Page 12 of 21
IM13.{6,14,16} | Cancer Treatment Decision Making — SDL Guide (Part 2)
Patient-Centred Treatment Decision Making
The oncological treatment decision is not purely a technical exercise — it is fundamentally a shared decision-making process between the clinician, the multidisciplinary team (MDT), and the patient. NMC competency IM13.16 explicitly requires demonstration that the student understands the needs and preferences of patients when choosing between curative and palliative therapy. This section addresses the practical and ethical dimensions of this process.
Shared decision making (SDM) in oncology has three essential components: (1) the clinician provides accurate, comprehensible information about the diagnosis, the available treatment options, the expected outcomes (survival benefit, response rates, quality of life during treatment), the potential toxicities, and the consequences of no treatment; (2) the patient's values, preferences, cultural and religious beliefs, family situation, and personal goals are elicited and given genuine weight; (3) a decision is reached collaboratively that reflects both the clinical evidence and the patient's priorities. This process is meaningfully different from informed consent — SDM does not simply require the patient to agree to the plan the doctor has already decided; it begins before the plan is formed.
In the Indian clinical context, several factors complicate SDM: (1) financial toxicity — the out-of-pocket cost of modern targeted therapies (osimertinib ~₹50,000–₹80,000/month; trastuzumab biosimilars have improved affordability) and the absence of universal health coverage means that the 'best available treatment' for a given tumour may be economically catastrophic; a patient who cannot afford 6 cycles of treatment will not benefit from a protocol designed for 6 cycles; (2) family-centred decision-making — in many Indian families, diagnosis disclosure and treatment decisions are shared with or delegated to the family rather than the patient alone; the physician has an ethical obligation to the patient's autonomy while respecting cultural norms; (3) health literacy — many patients cannot evaluate statistical expressions of benefit (e.g., '5% absolute survival benefit'); using natural language framing ('out of 100 patients like you, 5 more would be alive at 5 years with this treatment') or pictographs improves comprehension; (4) prognostic disclosure — many Indian patients prefer family-filtered prognostic information; the physician must navigate between honesty, sensitivity, and respect for the patient's expressed preferences about disclosure.
Quality of life versus survival trade-off: for many patients with advanced cancer, the question is not 'Do you want to live?' but 'How do you want to live with this illness?' A patient with metastatic pancreatic cancer may have a median overall survival of 11–12 months with FOLFIRINOX (highly toxic combination chemotherapy) versus 8–9 months with gemcitabine monotherapy (better tolerated). The absolute survival difference is 3 months — but the toxicity difference is large. For a patient who prioritises being well enough to attend a daughter's wedding in 4 months or to maintain independence, gemcitabine may be the right choice. For a patient who prioritises maximum survival time and accepts severe toxicity, FOLFIRINOX may be right. Neither is wrong — both are evidence-based. The physician's role is to present both options clearly and help the patient identify which aligns with their values.
The ECOG PS and treatment eligibility: performance status is the single most important patient-specific determinant of treatment eligibility. PS 0–1 patients tolerate full-dose cytotoxic chemotherapy; PS 2 patients require dose modification or single-agent regimens; PS 3–4 patients are generally not candidates for cytotoxic chemotherapy — the risk of treatment mortality outweighs the benefit. These thresholds must be communicated transparently: 'Your overall health means that intensive chemotherapy would be more likely to harm you than help you — here is what we can do to control your symptoms and maintain your quality of life.'
Multidisciplinary team (MDT): in India's tertiary cancer centres (Tata Memorial Hospital, AIIMS Cancer Institute, CMC Vellore, and similar institutions), treatment decisions are made at tumour board meetings attended by surgical oncologists, medical oncologists, radiation oncologists, radiologists, pathologists, and increasingly palliative care specialists. The MDT model reduces unilateral error, ensures that all modalities are considered, and produces a treatment plan that is evidence-based and tailored to the individual patient.
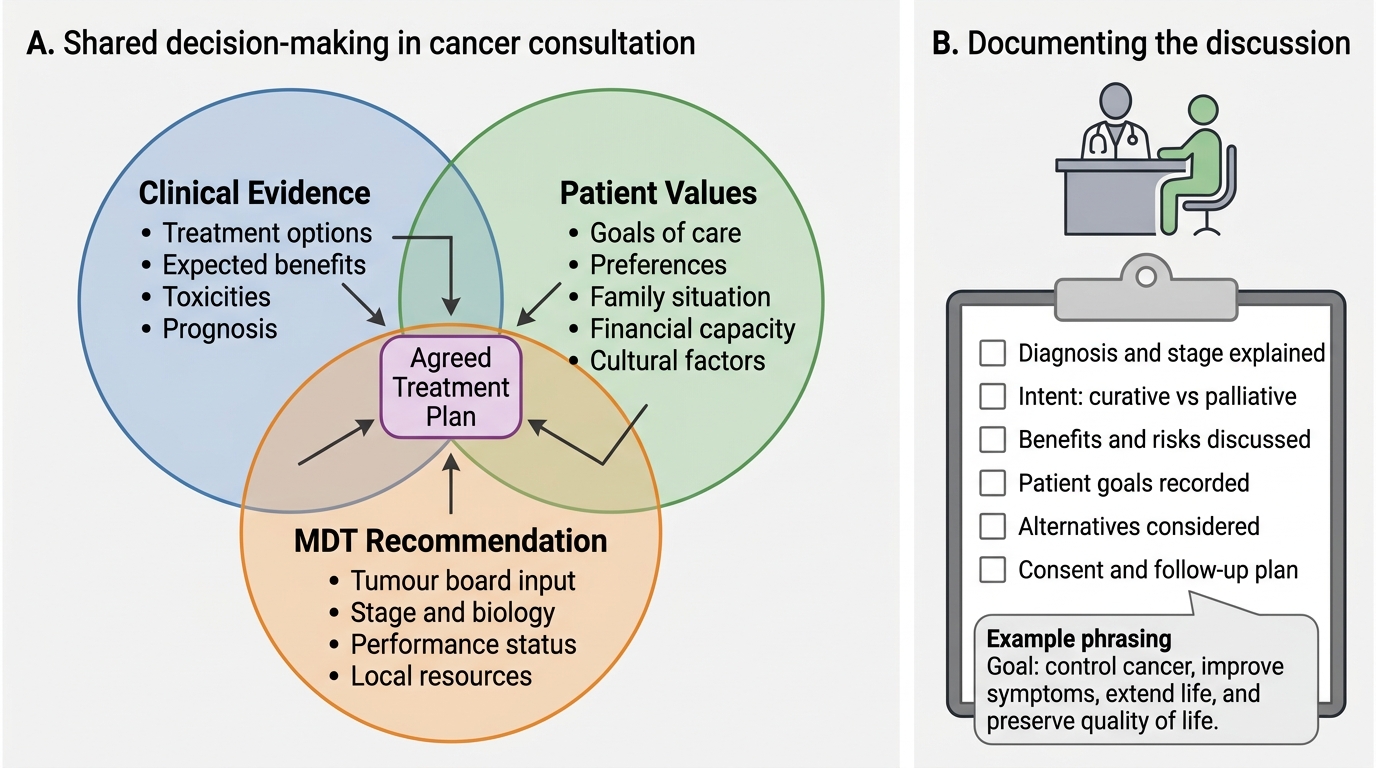
Shared Decision-Making in Cancer Consultation
SELF-CHECK
A 67-year-old woman with metastatic HER2-positive breast cancer is offered first-line trastuzumab plus chemotherapy. She asks whether the treatment is 'to cure her cancer'. Which is the most accurate and appropriate response?
A. Yes — trastuzumab-based therapy cures most HER2-positive metastatic breast cancers within 2 years
B. The treatment is designed to control the cancer for as long as possible, improve your symptoms, and extend your life, but at this stage the goal is not cure — it is to give you the best quality of life for the longest time
C. No treatment can help metastatic breast cancer — we can only provide pain relief
D. Whether it is curative or palliative depends entirely on your response to the first cycle
Reveal Answer
Answer: B. The treatment is designed to control the cancer for as long as possible, improve your symptoms, and extend your life, but at this stage the goal is not cure — it is to give you the best quality of life for the longest time
Metastatic (Stage IV) HER2-positive breast cancer is generally not curable with current systemic therapy, though long-term control (years) is possible in a subset of patients with trastuzumab-based regimens (e.g., pertuzumab + trastuzumab + docetaxel = CLEOPATRA regimen; median overall survival >56 months). The honest and compassionate response acknowledges that the intent is palliative — control, symptom improvement, and life prolongation — without cure. Saying 'Yes, it cures' is factually wrong and sets up a devastating expectation mismatch. Saying 'nothing can help' is also false and denies the patient access to effective treatment. The correct response reflects shared decision-making: honest intent plus realistic optimism about achievable benefit.
Self-Assessment: Treatment Decision Making Scenarios
These integrative scenarios test your ability to apply the curative/palliative distinction, modality indications, and patient-centred principles to realistic clinical situations.
Scenario A: A 45-year-old woman with Stage IB cervical cancer (tumour 4.5 cm, confined to the cervix, no lymph node involvement, no distant metastasis on CT/MRI) is referred to the oncology MDT. She is otherwise well, ECOG PS 0. Which treatment modalities are appropriate with curative intent, and how would you explain the choice to the patient?
Analysis: Stage IB2 cervical cancer is a potentially curable disease. Two curative-intent options exist with equivalent survival outcomes: (1) radical hysterectomy with bilateral pelvic lymph node dissection (Wertheim's procedure) — surgical option; (2) concurrent chemoradiation — external beam pelvic radiotherapy plus cisplatin chemotherapy plus intracavitary brachytherapy. Both achieve 5-year survival rates of approximately 80–85% for Stage IB. The choice between surgery and chemoradiation depends on patient preference (surgical complications including bladder and bowel dysfunction vs. radiation late effects), fertility wishes (radical trachelectomy is an option in selected cases for fertility preservation), and centre expertise. The clinician's role is to explain both options, their benefits and side-effects, and allow the patient to make an informed choice — a textbook SDM scenario. NEVER present only one option without mentioning the equivalent alternative unless there is a clear medical contraindication.
Scenario B: A 70-year-old man with Stage IV NSCLC (adenocarcinoma, EGFR wild-type, PD-L1 TPS 60%, ECOG PS 1) has been told by a relative that 'chemotherapy will definitely kill him before the cancer does'. He is reluctant to start treatment. How do you counsel him?
Analysis: First, acknowledge his fear — it is legitimate. However, his tumour has a PD-L1 expression of 60% (≥50%), qualifying him for pembrolizumab monotherapy as first-line treatment (KEYNOTE-024 trial). Pembrolizumab is immunotherapy — NOT conventional cytotoxic chemotherapy — with a fundamentally different toxicity profile: immune-related adverse events (pneumonitis, colitis, endocrinopathy) rather than the nausea, alopecia, and neutropenia of chemotherapy. Pembrolizumab improves median overall survival to approximately 26 months (vs. 14 months with chemotherapy) with a significantly better quality-of-life profile. The counselling must correct his misconception about 'chemotherapy', explain the mechanism of immunotherapy clearly, and provide realistic information about the magnitude of benefit. Treatment choice should still be collaborative — he has the right to decline — but the decision must be based on accurate information.
Scenario C: A 78-year-old woman with newly diagnosed Stage IIIC ovarian cancer, ECOG PS 3 (confined to bed more than 50% of waking hours due to significant ascites, abdominal pain, and malnutrition), presents with her daughter who insists 'we must do everything possible.' How do you approach the treatment discussion?
Analysis: ECOG PS 3 patients have very limited reserve for cytotoxic chemotherapy; standard first-line platinum-based chemotherapy (carboplatin plus paclitaxel) carries a risk of severe myelosuppression, renal impairment, and treatment-related death in this patient that likely exceeds any survival benefit. The priority is: (1) paracentesis for symptom relief — draining the ascites may improve PS enough to reassess treatment eligibility; (2) nutritional support and symptom management; (3) honest conversation with the patient AND family — the daughter's 'do everything' request must be balanced against the patient's own wishes and the real likelihood of harm from aggressive treatment. The PATIENT — not the family — is the primary decision-maker. In the Indian context, this is often the most sensitive conversation in clinical oncology. Gentle but honest prognostic disclosure, referral to palliative care, and a clearly documented advance care plan are the appropriate responses. This does NOT mean abandoning the patient — it means redirecting care toward what will genuinely help her.
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
Curative vs Palliative Intent in Oncology
CLINICAL PEARL
Two critical clinical pearls for treatment decision-making:
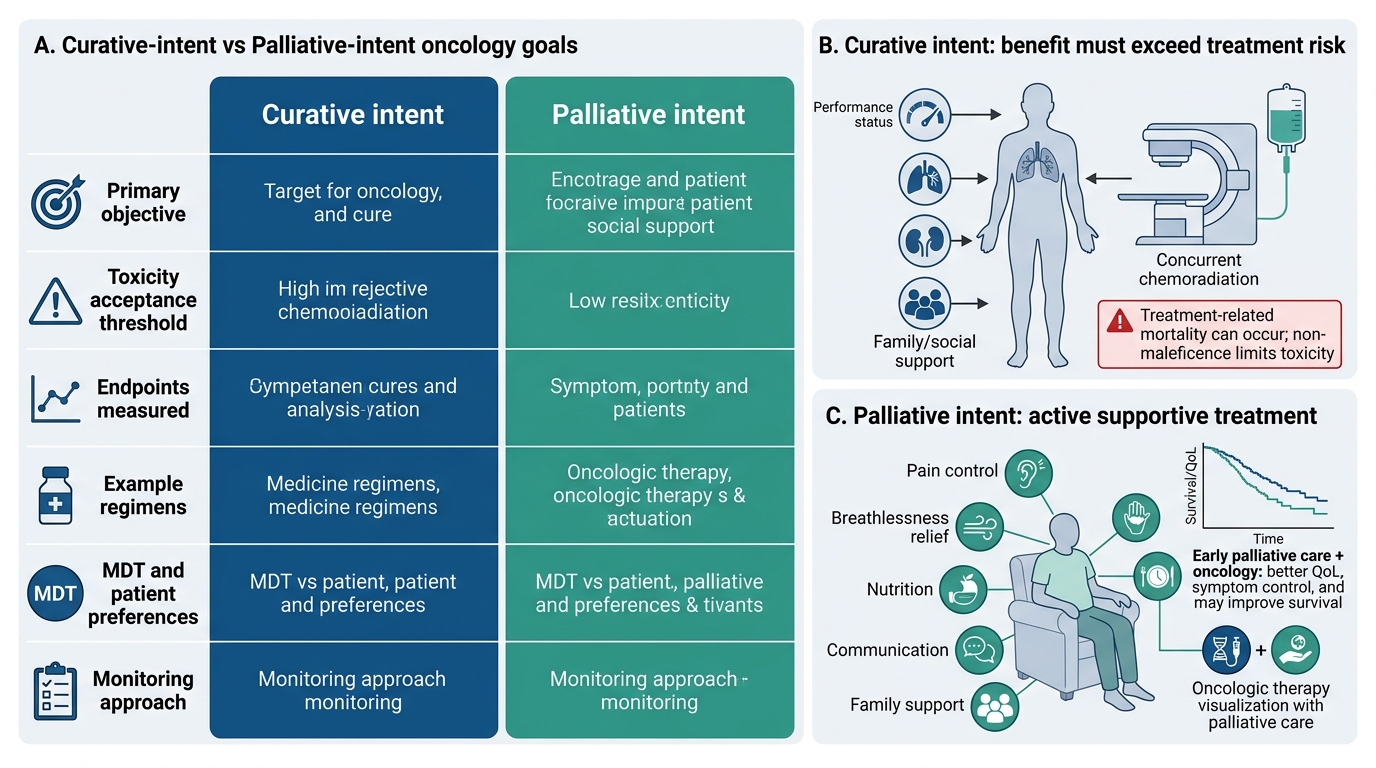
First, curative intent does not mean all adverse events are justified. Treatment mortality is a real outcome — cisplatin-based concurrent chemoradiation for Stage III NSCLC has a 2–5% treatment-related mortality rate in fit patients and significantly higher in those with poor lung function or renal impairment. When recommending curative-intent treatment, the clinician must be confident that the patient's PS, organ function, and social support are sufficient to survive the treatment itself. The principle of non-maleficence limits acceptable toxicity even in curative intent.
Second, palliative care is not the absence of treatment — it is a positive intervention. The Temel et al. (2010) landmark trial in the New England Journal of Medicine demonstrated that early integration of specialist palliative care alongside oncological treatment in Stage IV NSCLC patients improved median survival by approximately 2.7 months more than standard oncological care alone — despite the palliative care group receiving less aggressive end-of-life chemotherapy. The mechanism: better symptom management, earlier discontinuation of futile therapy, reduced depression, and improved nutrition. Palliative care from diagnosis — not just at the end of life — is now endorsed by ASCO, ESMO, and IAPC as a quality standard in oncology.