Page 2 of 15
IM14.1-5 | Obesity Foundations — SDL Guide (Part 2)
Environmental and Behavioural Determinants of Obesity
The global obesity epidemic cannot be explained by genetics alone — the gene pool has not changed dramatically in three decades, yet obesity prevalence has tripled. The driving force is the obesogenic environment: a constellation of food, activity, economic, and social factors that promote energy surplus. Understanding these determinants is essential not only for individual counselling but for designing effective public health interventions at a population level.
Dietary patterns and food environment:
India's nutrition transition has accelerated sharply since liberalisation in 1991. Key drivers include urbanisation (which increases reliance on processed and restaurant food), the proliferation of ultra-processed foods (UPFs) with high energy density and poor satiety signalling, marketing of sugar-sweetened beverages (SSBs), and declining consumption of traditional high-fibre staples. SSBs deserve special mention: liquid calories do not generate the same satiety response as solid food calories, and fructose in soft drinks preferentially drives hepatic de novo lipogenesis (fat production in the liver), contributing to fatty liver, dyslipidaemia, and insulin resistance independent of total caloric load. Refined carbohydrates (white rice, maida) produce rapid glycaemic spikes followed by compensatory hyperinsulinaemia, driving subsequent hunger and fat deposition.
Physical activity and built environment:
Modern occupational shifts — from physically demanding agricultural and manual labour to desk-based IT and service sector work — have dramatically reduced occupational energy expenditure. Commuting by personal vehicle replaces walking; elevators replace stairs. In India, the ICMR-INDIAB study found that 54% of adults do not meet the WHO recommendation of 150 minutes/week of moderate-intensity physical activity. Importantly, sedentary time (total hours spent sitting) is an independent risk factor for cardiometabolic disease even after accounting for exercise minutes — the 'active couch potato' phenomenon underscores that meeting exercise targets does not fully compensate for 8–12 hours of daily sitting.
Social and economic determinants:
The epidemiology of obesity is undergoing an important inversion in India: what was once a disease of affluence (only the wealthy could afford excess calories) is increasingly a disease of the less affluent urban poor, who have access to cheap, energy-dense processed foods but not fresh produce, and whose working environments are sedentary. Food marketing disproportionately targets lower socioeconomic groups. Stress from financial insecurity, poor sleep from shift work, and lack of green spaces for physical activity all compound the risk.
Gut microbiome:
Emerging evidence demonstrates that the gut microbiome composition influences energy extraction from food and systemic inflammation. Germ-free mice colonised with gut microbiota from obese humans gain significantly more weight than those colonised from lean donors. Specific microbiome signatures (reduced Bacteroidetes, increased Firmicutes) are associated with greater caloric extraction from food, though causality in humans remains under investigation.
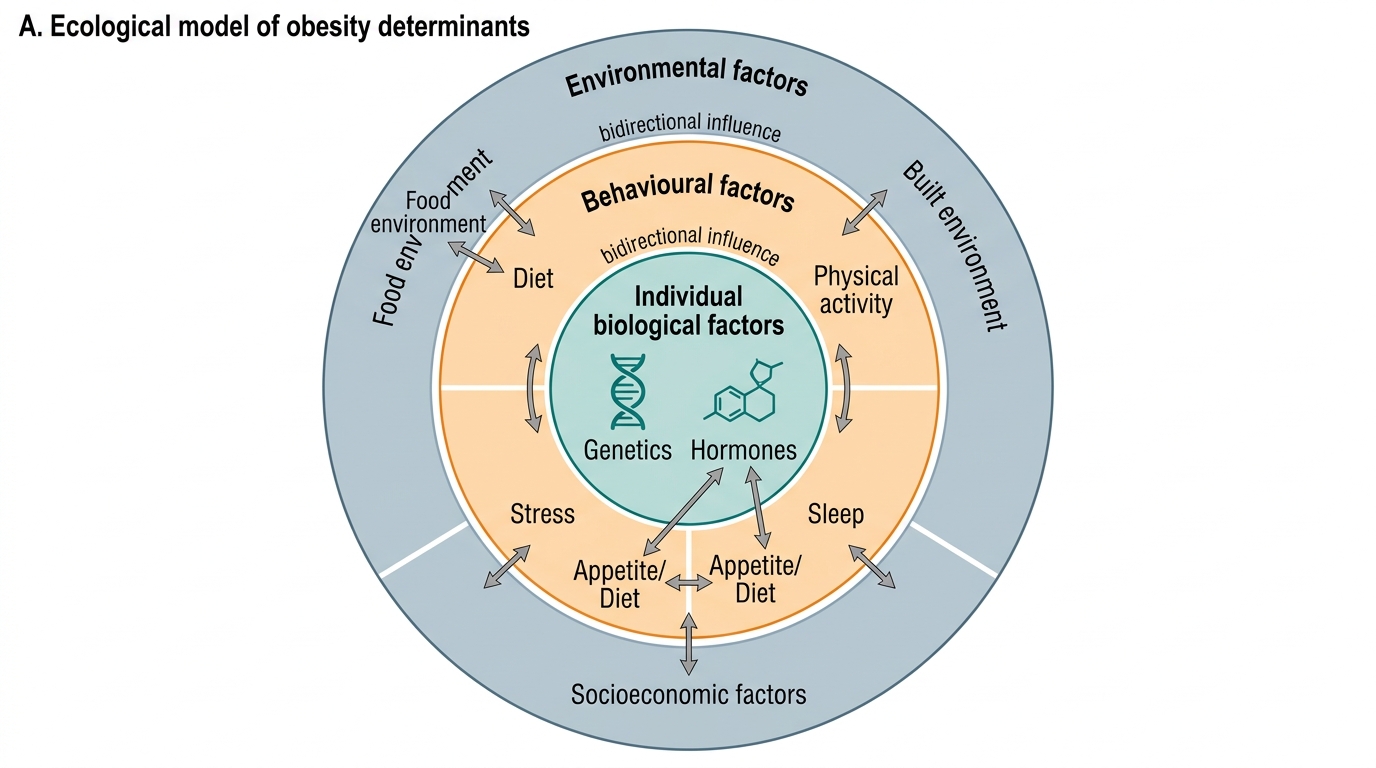
Ecological Determinants of Obesity
Diagnosis and Investigation of Obesity
The diagnosis of obesity is clinical and anthropometric — it does not require laboratory tests for confirmation. However, a structured investigative workup is essential for three distinct purposes: first, to screen for and exclude secondary causes before attributing obesity to lifestyle or genetics; second, to identify and quantify established obesity-related comorbidities (the complications that drive morbidity and mortality); and third, to risk-stratify the patient and guide the choice and intensity of treatment. The investigation of a new patient with obesity is therefore not a single test but a purposeful battery organised around these three goals, and approaching it systematically will prevent both over-investigation in low-risk patients and missed diagnoses in those harbouring a secondary or complicating condition.
Baseline anthropometry and clinical assessment:
Every patient should have BMI calculated (weight/height²) and classified using Asian-Indian cut-offs (overweight ≥23, obese ≥25 kg/m²), waist circumference measured at the midpoint between the lowest rib and the iliac crest (cut-offs: men ≥90 cm, women ≥80 cm), and blood pressure recorded. Body fat percentage by bioelectrical impedance analysis (BIA) can supplement BMI in patients where the BMI-to-fat relationship may be misleading (e.g., high-muscle athletes or sarcopenic elderly).
Screening for secondary causes:
| Test | Secondary Cause Excluded |
|---|---|
| Serum TSH | Primary hypothyroidism — mandatory in all new obesity presentations |
| 24-h urinary free cortisol or 1 mg overnight dexamethasone suppression test (DST) | Cushing syndrome — test if clinical features present (central obesity, striae, proximal myopathy, moon face) |
| Free testosterone, LH/FSH, pelvic ultrasound | PCOS in women with oligomenorrhea, hirsutism, acne |
| Fasting insulin, C-peptide with glucose | Insulinoma — if episodic hypoglycaemia with hyperphagia |
| IGF-1 | Adult growth hormone deficiency — if pituitary history |
| Pituitary MRI | Hypothalamic obesity — if headache, visual field defects, or pituitary history |
Screening for obesity-related comorbidities:
| Investigation | Comorbidity Detected |
|---|---|
| Fasting plasma glucose, HbA1c, 75 g OGTT | Pre-diabetes, type 2 diabetes mellitus |
| Fasting lipid profile (TG, LDL, HDL, total cholesterol) | Dyslipidaemia, metabolic syndrome |
| Liver function tests, ALT/AST ratio | NAFLD/NASH |
| Ultrasound abdomen | Hepatic steatosis, grade of fatty liver |
| ECG and echocardiography | Cardiac hypertrophy, diastolic dysfunction, arrhythmia |
| Polysomnography (sleep study) | Obstructive sleep apnoea — if snoring, witnessed apnoeas, daytime somnolence, morning headache |
| Uric acid | Hyperuricaemia, gout risk |
| Serum creatinine, eGFR | CKD — obesity-related glomerulopathy |
| DEXA scan | Bone density assessment in women with prolonged obesity and menstrual irregularity |
The depth of investigation is guided by clinical context. A 28-year-old otherwise healthy woman with BMI 27 and no symptoms warrants TSH, fasting glucose, and lipid profile. A 55-year-old man with BMI 35, snoring, and hypertension warrants a full metabolic panel plus polysomnography. Clinical acumen guides the sequence; the table above provides the menu, not a mandatory checklist.
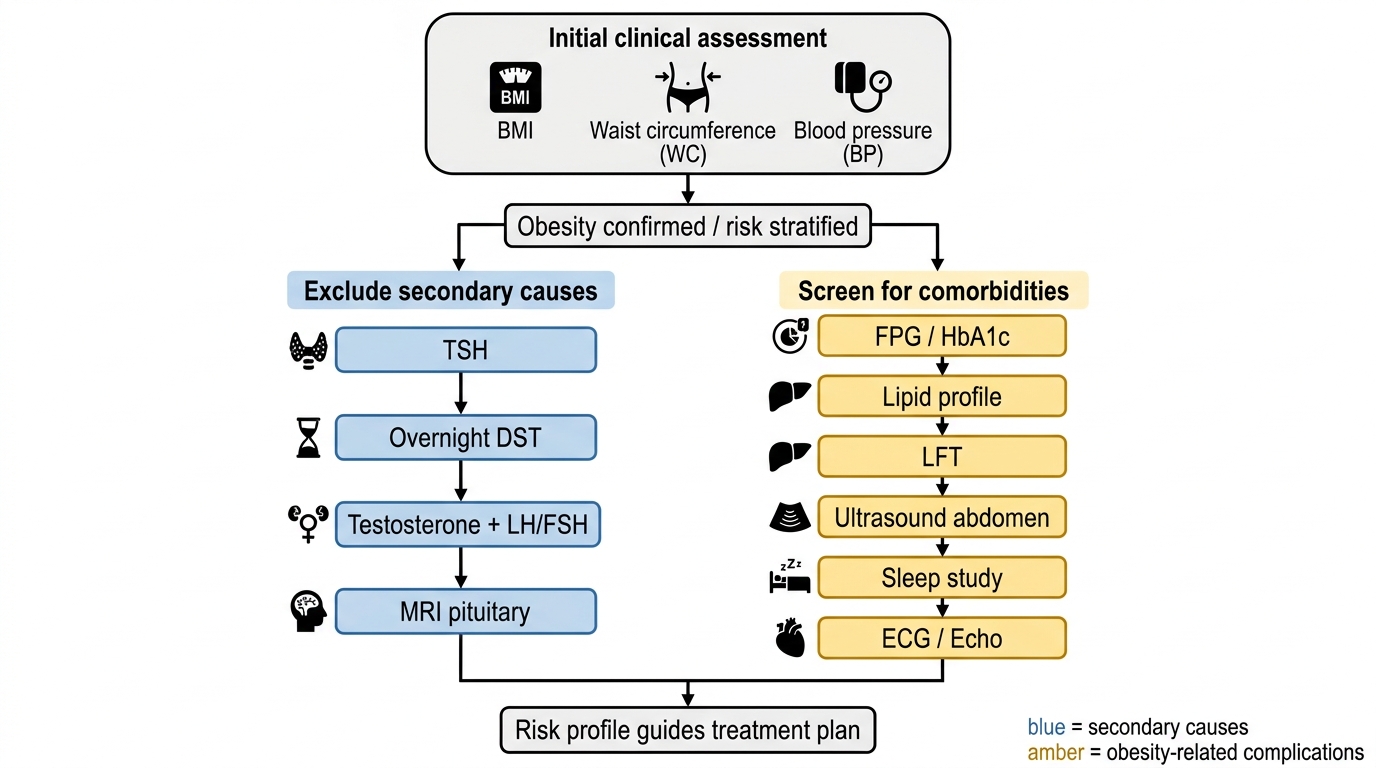
Investigation Algorithm for Obesity
Natural History of Obesity and Its Complications
The natural history of obesity follows a trajectory that begins with energy imbalance at the cellular and tissue level and, if left unaddressed, culminates in a spectrum of organ-level complications that are the principal cause of premature mortality and disability. Understanding the progression from adipose tissue dysfunction to systemic disease is fundamental to counselling patients on why intervention matters — and why intervening early is far more effective than treating established complications.
Provided image
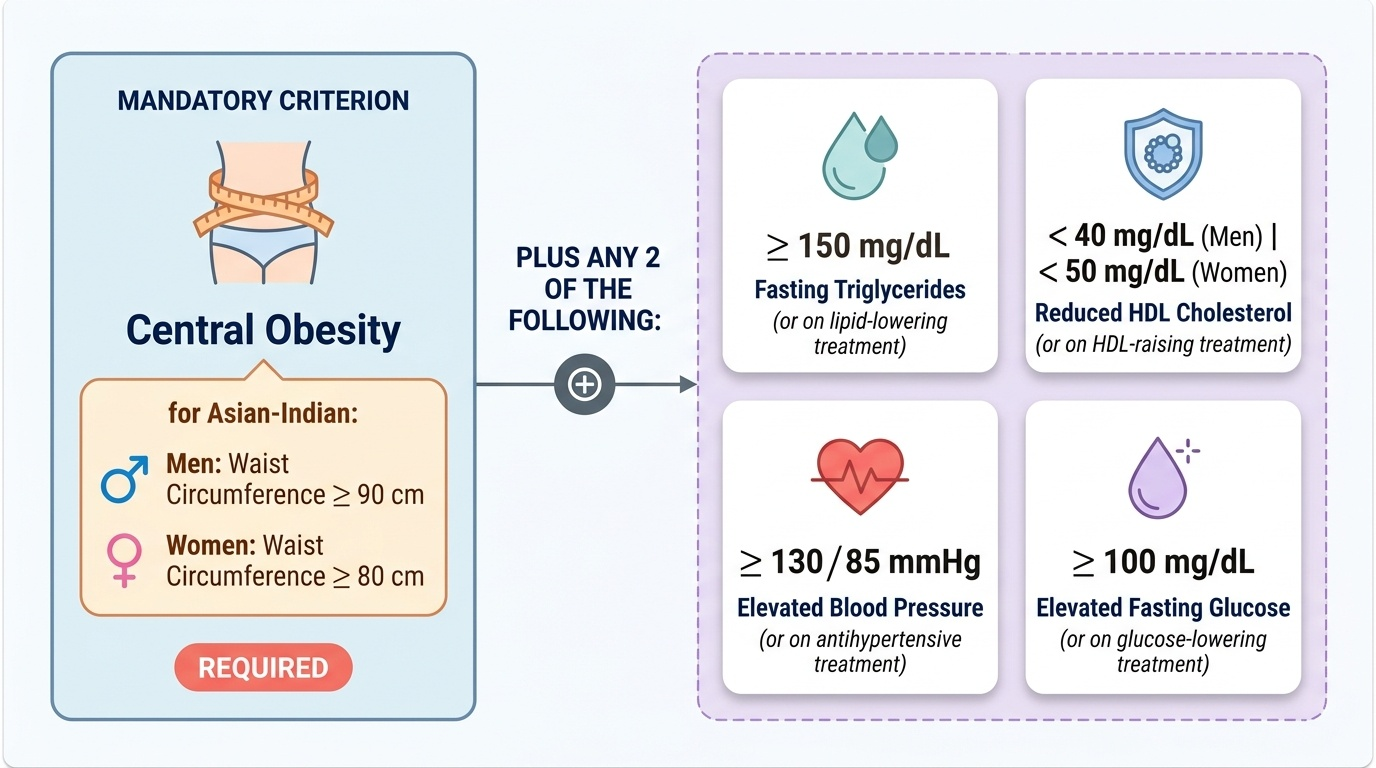
Metabolic Syndrome is a cluster of cardiometabolic risk factors that frequently co-occur in obese individuals and substantially amplify cardiovascular risk beyond any single component. The most widely used criteria are those of the International Diabetes Federation (IDF, 2005), which define metabolic syndrome as central obesity (mandatory: waist circumference ≥ 90 cm in Asian-Indian men, ≥ 80 cm in Asian-Indian women) PLUS any two of:
1. Fasting triglycerides ≥ 150 mg/dL (or on lipid-lowering treatment)
2. HDL cholesterol < 40 mg/dL in men or < 50 mg/dL in women (or on HDL-raising treatment)
3. Blood pressure ≥ 130/85 mmHg (or on antihypertensive treatment)
4. Fasting glucose ≥ 100 mg/dL (or on glucose-lowering treatment)
The alternative NCEP-ATP III criteria do not require central obesity as a prerequisite but specify any 3 of 5 components. The IDF criteria are increasingly preferred for South Asian populations because they embed the Asian-Indian waist circumference cut-offs and place central obesity at the centre of the diagnostic framework, aligning with the pathophysiology of visceral adiposity.
Complications of obesity are best understood as multi-organ manifestations of chronic metabolic inflammation, insulin resistance, and mechanical loading:
- Cardiovascular: Hypertension (increased cardiac output, sodium retention, sympathetic activation), coronary artery disease, heart failure, and atrial fibrillation are all significantly more prevalent. Obesity cardiomyopathy is a distinct entity characterised by increased left ventricular mass and diastolic dysfunction even in the absence of hypertension.
- Metabolic: Type 2 diabetes mellitus (central to the trajectory; visceral fat → hepatic insulin resistance → impaired glucose tolerance → frank diabetes); non-alcoholic fatty liver disease (NAFLD)/non-alcoholic steatohepatitis (NASH) — now increasingly termed metabolic-associated fatty liver disease (MAFLD) — which can progress to cirrhosis and hepatocellular carcinoma.
- Respiratory: Obstructive sleep apnoea (OSA) from pharyngeal fat deposition and loss of upper airway tone — associated with daytime somnolence, hypertension, arrhythmias, and cardiovascular events. Obesity hypoventilation syndrome (OHS, Pickwickian syndrome) — chronic hypoventilation, hypercapnia, polycythaemia, and pulmonary hypertension in severe obesity; can progress to right heart failure.
- Musculoskeletal: Knee and hip osteoarthritis accelerated by mechanical loading; gout risk elevated (uric acid increased by insulin resistance).
- Neoplastic: Obesity is causally associated with increased risk of colorectal cancer, postmenopausal breast cancer, endometrial cancer, oesophageal adenocarcinoma, pancreatic cancer, renal cell carcinoma, and hepatocellular carcinoma — through mechanisms including hyperinsulinaemia, elevated oestrogens (aromatase in adipose tissue), chronic inflammation, and altered adipokine signalling.
- Reproductive: PCOS in women; male hypogonadism and erectile dysfunction; reduced fertility in both sexes; obstetric complications (gestational diabetes, hypertension, caesarean delivery, neonatal macrosomia).
- Psychological: Depression, anxiety, poor body image, and social stigma — bidirectional with obesity (depression drives emotional eating; obesity drives depression).
The concept of progressive adiposopathy (Bays, 2011) frames these complications as consequences of dysfunctional adipose tissue — adipocytes that have outgrown their vascular supply become hypoxic, undergo necrosis, and trigger macrophage infiltration (producing the characteristic 'crown-like structures' on adipose tissue biopsy). This inflammatory milieu drives systemic insulin resistance and the multi-organ complications listed above.
SELF-CHECK
A 45-year-old man from Mumbai with BMI 26 kg/m² (by Asian-Indian criteria, this is frank obesity) has a waist circumference of 92 cm. His fasting triglycerides are 170 mg/dL, HDL is 38 mg/dL, BP is 138/88 mmHg, and fasting glucose is 108 mg/dL. How many components of metabolic syndrome does he have according to IDF 2005 criteria?
A. He has central obesity alone and does not yet meet IDF criteria for metabolic syndrome
B. He meets IDF criteria: central obesity plus 2 additional components
C. He meets IDF criteria: central obesity plus all 4 additional components
D. He cannot be assessed as metabolic syndrome without an OGTT result
Reveal Answer
Answer: C. He meets IDF criteria: central obesity plus all 4 additional components
IDF 2005 criteria for Asian-Indian men require: mandatory central obesity (waist ≥90 cm — he has 92 cm, so this criterion is met) PLUS any 2 of: TG ≥150 (he has 170 — YES), HDL <40 in men (he has 38 — YES), BP ≥130/85 (he has 138/88 — YES), fasting glucose ≥100 (he has 108 — YES). He actually meets ALL 4 additional components, not just 2 — meaning he has the full syndrome. An OGTT is not required for the IDF metabolic syndrome criteria, which use fasting glucose ≥100 mg/dL as the criterion.
SELF-CHECK
A 32-year-old woman has BMI 24.5 kg/m². Her colleague tells her this is 'normal weight' because it falls below 25. In the context of Asian-Indian cut-offs, which classification is correct?
A. Normal weight: BMI 23–24.9 is normal in Asian Indians
B. Overweight: BMI ≥23 is overweight by Asian-Indian cut-offs
C. Obese: BMI ≥23 is obese by Asian-Indian cut-offs
D. Classification requires waist circumference measurement before deciding
Reveal Answer
Answer: B. Overweight: BMI ≥23 is overweight by Asian-Indian cut-offs
According to the Asian-Indian BMI cut-offs endorsed by ICMR/WHO, overweight begins at BMI ≥23 kg/m² (NOT the Western ≥25). BMI 24.5 therefore falls in the overweight category (23.0–24.9 kg/m²) for Asian Indians. Obesity begins at ≥25 in this classification (vs ≥30 in Western WHO). The Western cut-offs are inappropriate for Indian patients and would miss a significant proportion of at-risk individuals. While waist circumference adds important information about visceral fat and cardiometabolic risk, it does not change the BMI classification.
CLINICAL PEARL
The single most important clinical lesson about obesity in India is to use the correct cut-offs. Asian-Indian BMI thresholds (overweight ≥23, obese ≥25 kg/m²) are not a minor technical detail — they represent a meaningful difference in cardiometabolic risk stratification. A patient with BMI 26 kg/m² who is reassured using Western charts may already have metabolic syndrome by IDF criteria. Always measure waist circumference alongside BMI — visceral fat is the metabolically active compartment, and a patient can be 'normal BMI' by Western standards yet have dangerous central adiposity (the 'normal weight obese' or 'thin-fat Indian' phenotype).
Second pearl: always screen for secondary causes before attributing obesity purely to lifestyle. Undiagnosed hypothyroidism or Cushing syndrome presenting as weight gain will not respond to diet and exercise counselling, and the missed diagnosis delays definitive treatment. A serum TSH is mandatory in all new presentations of obesity.