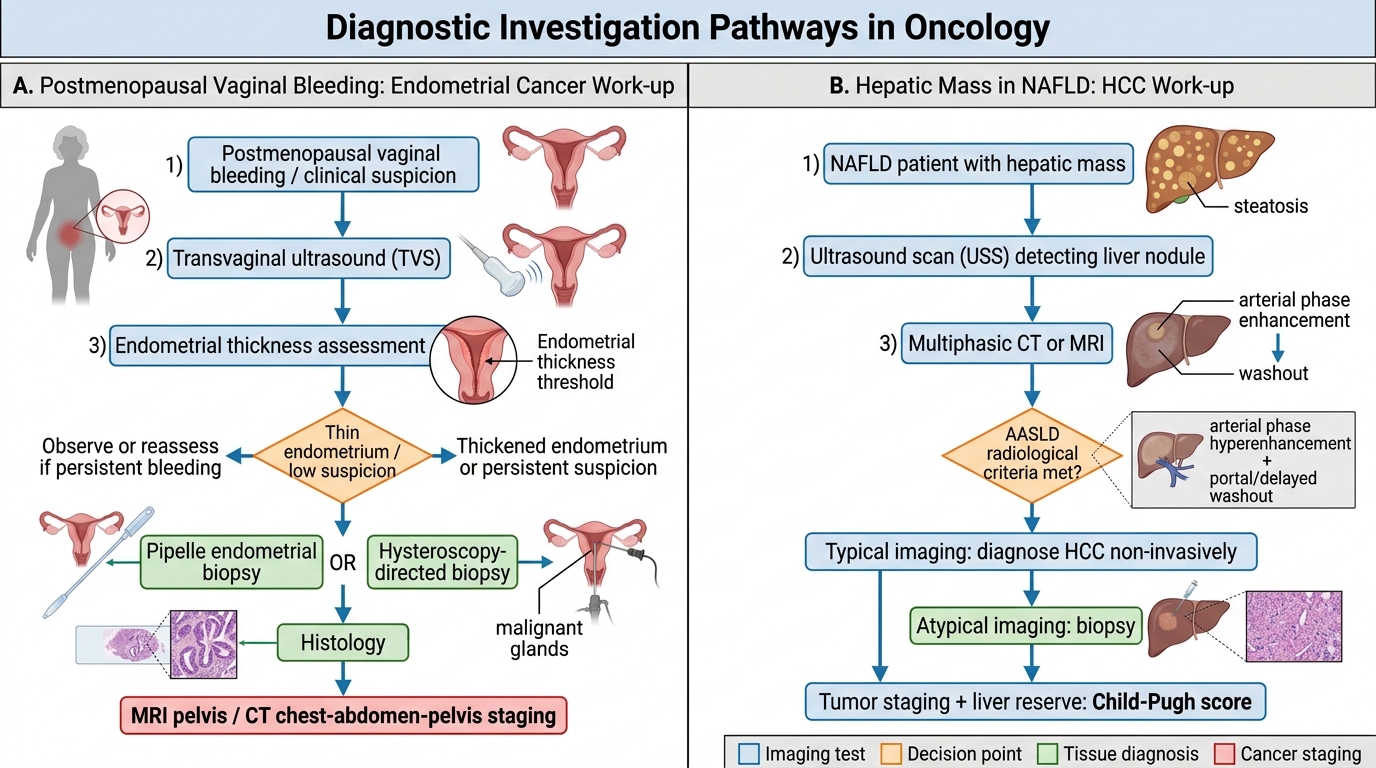
Oncology Diagnostic Investigation Pathways
Self-Assessment: Diagnostic Testing in Oncology
The following self-assessment questions and scenarios test your ability to apply the diagnostic testing principles covered in this module. Work through each before reviewing the answer.
Self-assessment Q1: A peripheral blood film shows numerous small, mature-appearing lymphocytes, many of which are disrupted during smear preparation forming characteristic artefacts. The total WBC is 46 × 10⁹/L. What is the most likely diagnosis and what diagnostic confirmation is needed?
Answer: The smear cells (Gumprecht shadows — disrupted lymphocytes that spill their nuclear material during blood film preparation) combined with mature lymphocytosis are the hallmark of chronic lymphocytic leukaemia (CLL). Confirmation requires flow cytometry of peripheral blood: CLL has a characteristic immunophenotype (B-cell markers CD19, CD20 [dim], CD23 + CD5 co-expression, negative FMC-7 and CD79b [dim] — Matutes score ≥4 = CLL).
Self-assessment Q2: A postmenopausal woman has CA 125 of 340 U/mL. Does this confirm ovarian cancer?
Answer: No. CA 125 is not sufficiently specific for a definitive diagnosis. While elevated CA 125 >35 U/mL in a postmenopausal woman with a pelvic mass carries a high positive predictive value for ovarian cancer, CA 125 can be elevated in endometriosis, uterine fibroids, liver cirrhosis, pleural effusion, and even menstruation (in premenopausal women). The elevated CA 125 must be interpreted alongside pelvic ultrasound (TVS), the Risk of Malignancy Index (RMI = U-score × M-score × CA 125) or ROMA score (includes HE4 + CA 125 + menopausal status), and ultimately surgical specimen histopathology. CA 125 alone should NEVER be used as a screening test or to confirm the diagnosis.
Self-assessment Q3: Why should PSA always be drawn BEFORE digital rectal examination?
Answer: DRE mechanically compresses the prostate, transiently disrupting the basement membrane between the acinar epithelium and the prostatic stroma, allowing PSA to leak into the bloodstream. This can elevate serum PSA by 0.4–2.0 ng/mL for up to 48–72 hours post-DRE. A post-DRE PSA in the grey zone (4–10 ng/mL) may represent a false elevation and should be repeated after 4–6 weeks with PSA drawn before any urological examination.
Self-assessment Q4: A mammogram is reported as BIRADS 3. What does this mean and what is the appropriate action?
Answer: BIRADS 3 = 'probably benign' — the radiologist estimates <2% risk of malignancy. Recommended action: short-interval follow-up mammography at 6 months, then annually for 2 years to document stability. If the lesion increases in size or changes character, upgrade to BIRADS 4 with biopsy. Routine biopsy is NOT recommended for BIRADS 3 (the low malignancy risk does not justify biopsy in most cases; the patient should be counselled about the meaning of this category).
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
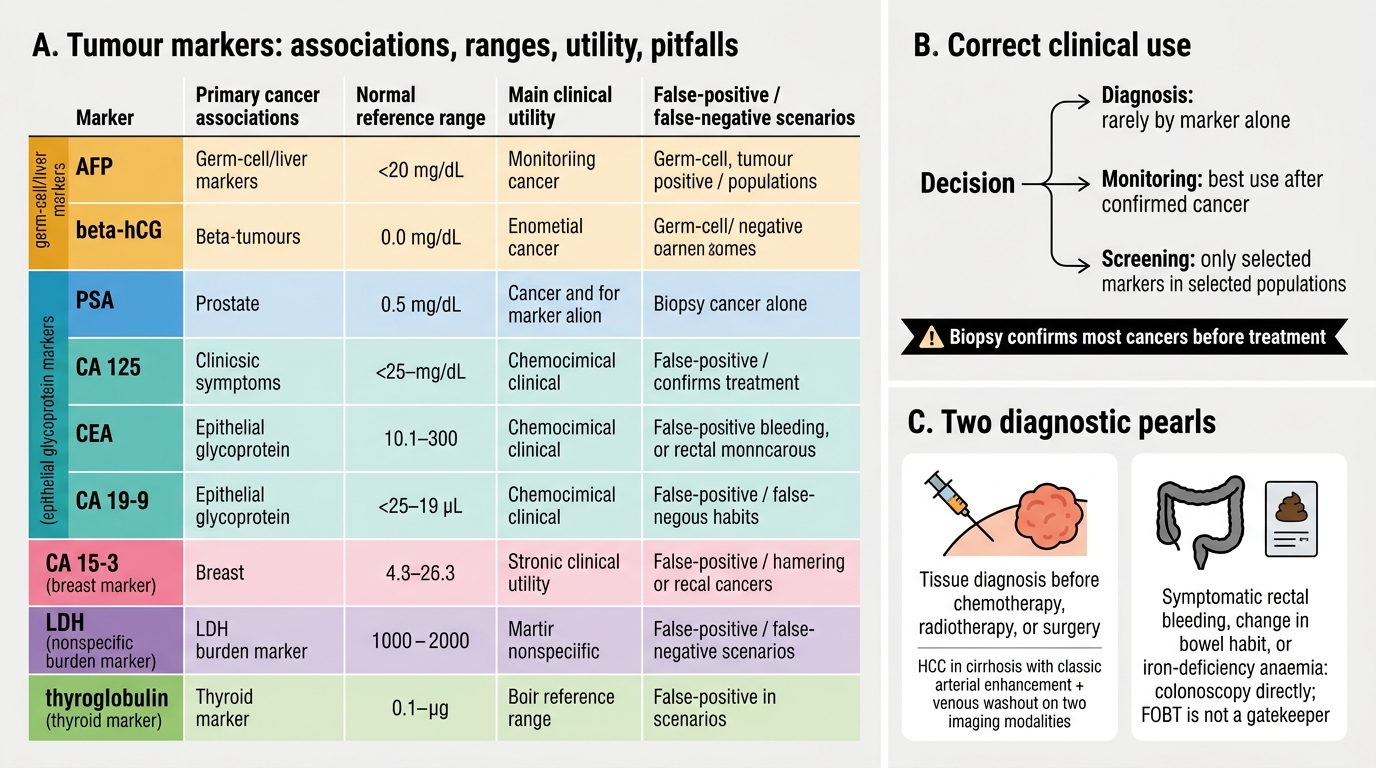
Tumour Markers: Uses, Associations, and Pitfalls
CLINICAL PEARL
Two essential diagnostic pearls:
First, tissue diagnosis is mandatory before treatment in all cancers. No clinical, radiological, or biomarker finding — however convincing — is sufficient to start chemotherapy, radiotherapy, or surgery without histological or cytological confirmation of malignancy. The only exception is HCC in a cirrhotic patient with a classic radiological vascular pattern (arterial enhancement + venous washout) on two imaging modalities. Every other cancer requires biopsy. The reason this matters: biopsy determines histological type (adenocarcinoma vs. squamous vs. small cell), grade, receptor status, and molecular profile — all of which determine treatment choice. Starting empirical chemotherapy without tissue diagnosis is a medical error.
Second, regarding stool occult blood testing: a positive FOBT in a symptomatic patient mandates colonoscopy — it is not a gatekeeper. In a patient with rectal bleeding, change in bowel habit, or iron-deficiency anaemia, proceed directly to colonoscopy without waiting for FOBT. FOBT is a population-level screening tool; in symptomatic patients, its negative predictive value is insufficient to exclude colorectal cancer.