Page 11 of 21
IM13.{6,14,16} | Cancer Treatment Decision Making — SDL Guide
Learning Objectives
- Distinguish between curative and palliative intent in cancer treatment and apply this distinction to clinical scenarios
- Describe the indications for surgery, radiation therapy, and chemotherapy in common malignancies
- Demonstrate an understanding of patients' needs and preferences when choosing between curative and palliative therapy
INSTRUCTIONS
Oncological treatment decision-making integrates tumour biology, patient fitness, available modalities, and most critically — the patient's own values and preferences. This module builds the conceptual framework for how oncologists think about treatment intent, modality selection, and the shared decision-making process that must accompany every treatment plan.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 70 — Cancer Treatment: Surgery, Radiation, and Systemic Therapy (textbook)
- API Textbook of Medicine, 10th ed., Treatment of Malignant Disease (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 11 — Treatment of Cancer (textbook)
- ESMO Clinical Practice Guidelines for Solid Tumours — Key modality sections (2023) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients, same diagnosis — Stage III non-small cell lung cancer. Patient A: a 58-year-old former athlete, ECOG PS 0, no significant comorbidities, good pulmonary function. Patient B: a 72-year-old with COPD, an FEV1 of 42% predicted, mild renal impairment, and an ECOG PS 2. Both have Stage IIIA disease; for Patient A, concurrent chemoradiation with curative intent is the standard of care. For Patient B, the same regimen would carry a high risk of fatal pneumonitis, acute kidney injury from cisplatin, and treatment mortality exceeding any potential survival benefit — so palliative-intent radiotherapy for symptom control plus immunotherapy is planned instead. Same stage, same histology, entirely different treatment intent and strategy. The principle at the heart of this case — that treatment decisions in oncology are never driven by tumour biology alone — is what this module teaches.
WHY THIS MATTERS
NMC competencies IM13.6, IM13.14, and IM13.16 require you to understand and apply the distinction between curative and palliative care, know the indications for each treatment modality, and demonstrate sensitivity to patient preferences and values. These competencies matter because the general physician — not just the oncologist — is frequently the first clinician to counsel a patient after a cancer diagnosis, to explain treatment options, and to help the patient understand what 'cure' means in oncological terms. Getting this conversation right has direct effects on treatment adherence, quality of life, and the patient's trust in the healthcare system.
RECALL
Activate your prior knowledge. Recall the three main cancer treatment modalities: surgery (local-regional), radiation therapy (local-regional), and systemic therapy (chemotherapy, targeted therapy, immunotherapy — systemic). Recall from your pharmacology that alkylating agents, antimetabolites, and topoisomerase inhibitors are classes of cytotoxic chemotherapy agents with different mechanisms of DNA damage. Recall that the ECOG performance status scale (0–4) was covered in the clinical evaluation module — performance status directly determines which treatments a patient can tolerate. From ethics, recall the four principles of Beauchamp and Childress: autonomy, beneficence, non-maleficence, and justice — all four are directly applicable to treatment decision-making in oncology, particularly when weighing aggressive treatment against palliative care.
Curative versus Palliative Intent — the Fundamental Distinction
The most foundational concept in oncological treatment is treatment intent — the explicit answer to the question: 'What are we trying to achieve with this treatment?' In oncology, intent is bifurcated into two categories that determine the entire logic of the treatment plan, the acceptable toxicity burden, the endpoint of therapy, and the nature of the information the patient must receive to give informed consent.
Curative intent means the treatment is designed to eliminate all cancer from the body, with the goal of achieving complete remission and long-term disease-free survival that is functionally equivalent to cure. Curative treatment accepts a higher burden of acute toxicity — including potentially life-threatening complications such as post-operative mortality, radiation pneumonitis, severe myelosuppression, and aplasia — because the long-term benefit of cure justifies these risks. Curative intent is feasible when: (1) the cancer is at a stage where all disease can be encompassed by local therapy (surgery or radiotherapy) or eradicated by systemic therapy; (2) the biology of the tumour is sensitive to available treatments; and (3) the patient has the physiological reserve to survive the treatment and its acute toxicities. Examples of curative-intent treatment: radical nephrectomy for Stage I renal cell carcinoma; chemoradiation for Stage I–III cervical cancer; ABVD chemotherapy (doxorubicin, bleomycin, vinblastine, dacarbazine) for early Hodgkin lymphoma; curative mastectomy or breast-conserving surgery plus adjuvant systemic therapy for Stage I–II breast cancer.
Palliative intent means the treatment is designed to control symptoms, maintain quality of life, and prolong life — but not to cure. Palliative treatment explicitly accepts that the cancer will not be eliminated and that the patient will ultimately die of their disease. This does NOT mean 'no treatment' or 'giving up' — palliative chemotherapy in metastatic colorectal cancer, for example, extends median survival from approximately 5 months (best supportive care alone) to 20–30 months with modern FOLFOX/FOLFIRI ± bevacizumab/cetuximab regimens. The critical distinction is that palliative treatment is constrained by a different toxicity threshold: a treatment that causes 3–4 months of severe nausea, alopecia, and fatigue would be acceptable if it cured the patient, but may not be acceptable if it adds only 3 months of median survival in the palliative context. The therapeutic index calculation — benefit vs. harm vs. patient values — is therefore even more patient-specific in the palliative setting.
Between these two poles lies neoadjuvant and adjuvant therapy: neoadjuvant therapy (given BEFORE the definitive local treatment) aims to shrink the tumour to improve surgical margins, downstage an initially unresectable tumour, or treat micrometastatic disease early; adjuvant therapy (given AFTER the definitive local treatment) aims to eradicate residual microscopic disease and reduce relapse risk. Both are given with curative intent. Classic examples: neoadjuvant FLOT chemotherapy before oesophagogastric cancer surgery; neoadjuvant concurrent chemoradiation before rectal cancer surgery (long-course chemoradiation reduces local recurrence by ~50%); adjuvant paclitaxel + trastuzumab after surgery for HER2-positive breast cancer.
Salvage therapy refers to treatment given after the failure of first-line (or subsequent lines of) therapy — still potentially curative in some haematological malignancies (DHAP or ICE regimens before autologous stem cell transplant in relapsed Hodgkin lymphoma) but more commonly with palliative intent in solid tumours.
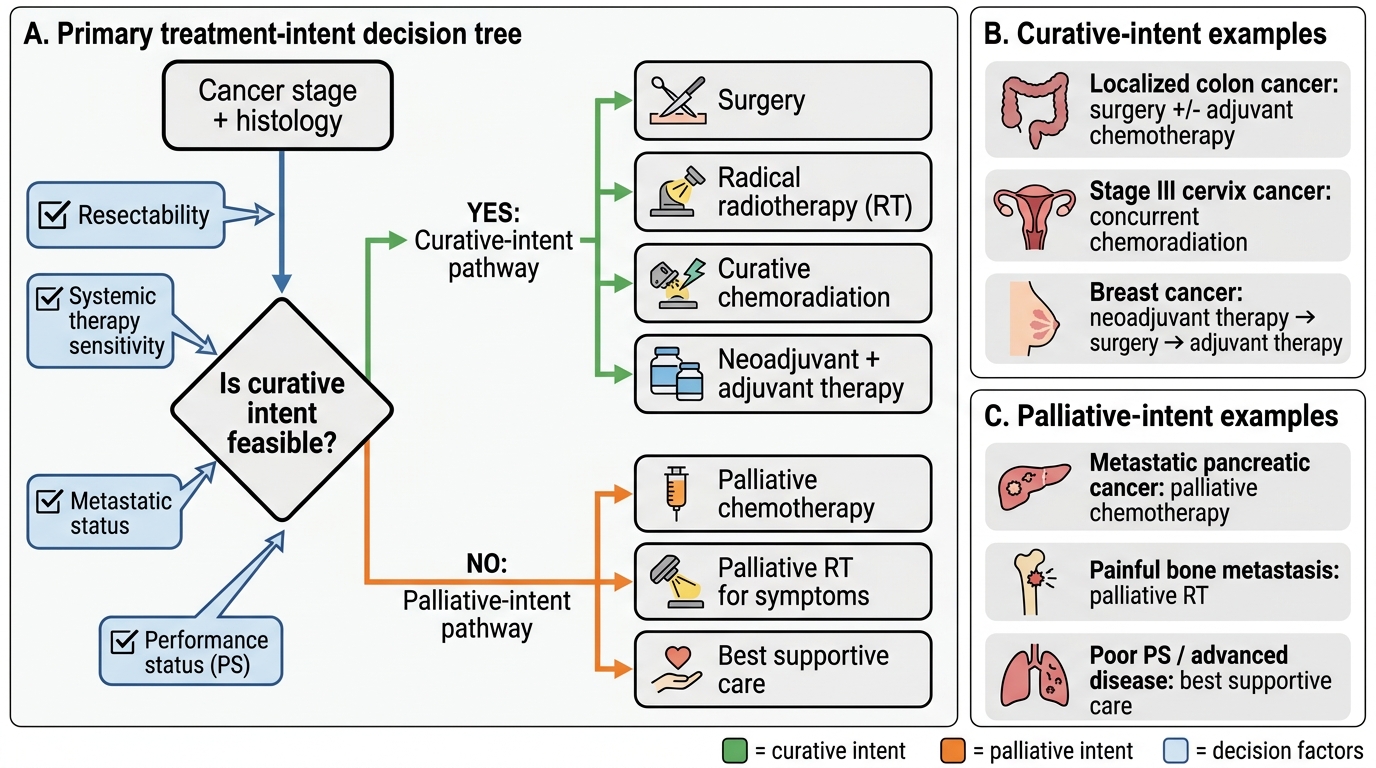
Treatment Intent Decision Tree in Oncology
Pathophysiology of Tumour Growth and Treatment Resistance
Understanding the pathophysiology of tumour growth, spread, and resistance is essential for understanding why specific treatment modalities are chosen for specific tumour types, and why tumours recur. The treatment plan is essentially an attempt to exploit the biological vulnerabilities of the tumour while protecting normal tissue.
Tumour growth kinetics follow a Gompertzian growth model: rapid exponential growth in the early phase (when the tumour is small), followed by deceleration as the tumour enlarges (nutrient/oxygen limitation, necrosis in the core). This is clinically important because small tumours — paradoxically — have the highest proportion of actively dividing cells (the growth fraction), making them most sensitive to cell-cycle-active chemotherapy agents. This is one of the arguments for early systemic treatment and neoadjuvant approaches in large tumours: shrinking the tumour mass may re-enter a larger proportion of cells into the cell cycle, increasing chemosensitivity.
Tumour heterogeneity refers to the existence of genetically distinct clonal populations within a single tumour. This heterogeneity, arising from the high mutation rate of cancer cells, is the primary mechanism of drug resistance: a pre-existing minor clone that carries a resistance mutation (e.g., T790M resistance to first-generation EGFR inhibitors in NSCLC; BCR-ABL T315I mutation conferring resistance to imatinib in CML) may be present before treatment begins. Under selective pressure from the drug, the sensitive clones are killed and the resistant clone expands — driving relapse. This is why combination chemotherapy (multiple agents with different mechanisms) is used for most curative-intent regimens: the probability of a single cell carrying mutations conferring resistance to multiple unrelated agents simultaneously is extremely low.
The log-kill hypothesis: each course of chemotherapy kills a constant fraction of tumour cells (not a constant number). If a regimen kills 99% of cells per cycle and the tumour starts with 10¹⁰ cells, it takes multiple cycles to reduce the burden below 1 cell (log₁₀ = approximately 10 cycles). This explains the empirical observation that most curative chemotherapy regimens require a defined number of cycles (e.g., ABVD × 6 cycles for Hodgkin lymphoma; CHOP × 6 cycles for diffuse large B-cell lymphoma); stopping early 'because the scans look good' carries a high risk of relapse from residual microscopic disease.
The tumour microenvironment (TME): cancer cells exist within a complex ecosystem of cancer-associated fibroblasts, tumour-infiltrating lymphocytes, myeloid-derived suppressor cells (MDSCs), and an aberrant vasculature. Many tumours suppress the immune response through the PD-1/PD-L1 axis — tumour cells express PD-L1, which engages PD-1 on T-cells and suppresses their cytotoxic function. Immune checkpoint inhibitors (pembrolizumab, nivolumab — anti-PD-1; atezolizumab — anti-PD-L1; ipilimumab — anti-CTLA-4) block this suppressive signalling, releasing T-cells to attack the tumour. Their efficacy is highest in tumours with high tumour mutational burden (TMB-H) and MSI-H, where the large neoantigen load provides abundant T-cell targets.
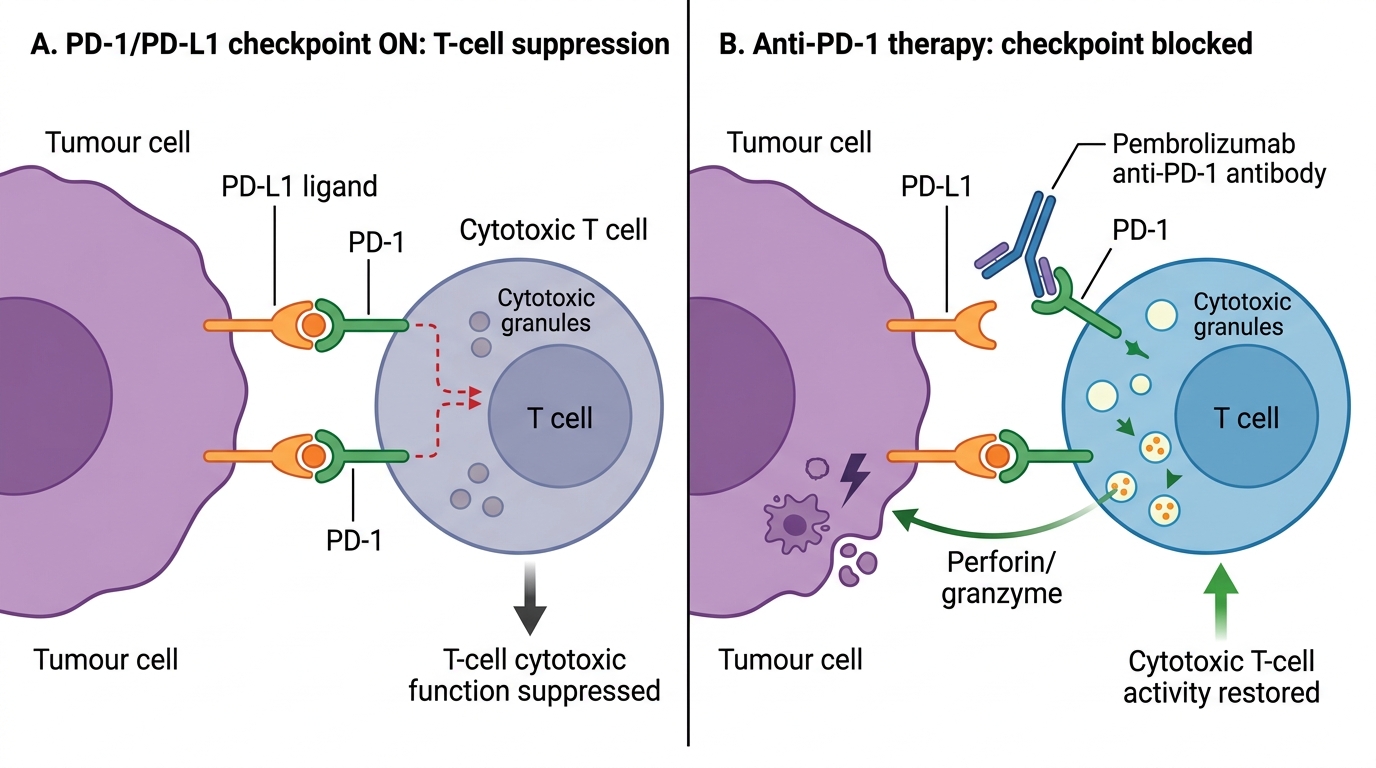
PD-1/PD-L1 Immune Checkpoint Axis and Pembrolizumab Action
SELF-CHECK
A patient with Stage II Hodgkin lymphoma is receiving ABVD chemotherapy with curative intent. After 2 cycles, an interim PET-CT shows a complete metabolic response (Deauville score 1). The patient asks if the remaining 4 cycles can be cancelled since 'the scans show no cancer'. What is the correct explanation?
A. Yes — a complete PET response after 2 cycles means cure; the remaining cycles are unnecessary
B. No — the log-kill model predicts that residual microscopic disease (below PET detection threshold) is likely still present; completing the full course is required for cure
C. No — more cycles are needed only if the interim PET shows residual uptake; a negative scan means all cancer is gone
D. Yes — extending chemotherapy beyond imaging response increases toxicity without additional benefit
Reveal Answer
Answer: B. No — the log-kill model predicts that residual microscopic disease (below PET detection threshold) is likely still present; completing the full course is required for cure
PET-CT cannot detect residual microscopic disease below approximately 10⁶–10⁷ cells — a burden that is clinically and radiologically 'invisible' but capable of regenerating a full relapse. The log-kill model demonstrates that multiple courses of chemotherapy are needed to reduce the tumour burden below a critical threshold. For Stage II favourable Hodgkin lymphoma, interim PET-adapted de-escalation (e.g., reducing ABVD to AVD) is evidence-based, but the total number of cycles should follow the protocol. Stopping treatment at a complete imaging response prematurely would leave residual microscopic disease untreated and risk relapse.
Indications for Surgery, Radiation, and Systemic Therapy
Each of the three primary treatment modalities has distinct biological, anatomical, and physiological prerequisites that determine its indication. In clinical practice, these modalities are almost always used in combination — the art of oncological treatment planning lies in selecting the right combination, in the right sequence, with the right intent.
SURGERY is the definitive curative local treatment for most solid tumours when disease is localised and technically resectable. The goals of surgery vary: (1) curative resection — complete removal of the tumour with negative surgical margins (R0 resection), which is the standard objective for most solid tumours (colorectal cancer, gastric cancer, breast cancer, lung cancer, renal cell carcinoma, soft tissue sarcoma); an R1 resection (microscopic positive margin) carries a high local recurrence risk; R2 (macroscopic residual disease) is not curative; (2) debulking (cytoreductive surgery) — intentional removal of as much tumour as possible even when complete resection is not achievable; the most important example is optimal cytoreduction in ovarian cancer (residual disease <1 cm, ideally no macroscopic residual — associated with significantly improved response to subsequent platinum-taxane chemotherapy); (3) palliative surgery — procedures to relieve symptoms without curative intent: colostomy for obstructing rectal cancer, biliary stenting for pancreatic head cancer obstructing the common bile duct, vertebroplasty for painful bone metastases, TURP for obstructing prostate cancer.
Surgical eligibility depends on: tumour factors (TNM stage, proximity to critical structures, vascular involvement, extent of nodal disease) and patient factors (cardiopulmonary reserve — FEV1 for thoracic surgery, cardiac function for abdominal aortic involvement; nutrition — malnourished patients tolerate surgery poorly; ECOG PS — PS ≥3 contraindicates major surgery in most settings).
RADIATION THERAPY (RT) uses ionising radiation (photons — X-rays or gamma rays; or protons) to damage tumour cell DNA, primarily by creating double-strand breaks. The therapeutic index of radiotherapy is exploited by fractionation — dividing the total dose into multiple smaller fractions (fractions of 1.8–2 Gy daily, Monday to Friday). Fractionation exploits the '4Rs of radiobiology': Repair (normal tissues repair radiation damage between fractions better than tumour cells), Redistribution (cycling cells in sensitive phases move into sensitive phases), Repopulation (repopulation in normal tissues is faster), and Reoxygenation (hypoxic resistant cells become oxygenated between fractions). Indications for RT: radical (curative-intent) RT — for anatomically inoperable tumours or as an alternative to surgery in organ-preserving approaches (e.g., radical chemoradiation in Head and Neck SCC, anal canal cancer, early laryngeal cancer, cervical cancer Stage IB–IVA); adjuvant RT — after surgery to reduce local recurrence (post-mastectomy RT, adjuvant RT after rectal cancer surgery); neoadjuvant RT — to downstage before surgery (long-course chemoRT for rectal cancer, pre-operative RT for extremity sarcoma); palliative RT — for bone metastases (single fraction 8 Gy is as effective as multi-fraction for pain control — SCORAD trial), brain metastases (whole brain RT or stereotactic radiosurgery), SVC obstruction (emergency palliative RT).
SYSTEMIC THERAPY encompasses all treatments delivered through the bloodstream, targeting cancer wherever it may be:
- Conventional cytotoxic chemotherapy: cell-cycle-non-specific agents (alkylating agents: cyclophosphamide, platinum compounds — cisplatin, carboplatin, oxaliplatin; anthracyclines: doxorubicin, epirubicin — intercalate DNA and inhibit topoisomerase II; are cardiotoxic with cumulative dose limit) and cell-cycle-specific agents (antimetabolites: 5-fluorouracil, methotrexate, gemcitabine — inhibit DNA/RNA synthesis; taxanes: paclitaxel, docetaxel — stabilise microtubules; vinca alkaloids: vincristine, vinblastine — inhibit microtubule polymerisation).
- Targeted therapy: agents designed against specific molecular drivers — TKIs (imatinib for BCR-ABL1 CML; erlotinib/osimertinib for EGFR-mutated NSCLC; crizotinib/alectinib for ALK-rearranged NSCLC); monoclonal antibodies against tumour antigens (trastuzumab for HER2-amplified breast and gastric cancer; rituximab for CD20+ B-cell lymphoma; cetuximab for EGFR+ colorectal cancer — only if KRAS wild-type); PARP inhibitors (olaparib for BRCA-mutated breast and ovarian cancer).
- Immunotherapy: immune checkpoint inhibitors (anti-PD-1: pembrolizumab, nivolumab; anti-CTLA-4: ipilimumab); CAR-T cell therapy for haematological malignancies (B-ALL, diffuse large B-cell lymphoma — post-relapse).
- Hormonal therapy: for hormone-receptor-positive cancers — tamoxifen or aromatase inhibitors (anastrozole, letrozole) for ER+ breast cancer; androgen deprivation therapy (GnRH agonists: leuprolide; or GnRH antagonists: degarelix) and androgen receptor pathway inhibitors (enzalutamide, abiraterone) for prostate cancer.
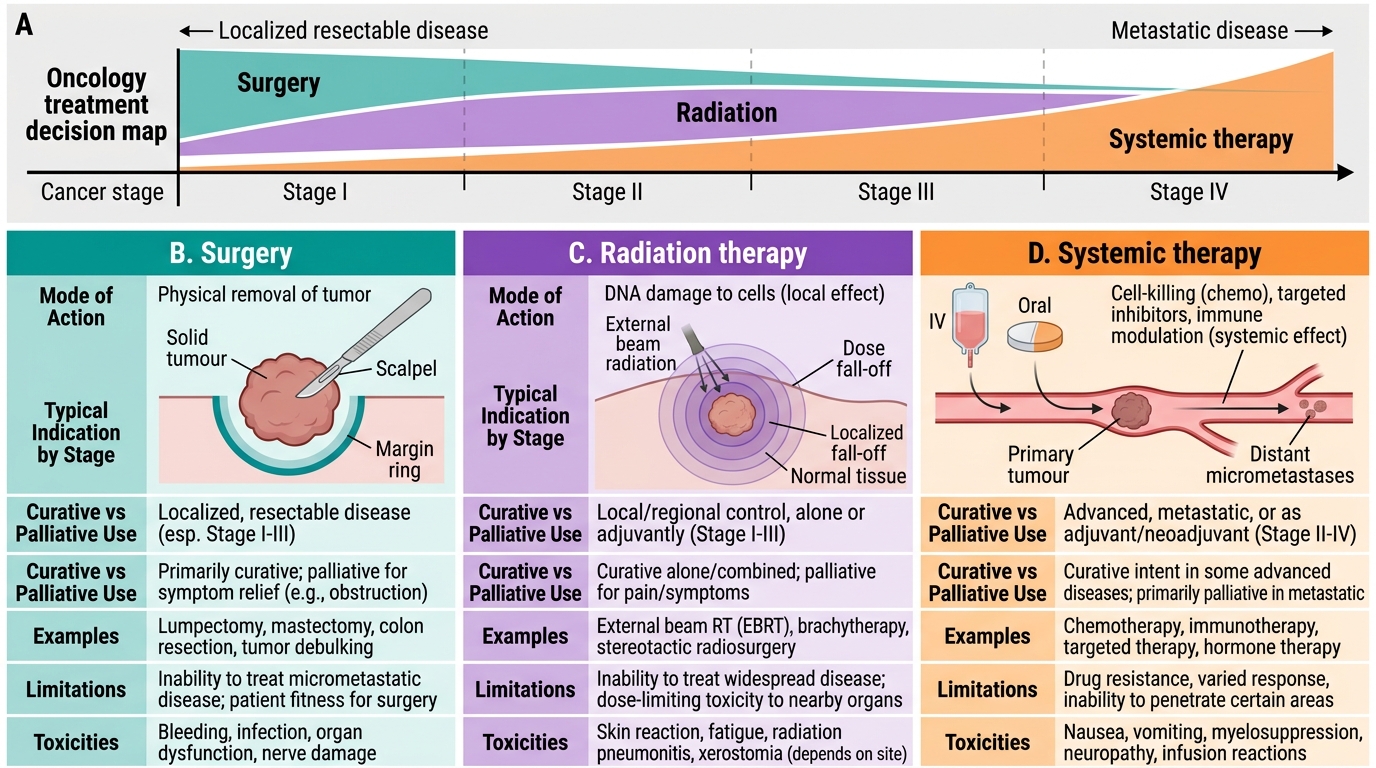
Primary Modalities in Cancer Treatment