Page 6 of 15
IM14.6-10 | Obesity Clinical Evaluation — SDL Guide (Part 2)
Differential Diagnosis and Prioritisation
The differential diagnosis in the clinical evaluation of obesity is structured around two questions: what type of obesity is this (primary multifactorial vs secondary), and what complications are already present? Generating a complete and prioritised differential diagnosis requires integrating the history, examination findings, and risk context — and the ability to flag the red-flag features that demand urgent investigation.
Provided image
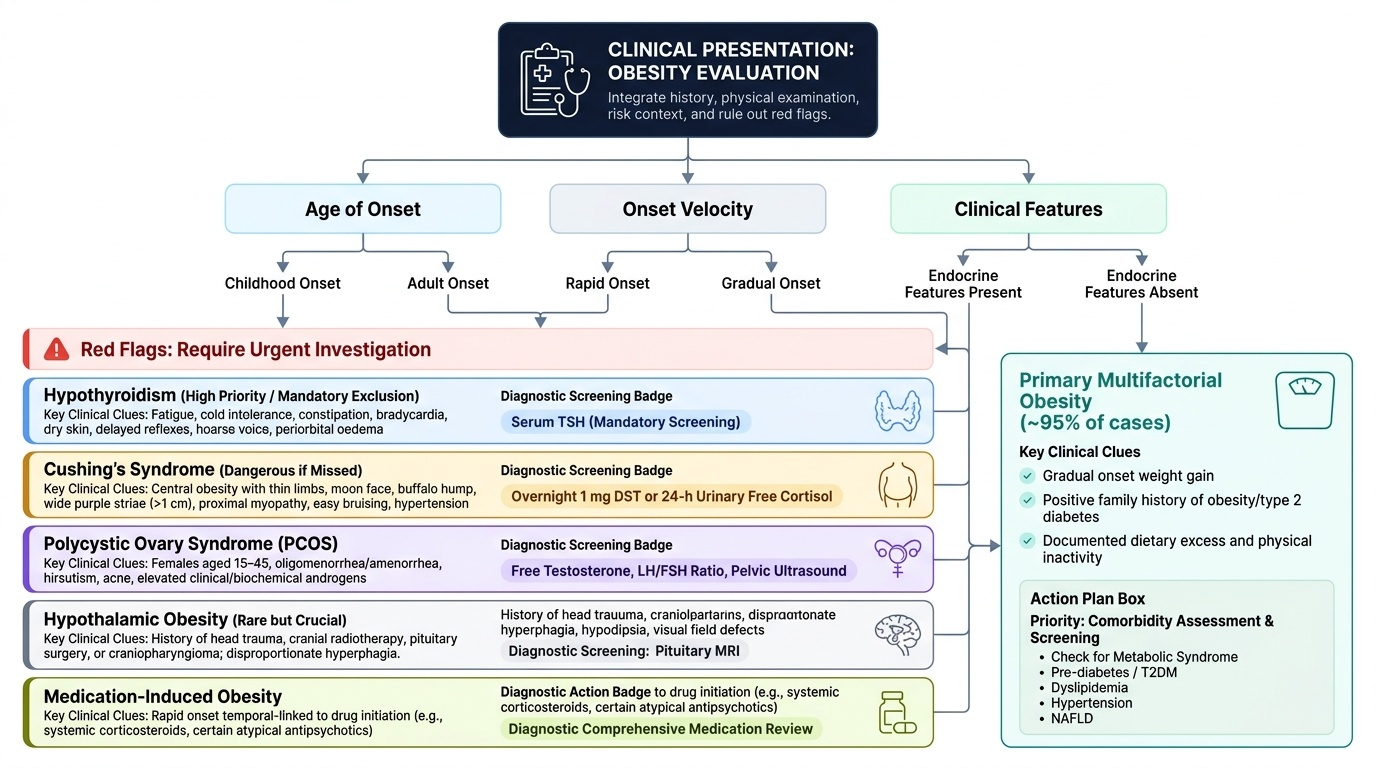
For the most common presentation — an adult with gradually progressive obesity and a family history of obesity and diabetes — the working diagnosis is primary multifactorial obesity with likely comorbidities (metabolic syndrome, pre-diabetes or T2DM, dyslipidaemia, hypertension, NAFLD). However, this diagnosis must remain provisional until secondary causes have been excluded. The fundamental clinical error is to attribute obesity to lifestyle without first ruling out a treatable endocrine cause.
Prioritised differential for new-onset or progressive obesity:
- Primary multifactorial obesity — most common (>95%); gradual onset, family history positive, no specific endocrine features, dietary excess and inactivity documented. Comorbidity assessment is the priority.
- Hypothyroidism — second most important to exclude; clinical features: cold intolerance, constipation, fatigue, bradycardia, dry skin, hoarse voice, delayed reflexes, periorbital oedema. Serum TSH is the screening test; mandatory in all new obesity presentations.
- Cushing syndrome — less common but dangerous if missed; clinical features: central obesity with thin limbs, moon face, buffalo hump, purple/wide striae (>1 cm), proximal myopathy, easy bruising, hypertension, hyperglycaemia, hypogonadism. Suspect in any patient where these features are present; screen with overnight 1 mg DST or 24-h urinary free cortisol.
- PCOS — common in women aged 15–45 with obesity; features: oligomenorrhea/amenorrhea, hirsutism, acne, elevated androgens, polycystic ovaries on ultrasound. Screen with free testosterone, LH/FSH ratio, pelvic ultrasound.
- Hypothalamic obesity — rare but important; features: preceding head trauma, cranial radiotherapy, pituitary surgery, or history of craniopharyngioma; disproportionate hyperphagia, hypodipsia, visual field defects; pituitary MRI required.
- Medication-induced obesity — look carefully at the drug list; corticosteroids (any route), antipsychotics, antidepressants, insulin, sulphonylureas, valproate, lithium.
- Monogenic/syndromic obesity — suspect in early-onset severe childhood obesity with constant hyperphagia; syndromic features (intellectual disability, retinal dystrophy, polydactyly) suggest Bardet-Biedl or Prader-Willi.
Red-flag features requiring urgent workup:
- Rapid weight gain (>5 kg in 3 months) without obvious dietary cause
- Purple striae >1 cm width, proximal myopathy, easy bruising → Cushing syndrome
- Headache, visual field defect, and rapid weight gain → hypothalamic lesion
- Episodic hypoglycaemia with weight gain → insulinoma
- Obese child with intellectual disability and visual symptoms → syndromic obesity
Ordering and Interpreting Investigations
Investigations in the clinical evaluation of obesity serve two distinct purposes: first, excluding secondary causes that would otherwise go untreated while the clinician pursues a lifestyle-based management plan that cannot address the underlying hormonal driver; and second, quantifying established comorbidities that define the patient's cardiometabolic risk tier and determine the intensity and urgency of intervention. The selection of tests must be driven by clinical probability derived from the history and examination — not by a standing protocol ordering the same battery for every obese patient. Ordering a dexamethasone suppression test on a patient with no Cushingoid features and a 20-year history of gradual weight gain is not evidence-based and adds cost, anxiety, and occasional false-positive results. Conversely, missing a TSH in a patient with rapid weight gain, constipation, and bradycardia because 'she eats a lot' is a clinical error of omission. This section provides a structured framework for selecting investigations by clinical probability and interpreting each test class in the context of obesity.
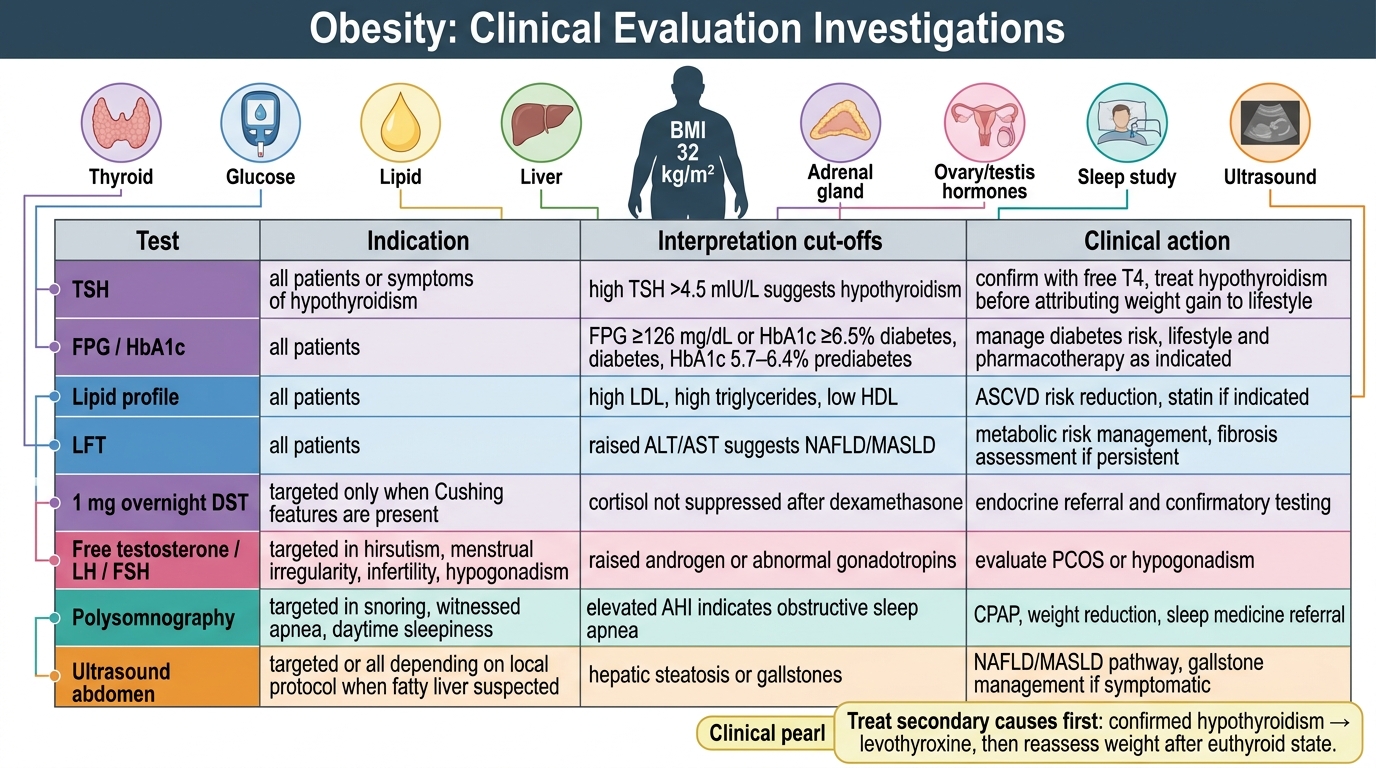
Mandatory baseline investigations in all patients with obesity:
- Serum TSH: the single most important test; elevated TSH (>4.5 mIU/L) confirms primary hypothyroidism. If TSH is normal, thyroid disease is effectively excluded and no further thyroid testing is needed unless clinical suspicion is very high.
- Fasting plasma glucose (FPG) or HbA1c: to detect diabetes (FPG ≥126 mg/dL, HbA1c ≥6.5%) or pre-diabetes (FPG 100–125 mg/dL = impaired fasting glucose; HbA1c 5.7–6.4%). If both FPG and HbA1c are inconclusive, a 75 g OGTT (2-hour plasma glucose ≥200 mg/dL = diabetes; 140–199 = impaired glucose tolerance) provides definitive classification.
- Fasting lipid profile: TG, LDL, HDL, total cholesterol. Assess for dyslipidaemia and metabolic syndrome components.
- Liver function tests (LFT) + ALT/AST: elevated transaminases suggest NAFLD/NASH; ALT is more sensitive than AST for fatty liver. ALT:AST ratio <1 suggests fatty liver; ratio >2 in the presence of elevated GGT suggests alcoholic hepatitis.
- Serum uric acid: hyperuricaemia is common in metabolic syndrome and predisposes to gout.
- Complete blood count: to detect anaemia (which may contribute to fatigue attributed to obesity) or polycythaemia (OSA/OHS).
- Renal function (serum creatinine, eGFR, spot urine albumin-creatinine ratio): obesity-related glomerulopathy; hypertension-related CKD.
- ECG: left ventricular hypertrophy (voltage criteria + strain pattern), arrhythmias.
Targeted investigations for secondary causes:
- 1 mg overnight dexamethasone suppression test (DST): administer 1 mg oral dexamethasone at 11 PM; measure serum cortisol at 8 AM next morning. Normal response: cortisol <50 nmol/L (suppressed). Failure to suppress = possible Cushing syndrome → refer for 24-h urinary free cortisol and endocrinology review. Note: false positives occur with depression, alcoholism, obesity itself (mild non-suppression), and concurrent enzyme-inducing drugs.
- Free testosterone, DHEAS, LH/FSH: in women with oligomenorrhea, hirsutism, or acne; elevated free testosterone + LH:FSH >2:1 + polycystic ovaries on ultrasound supports PCOS diagnosis (Rotterdam criteria: 2 of 3).
- Fasting insulin and HOMA-IR (homeostatic model assessment of insulin resistance): HOMA-IR = [fasting insulin (μU/mL) × fasting glucose (mmol/L)] / 22.5; value >2.5 indicates insulin resistance. Not a diagnostic test for diabetes, but useful for quantifying metabolic risk and guiding pharmacotherapy decisions.
- Polysomnography (sleep study): indicated if OSA suspected (snoring, witnessed apnoeas, Epworth Sleepiness Scale ≥10, neck circumference ≥40/35 cm, BMI >30). Confirms OSA, grades severity by apnoea-hypopnoea index (AHI): mild 5–14, moderate 15–30, severe >30 events/hour.
- Ultrasound abdomen: assess hepatic echogenicity (bright liver = steatosis), liver size, and grade of fatty infiltration. Can also assess ovarian morphology (PCOS: ≥20 follicles per ovary or ovarian volume >10 mL).
- MRI pituitary: if Cushing confirmed or if hypothalamic obesity suspected.
Interpreting findings in context:
A fasting glucose of 112 mg/dL = impaired fasting glucose (pre-diabetes) — this patient needs lifestyle intervention and reassessment in 3 months; not yet diabetes, but clinically actionable. Serum ALT 62 IU/L in an obese patient without alcohol use = probable NAFLD; add ultrasound abdomen to grade steatosis and counsel on weight loss. Serum TSH 7.8 mIU/L in an obese patient = primary hypothyroidism — treat with levothyroxine before attributing all weight gain to lifestyle; repeat TSH in 6–8 weeks after dose titration.
Investigations in Clinical Evaluation of Obesity
SELF-CHECK
A 38-year-old woman with BMI 32 kg/m² has serum TSH 6.2 mIU/L (normal 0.5–4.5). She has fatigue, weight gain of 9 kg over 12 months, constipation, and cold intolerance. The most appropriate next step after confirming primary hypothyroidism is:
A. Refer directly to a dietitian for a calorie-restricted diet and exercise programme
B. Start levothyroxine replacement and reassess her weight after achieving a euthyroid state before attributing residual weight gain to lifestyle
C. Order a 24-h urinary free cortisol to exclude co-existing Cushing syndrome
D. Start anti-obesity pharmacotherapy with a GLP-1 receptor agonist immediately
Reveal Answer
Answer: B. Start levothyroxine replacement and reassess her weight after achieving a euthyroid state before attributing residual weight gain to lifestyle
This patient has confirmed primary hypothyroidism (elevated TSH with classical clinical features), which is a secondary cause of obesity. The correct approach is to treat the underlying cause first — levothyroxine replacement. Weight gain attributable to hypothyroidism may partially reverse once euthyroidism is achieved. It is inappropriate to begin lifestyle or pharmacological weight management before addressing the secondary cause, as the patient would be managed for the wrong problem. Cushing syndrome screening is not the immediate priority when hypothyroidism has been confirmed as the explanation. GLP-1 agonists for obesity are not indicated until secondary causes have been treated and any residual obesity assessed.
Tests for Secondary Causes: Indications and Interpretation
Identifying secondary causes of obesity requires a clinician to move beyond opportunistic screening (always doing TSH) to a more sophisticated pattern-recognition approach where the clinical features encountered in the history and examination trigger specific targeted investigations. This section consolidates the clinical features, investigation selection, and result interpretation for the three most important secondary causes encountered in Indian practice.
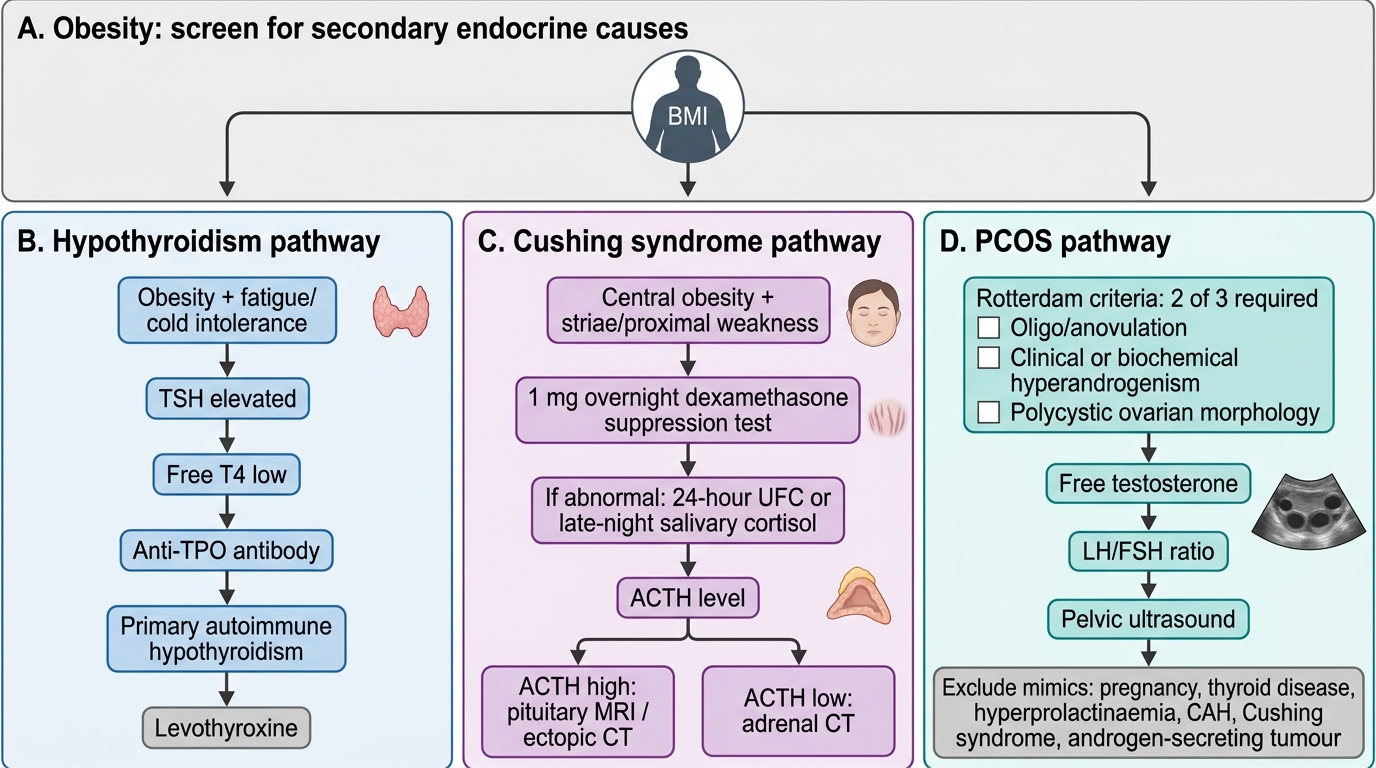
Hypothyroidism — detailed interpretation:
Primary hypothyroidism is caused by thyroid gland failure (most commonly autoimmune thyroiditis, previously termed Hashimoto's thyroiditis). TSH is the most sensitive test: it rises before free T4 (fT4) falls, because the pituitary responds to even subtle falls in thyroid hormone. A TSH >4.5 mIU/L with low fT4 confirms overt hypothyroidism — initiate levothyroxine. A TSH 4.5–10 mIU/L with normal fT4 = subclinical hypothyroidism — treat if: the patient has symptoms, anti-TPO antibodies are positive (indicating autoimmune origin and higher risk of progression to overt hypothyroidism), cholesterol is elevated, or the patient is attempting pregnancy. Anti-TPO antibodies confirm autoimmune aetiology and predict progression. Dose of levothyroxine: approximately 1.6 mcg/kg/day lean body weight; start low (25–50 mcg/day) in elderly or patients with cardiac disease; titrate to TSH within the reference range every 6–8 weeks.
Cushing syndrome — detailed interpretation:
Cushing syndrome results from excess cortisol — from exogenous corticosteroids (most common cause in practice, iatrogenic) or from endogenous overproduction (pituitary ACTH-secreting adenoma = Cushing disease, 70%; adrenal adenoma/carcinoma, 15%; ectopic ACTH, 15%). Clinical features that strongly predict Cushing syndrome (high specificity): easy bruising, proximal myopathy, wide purple striae (>1 cm), facial plethora, and new-onset diabetes or hypertension in a young patient. The initial test is the 1 mg overnight DST: give 1 mg dexamethasone orally at 11 PM, measure cortisol at 8 AM — cortisol <50 nmol/L = suppressed (Cushing excluded); cortisol >138 nmol/L = fail (Cushing probable); 50–138 = grey zone, repeat with 24-h urinary free cortisol (>3× upper limit of normal confirms Cushing). If confirmed, plasma ACTH levels distinguish ACTH-dependent (elevated ACTH = pituitary or ectopic) from ACTH-independent (suppressed ACTH = adrenal) Cushing — which then directs imaging (MRI pituitary vs CT adrenals).
PCOS — detailed interpretation:
PCOS is the most common endocrine disorder in women of reproductive age and a major cause of secondary obesity, anovulatory infertility, and metabolic syndrome in women. The Rotterdam 2003 diagnostic criteria (revised, most widely used) require 2 of 3:
1. Oligo- or anovulation (irregular or absent menstrual cycles)
2. Clinical or biochemical hyperandrogenism (hirsutism on modified Ferriman-Gallwey ≥8, or elevated free testosterone, or elevated DHEAS)
3. Polycystic ovarian morphology on ultrasound (≥20 follicles per ovary, 2–9 mm diameter, in the absence of a dominant follicle/corpus luteum, OR ovarian volume >10 mL)
Biochemical hyperandrogenism: free testosterone is more sensitive than total testosterone; DHEAS elevation suggests adrenal androgen excess. LH:FSH ratio >2:1 supports PCOS but is neither required nor sufficient. AMH (anti-Müllerian hormone) is elevated in PCOS and correlates with ovarian follicle count. Exclude other causes of androgen excess before diagnosing PCOS: 17-hydroxyprogesterone (late-onset congenital adrenal hyperplasia), 24-h urinary free cortisol (Cushing), prolactin (hyperprolactinaemia), and TSH (hypothyroidism can cause menstrual irregularity mimicking PCOS).
Diagnostic Algorithm for Secondary Causes of Obesity
SELF-CHECK
A 28-year-old woman has oligomenorrhoea, facial hirsutism (modified Ferriman-Gallwey score 11), and BMI 28 kg/m² (obese by Asian-Indian criteria). Pelvic ultrasound shows 22 follicles in the right ovary and 18 in the left, ovarian volume 12 mL bilaterally. Serum TSH is normal. Her serum free testosterone is elevated. How many of the Rotterdam 2003 criteria does she meet?
A. One criterion only (hyperandrogenism) — ultrasound alone is insufficient
B. Two criteria: oligomenorrhoea and biochemical hyperandrogenism (free testosterone elevated)
C. All three Rotterdam criteria: oligo/anovulation, hyperandrogenism (clinical Ferriman-Gallwey ≥8 plus elevated free testosterone), and polycystic ovarian morphology on ultrasound
D. None — the diagnosis requires all three criteria to be met, not just two
Reveal Answer
Answer: C. All three Rotterdam criteria: oligo/anovulation, hyperandrogenism (clinical Ferriman-Gallwey ≥8 plus elevated free testosterone), and polycystic ovarian morphology on ultrasound
The Rotterdam 2003 criteria require 2 of 3: (1) oligo/anovulation — YES (oligomenorrhoea is present); (2) clinical or biochemical hyperandrogenism — YES (both clinical: Ferriman-Gallwey score 11 ≥8, and biochemical: elevated free testosterone); (3) polycystic ovarian morphology on ultrasound — YES (≥20 follicles per ovary OR volume >10 mL; she has 22+18 follicles and volume 12 mL bilaterally). She therefore meets ALL three criteria. The diagnosis requires only 2 of 3, so she would qualify with any two — but in this case all three are present. Note: the Rotterdam diagnosis of PCOS requires exclusion of other androgen-excess causes, and TSH is already normal.
CLINICAL PEARL
The most common technical error in the obesity physical examination is using an incorrectly sized blood pressure cuff. A standard cuff on an arm circumference >34 cm will over-read by 5–10 mmHg, leading to misdiagnosis of hypertension and unnecessary treatment. Always select cuff size based on measured arm circumference: standard adult (27–34 cm), large adult (35–44 cm), extra-large or thigh cuff (>44 cm). This simple check prevents the misdiagnosis of cuff hypertension.
The second most common omission is failing to measure waist circumference. A patient with a BMI of 24 kg/m² (borderline overweight by Asian-Indian standards) may have a waist circumference of 95 cm — placing him in the metabolic syndrome central obesity category and warranting the full metabolic workup. BMI and waist circumference must both be measured and documented at every obesity-related consultation. They are not interchangeable; they measure different things.
Self-Assessment: Integrating the Obesity Clinical Evaluation
The following clinical scenarios require you to integrate all five elements of the obesity evaluation: recognising the indication, taking a targeted history, performing a focused examination, generating a prioritised differential, and selecting appropriate investigations. Work through each before reading the analysis.
Scenario A: A 44-year-old woman presents with a 3-year history of progressive weight gain (currently 94 kg, height 162 cm). She reports fatigue, cold intolerance, and constipation. On examination: BMI 35.8 kg/m², waist 98 cm, heart rate 56/min, reflexes delayed (ankle jerk relaxation phase slow), dry coarse skin, non-pitting periorbital oedema, small smooth goitre. BP 142/88 mmHg. What is the most likely secondary cause, the key diagnostic test, and the immediate treatment priority?
Analysis: The symptom cluster (fatigue, cold intolerance, constipation) plus signs (bradycardia, delayed reflexes, dry coarse skin, periorbital oedema, goitre) are classical for hypothyroidism. Key diagnostic test: serum TSH (expected to be elevated). Treatment priority: initiate levothyroxine replacement, titrate to normalise TSH, then reassess residual obesity after euthyroidism is achieved. Do not start a weight loss programme until the thyroid disorder is treated. Also check anti-TPO antibodies and fasting lipids (hypothyroidism causes dyslipidaemia).
Scenario B: A 32-year-old man presents with obesity, new-onset hypertension, and type 2 diabetes diagnosed 6 months ago. His GP assumed lifestyle-related obesity. On review: BMI 31 kg/m², but waist is only 86 cm (below the 90 cm Asian-Indian threshold for men — his adiposity is more generalised). On examination: mild proximal muscle weakness (difficulty rising from chair without using hands), facial plethora, easy bruising on the arms, and a 2 cm wide purple/violaceous striae over the abdomen. What secondary cause must be excluded urgently?
Analysis: The combination of rapid-onset obesity, hypertension, diabetes in a young man PLUS proximal myopathy, easy bruising, and wide purple striae constitutes a classic Cushing syndrome presentation. This requires urgent workup. Screen with 1 mg overnight DST and 24-h urinary free cortisol. Do not defer secondary cause investigation in the presence of these red-flag features. If confirmed, measure plasma ACTH (to distinguish ACTH-dependent vs independent), and arrange MRI pituitary.
Scenario C: A 26-year-old woman presents for evaluation of obesity (BMI 27 kg/m², waist 85 cm — both above Asian-Indian thresholds) with irregular cycles (1–2 per year) and unwanted facial and chest hair. Serum TSH is normal. She is concerned about fertility. What history details, examination findings, and investigations complete the evaluation?
Analysis: PCOS is the leading differential. History: duration of menstrual irregularity, acne, previous pregnancy attempts, medications, family history (first-degree relatives with PCOS or T2DM). Examination: quantify hirsutism with modified Ferriman-Gallwey score; check for acanthosis nigricans (insulin resistance); blood pressure. Investigations: free testosterone, DHEAS, LH/FSH, pelvic ultrasound (follicle count and ovarian volume), fasting glucose/HOMA-IR (insulin resistance assessment), fasting lipids (metabolic syndrome screening). Exclude late-onset CAH (17-OHP), Cushing syndrome, and hyperprolactinaemia. Management: weight loss (even 5% improves cycle regularity and fertility); consider OCP for symptom management or ovulation induction if fertility is desired.
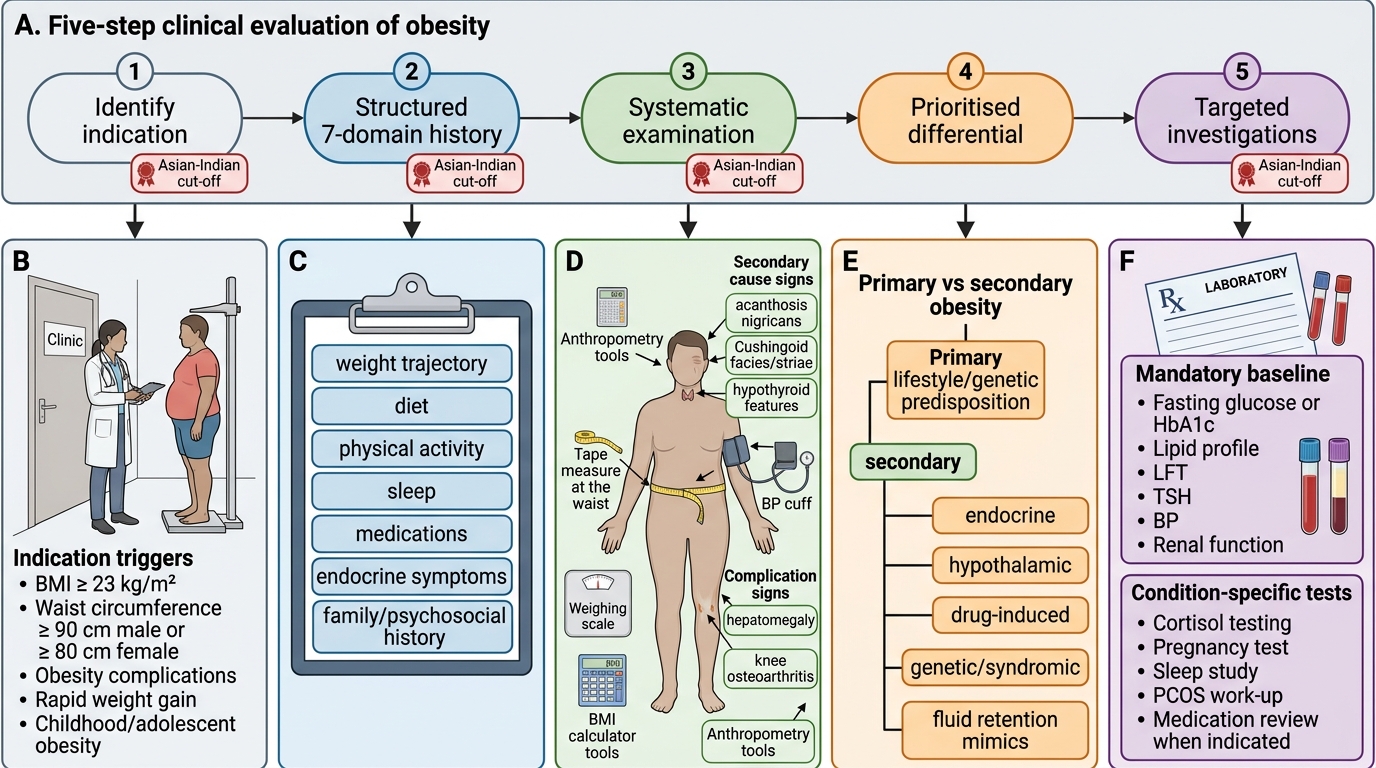
Five-Step Clinical Evaluation of Obesity