Page 5 of 15
IM14.6-10 | Obesity Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit and document a structured obesity history covering weight trajectory, dietary habits, physical activity, medications, family history, secondary cause symptoms, and motivational readiness
- Perform a systematic obesity-focused physical examination including correct anthropometric measurement technique (BMI, waist circumference, hip circumference, neck circumference) and targeted signs of secondary causes
- Generate a prioritised differential diagnosis for obesity, distinguishing primary multifactorial from secondary causes, and identify red-flag features requiring urgent investigation
- Select and interpret appropriate investigations for obesity including mandatory baseline tests and targeted secondary cause screening
- Apply the diagnostic criteria and investigation strategy for hypothyroidism, Cushing syndrome, and PCOS as secondary causes of obesity
INSTRUCTIONS
This module develops the clinical skills for structured evaluation of obesity in Indian patients. The competencies addressed (IM14.6–14.10) require applied skills at the SH level — meaning you must be able to perform and document the history, examination, and investigations on a real patient encounter. Focus on the technique of anthropometric measurement, the 7-domain history structure, the red-flag secondary cause features, and the interpretation of investigation results in clinical context.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 415 — Evaluation and Management of Obesity (textbook)
- API Textbook of Medicine, 10th ed. — Clinical Approach to Obesity (textbook)
- Obesity Management Association of India (OMAI): Clinical Practice Guidelines for Management of Obesity in Indians, 2016 (guideline)
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group: Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are seeing a 42-year-old woman referred by her gynaecologist for 'obesity and irregular periods.' She weighs 88 kg and is 158 cm tall. Before you even open the consultation, consider what you already know: her BMI is approximately 35.3 kg/m² — well into the obese category by Asian-Indian standards. But the art of the obesity consultation lies not in the number on the weighing scale. It lies in the history you take in the next 20 minutes — how she gained the weight, what she eats, how she moves, why she is here now, and crucially, whether she has the motivation and self-efficacy to change. The physical examination that follows must be purposeful: not merely confirming that she is heavy, but actively searching for signs of secondary causes (hypothyroidism? Cushing syndrome?) and the complications already in motion (hypertension? acanthosis? sleep apnoea?). The clinical evaluation of obesity is a skill — and like all clinical skills, it rewards structure and deliberate practice.
WHY THIS MATTERS
The clinical evaluation of obesity is a skill that will be exercised in every medical specialty. The NMC competencies IM14.6–14.10 require you to elicit and document a structured obesity history (including dietary habits, physical activity, medications, family history, and motivational readiness), perform a targeted physical examination, generate and prioritise a differential diagnosis including secondary causes, and select and interpret investigations. These skills apply whether you are seeing the patient in general medicine, endocrinology, cardiology, gynaecology, or a family practice setting. They underpin not only the diagnostic encounter but the therapeutic relationship — how you take this history shapes whether the patient returns for follow-up.
RECALL
Before the clinical assessment module, activate your knowledge from the Obesity Foundations module. Recall that Asian-Indian BMI cut-offs define overweight as ≥23 kg/m² and obesity as ≥25 kg/m², substantially lower than Western thresholds. Recall that waist circumference cut-offs for central obesity are ≥90 cm in men and ≥80 cm in women. Recall the secondary causes of obesity — hypothyroidism, Cushing syndrome, PCOS, hypothalamic injury, growth hormone deficiency, insulinoma — each with characteristic clinical features that the history and examination must actively seek. Recall that metabolic syndrome by IDF 2005 requires central obesity (mandatory) plus any 2 of TG ≥150, HDL <40/50, BP ≥130/85, FBG ≥100. These form the clinical backbone of the evaluation you are about to perform.
Clinical Indication: When and Why to Evaluate for Obesity
The clinical evaluation of obesity is triggered by a range of clinical presentations, and recognising when to initiate a structured obesity workup is the first competency in this skills module. Unlike many clinical problems that present with a chief complaint, obesity often enters the consultation as a finding rather than a primary concern — yet it may be the most important modifiable determinant of the patient's current and future health. Developing the clinical judgement to recognise and act on obesity wherever it appears is as important as knowing the technical elements of the history and examination.
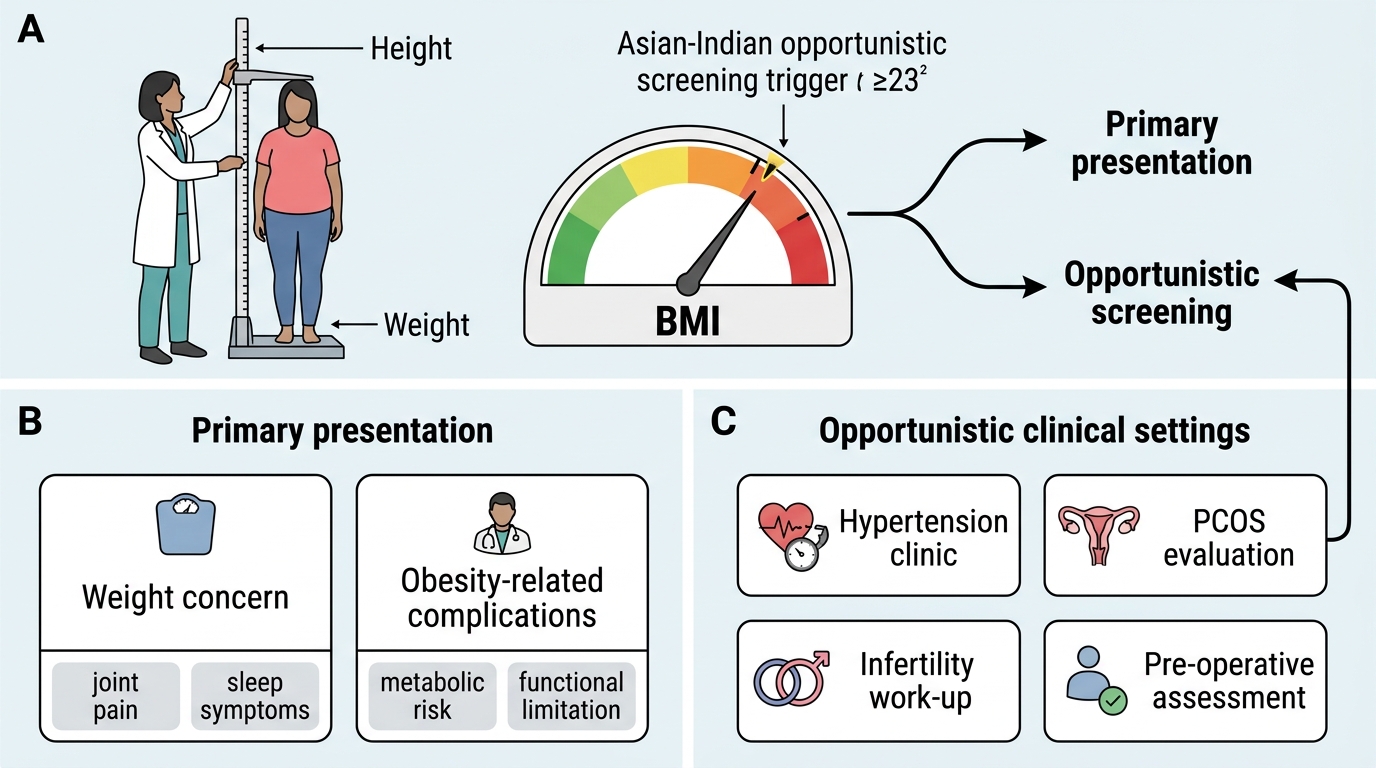
The primary indication is the straightforward presentation: a patient who comes because of weight — seeking advice on weight loss, referred by another clinician, or presenting with a complication (breathlessness, knee pain, snoring, irregular periods) that the clinician must connect to adiposity. In these cases, a full structured obesity evaluation is clearly warranted and the patient has already accepted that weight is part of the consultation.
A more challenging and clinically important scenario is opportunistic identification: a patient presents for an unrelated reason (hypertension, back pain, infertility, mood disorder) and you observe that BMI is elevated. The clinical decision to raise obesity in this consultation requires tact, patient-centredness, and situational awareness — raising weight as an issue uninvited can damage the therapeutic relationship if done clumsily. Current best practice supports brief opportunistic intervention (raising it once, inviting the patient's readiness to discuss, not moralising) in any patient with BMI ≥23 kg/m² (Asian-Indian threshold) who presents for any reason.
Indicators that a full obesity evaluation is warranted regardless of the chief complaint:
- BMI ≥25 kg/m² (obese by Asian-Indian criteria) at any consultation
- Waist circumference ≥90 cm (men) or ≥80 cm (women) detected on routine examination
- Two or more metabolic syndrome components present on routine investigations
- Presentation with a complication strongly linked to obesity: T2DM, hypertension, dyslipidaemia, OSA, NAFLD, PCOS, knee/hip osteoarthritis
- Unexplained rapid weight gain (≥5 kg in 6 months) which may signal a secondary cause
- Pre-operative assessment for any major procedure (obesity increases anaesthetic and surgical risk)
- Reproductive consultation: infertility, PCOS, obstetric care
Clinical Indications for Obesity Evaluation
History Taking in Obesity: Structure and Key Domains
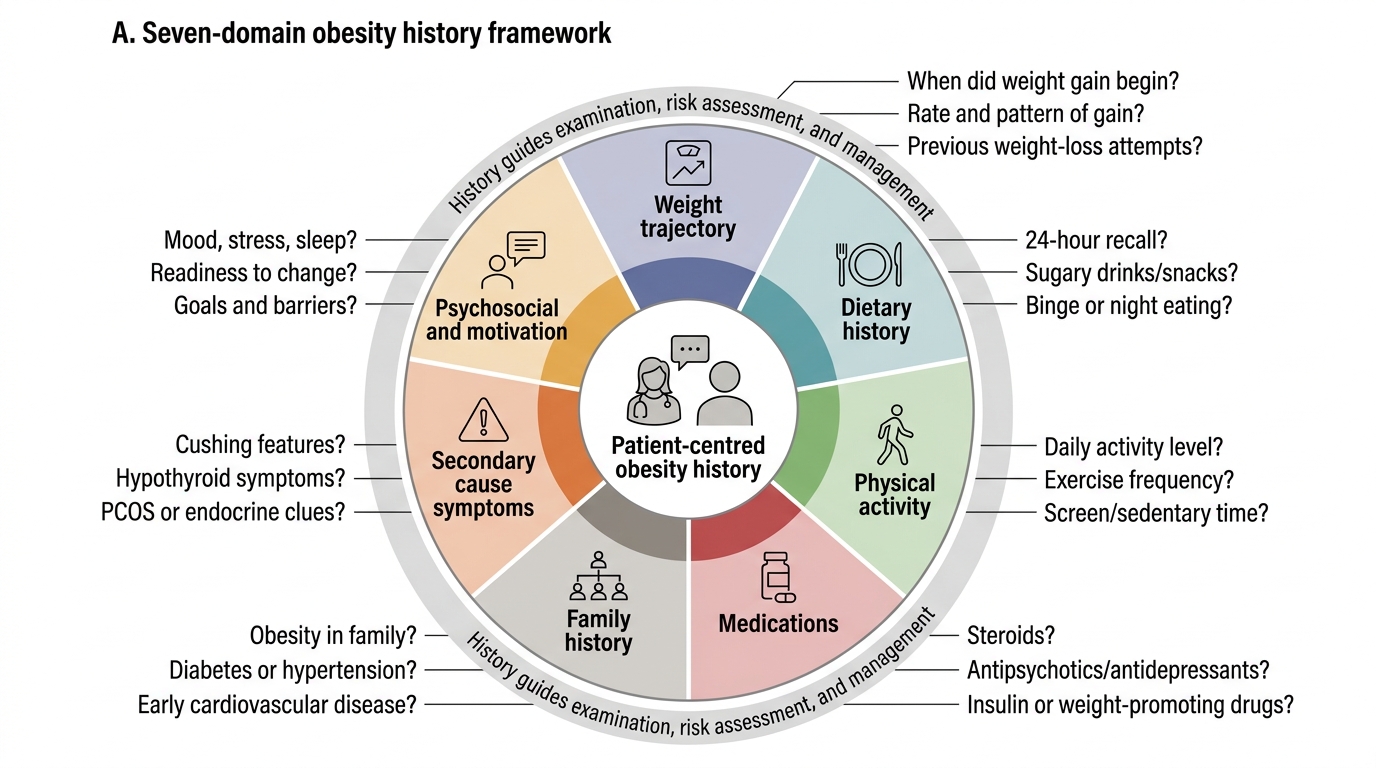
The obesity history is structured around seven domains, each serving a distinct purpose. A skilled clinician moves fluidly between these domains in a patient-centred conversational style, but the underlying structure ensures that no clinically important dimension is missed. The history must accomplish: establishing the trajectory (when, how fast, what precipitated), identifying contributing factors (dietary, activity, medications, psychological), screening for secondary causes (endocrine, hypothalamic), assessing current complications, and — critically — gauging the patient's readiness and motivation to change, which determines what kind of help will actually be accepted.
Domain 1 — Weight history and trajectory:
Begin with an open question: 'Can you tell me about your weight over the years?' Key questions: What is the patient's highest and lowest adult weight? When did the weight gain begin? Was the onset gradual (years, consistent with lifestyle/genetic obesity) or sudden/rapid (months, raising the suspicion of secondary causes such as hypothyroidism or Cushing syndrome, or medication effect)? Were there identifiable triggers — pregnancy, relationship stress, bereavement, change in job, stopping smoking, starting a new medication? A progressive gain since childhood suggests polygenic predisposition or an early secondary cause; a gain beginning abruptly in a previously weight-stable adult demands secondary cause screening.
Domain 2 — Dietary history:
A 24-hour dietary recall provides a useful starting estimate. Ask: what does the patient typically eat for breakfast, lunch, dinner, and snacks? Note portion sizes, meal frequency, eating out frequency, sugar-sweetened beverage intake, alcohol (liquid calories are underestimated), late-night eating (associated with metabolic risk independent of total calories), and emotional eating patterns. Ask whether hunger is present between meals, and whether the patient feels they eat for hunger or for other reasons (stress, boredom, habit). In the Indian context, ask specifically about refined carbohydrate staples (white rice, chapati), oil consumption in cooking, and use of street food or ultra-processed snacks.
Domain 3 — Physical activity history:
Assess both structured exercise and lifestyle physical activity. 'Do you do any exercise?' is a start, but 'How much walking do you do in a typical day?' and 'What is your job — do you sit most of the day?' give richer information. Enquire about barriers: time, physical limitations (knee pain, breathlessness limiting exertion), cost, safety (can they walk in their neighbourhood?), and previous attempts at exercise. The WHO target is ≥150 minutes/week moderate-intensity — ask if they currently meet it.
Domain 4 — Medical and medication history:
Review all current medications with specific attention to those that promote weight gain: corticosteroids (route and dose matter), antipsychotics (olanzapine and clozapine are the worst offenders), antidepressants (mirtazapine, TCAs), insulin and sulphonylureas, thiazolidinediones, valproate, lithium, and beta-blockers. A medication-induced 8–12 kg weight gain is clinically meaningful and potentially reversible. Also review for obesity-related comorbidities already diagnosed: diabetes, hypertension, dyslipidaemia, OSA, PCOS, NAFLD, GORD, osteoarthritis.
Domain 5 — Family history:
A positive family history of obesity, T2DM, and cardiovascular disease is both a risk indicator and a basis for prognostic counselling. Ask specifically about parents and siblings. A strong family history in a patient with severe early-onset obesity prompts consideration of monogenic or syndromic forms.
Domain 6 — Symptoms of secondary causes (must not be missed):
Systematically screen for:
- Hypothyroidism: fatigue, cold intolerance, constipation, dry skin, hair loss, menstrual irregularity, low mood, slow speech
- Cushing syndrome: easy bruising, proximal muscle weakness (difficulty rising from a chair, climbing stairs), new-onset hypertension, mood change, striae
- PCOS: oligomenorrhea/amenorrhoea, hirsutism (facial, chest, abdomen), acne, infertility
- OSA: snoring, witnessed apnoeas, daytime somnolence (Epworth Sleepiness Scale ≥10), morning headache, nocturia
- Hypothalamic obesity: headache, visual field changes, prior pituitary surgery, cranial radiotherapy, hyperphagia out of proportion to weight
Domain 7 — Psychosocial and motivational assessment:
This domain is often omitted under time pressure but is the most predictive of treatment success. Ask about the patient's understanding of their weight problem, previous weight loss attempts (what worked, what didn't, why), support at home, food security (can they afford healthier foods?), mental health (depression and anxiety are bidirectionally linked to obesity), work schedule (night shifts, sedentary jobs), and — most importantly — readiness to change. The Stages of Change (Transtheoretical) model provides a practical framework: pre-contemplation (not aware or not ready), contemplation (aware but ambivalent), preparation (planning to change), action, and maintenance. Matching your intervention to the patient's stage prevents mismatched advice that the patient cannot implement.
Seven-Domain Obesity History Framework
Physical Examination: Systematic Approach and Key Findings
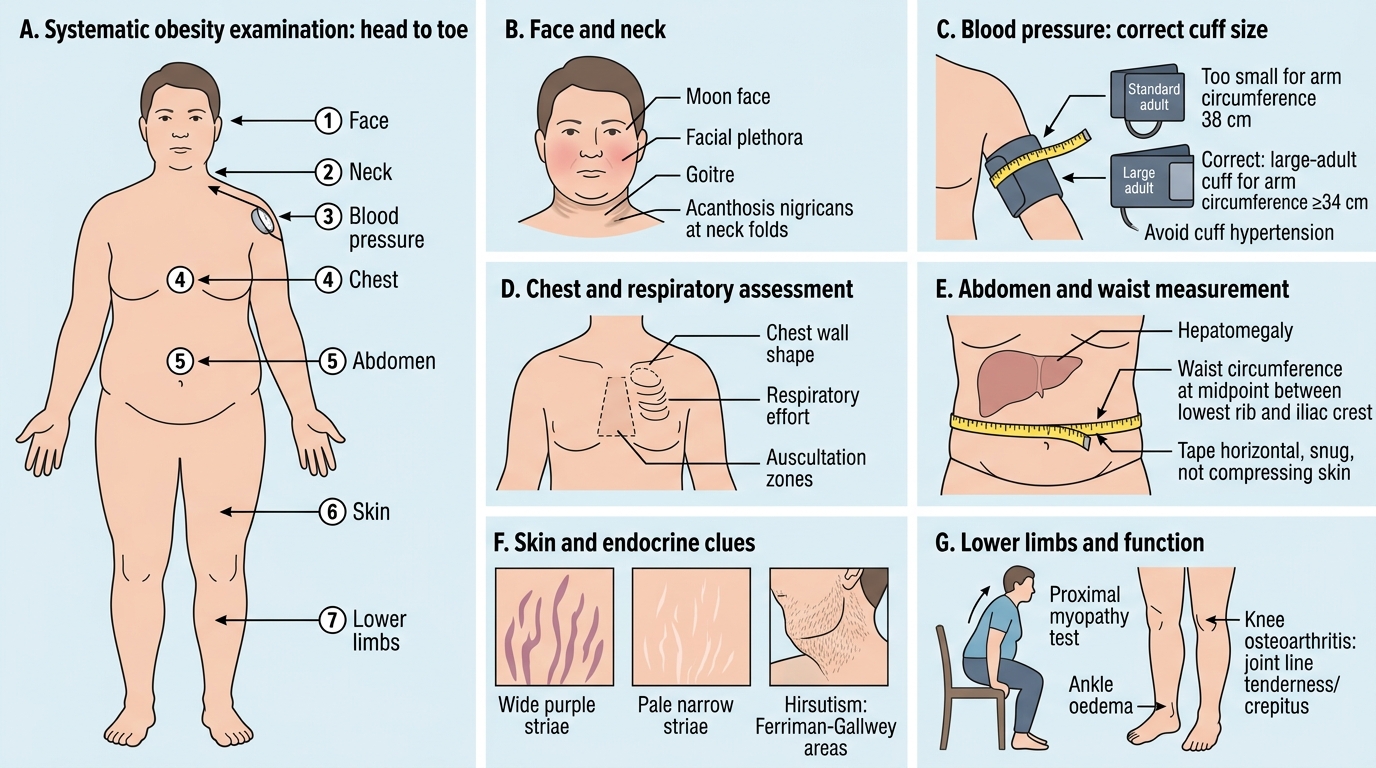
The physical examination in obesity is not a passive observation of weight but a purposeful, structured search for signs of secondary causes, obesity-related complications, and the metabolic markers that define risk. It should be performed sensitively — a patient-centred approach that preserves dignity and avoids implicit or explicit weight stigma. The examination proceeds in a logical sequence from general inspection to targeted organ system assessment.
General inspection and vital signs:
Note body habitus distribution: generalised obesity (uniform fat deposition, typical of dietary/genetic obesity) versus central/truncal adiposity with thin limbs (Cushing syndrome, hypothyroidism, lipodystrophy). Measure height and weight with calibrated instruments; calculate BMI. Assess distribution at the face: moon face (rounded, plethoric, facial fullness — Cushing syndrome) versus generalised facial fullness. Note skin colour (plethora = Cushing; pallor/carotenodermia = hypothyroidism). Vital signs: blood pressure (measure with an appropriately sized cuff — a standard cuff on a large arm will give falsely elevated readings; use a large-sized or thigh cuff if arm circumference >34 cm), heart rate (bradycardia in hypothyroidism), respiratory rate and oxygen saturation at rest (low SaO2 at rest suggests OSA/OHS).
Anthropometric measurements — technique and interpretation:
- BMI: weight (kg) / height² (m²). Classify using Asian-Indian cut-offs: overweight ≥23, obese ≥25 kg/m².
- Waist circumference: measured at the end of a gentle expiration, at the mid-point between the lower rib margin and the iliac crest, with the measuring tape horizontal and snug but not compressing the skin. Cut-offs for Asian Indians: men ≥90 cm = central obesity; women ≥80 cm = central obesity.
- Hip circumference: measured at the widest point of the buttocks. Calculate waist-to-hip ratio (WHR): action cut-offs WHR >0.90 (men), >0.85 (women).
- Neck circumference: ≥40 cm (men) or ≥35 cm (women) is associated with OSA risk.
Skin examination:
- Acanthosis nigricans: velvety, hyperpigmented, thickened skin at the nape of the neck, axillae, and groin — a reliable cutaneous marker of insulin resistance and hyperinsulinaemia. Note its distribution (neck and axillae most common; also under the breasts and groin). Bilateral, symmetrical distribution with a velvety texture is typical of metabolic acanthosis; unilateral or warty acanthosis in an older patient raises the concern of paraneoplastic origin.
- Striae: purple/violaceous, wide (>1 cm) striae on the abdomen, flanks, thighs, or axillae are a red-flag sign of Cushing syndrome (due to rapid skin stretching with protein catabolism); narrow, silvery striae are non-specific and can occur with any rapid weight gain.
- Hirsutism: excess terminal hair in a male-distribution pattern (upper lip, chin, sideburns, chest, linea alba, inner thighs) in women — assess using the modified Ferriman-Gallwey score (>8 is abnormal); suggests hyperandrogenism (PCOS most commonly; also Cushing syndrome, congenital adrenal hyperplasia).
- Easy bruising, thin skin, poor wound healing: features of Cushing syndrome.
Cardiovascular and respiratory examination:
Blood pressure (bilateral arm, correct cuff size). Peripheral pulses. Precordial examination for displaced apex beat (left ventricular hypertrophy from hypertension or obesity cardiomyopathy). Respiratory: basal dullness and reduced air entry (raised diaphragm, pleural effusions); assess for signs of pulmonary hypertension (right ventricular heave, loud P2, raised JVP) in patients with severe OSA or OHS.
Abdominal examination:
Hepatomegaly (smooth, mildly tender in NAFLD); splenomegaly if cirrhosis is advanced. Assess for ovarian enlargement and uterine abnormality in women with PCOS (though pelvic ultrasound is more reliable). Assess for tenderness in the right upper quadrant.
Neurological and musculoskeletal:
Proximal muscle weakness (Cushing syndrome): test by asking the patient to rise from a seated position without using hands, or to raise both arms above the head — difficulty suggests proximal myopathy. Assess knee and hip joints for signs of osteoarthritis: crepitus, restricted range of motion, tenderness. Assess ankle oedema.
Thyroid examination:
Palpate for goitre (diffuse or nodular); note voice quality (hoarse in hypothyroidism), deep tendon reflexes (delayed relaxation in hypothyroidism — elicit ankle jerk), dry coarse skin, and peripheral oedema (pretibial myxoedema).
Systematic Obesity Examination Checklist
SELF-CHECK
A 35-year-old woman with obesity has her blood pressure measured as 152/94 mmHg using a standard adult cuff. Her arm circumference is 38 cm. The correct next step is:
A. Record the reading as Stage 2 hypertension and initiate antihypertensive therapy
B. Repeat the measurement after 5 minutes of rest with the same cuff
C. Repeat the measurement using a large-adult cuff (arm circumference ≥34 cm requires a large cuff) to eliminate cuff error
D. Measure blood pressure in both arms to exclude coarctation of the aorta
Reveal Answer
Answer: C. Repeat the measurement using a large-adult cuff (arm circumference ≥34 cm requires a large cuff) to eliminate cuff error
A standard adult cuff (bladder 12–13 cm wide) under-cuffs a large arm, falsely elevating the reading — the technical term is 'cuff hypertension.' When arm circumference exceeds ~34 cm, a large-adult or wide cuff (bladder 15–16 cm) must be used. Recording a cuffed-up reading as hypertension would lead to unnecessary investigation and medication. Repeating with the same cuff does not address the error. Bilateral measurement is useful for detecting coarctation but that is not the primary issue here. The correct action is to remeasure with an appropriately sized large-adult cuff.