Page 4 of 19
IM15.{4-5,7-8} | GI Bleeding Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit and document a focused history in a patient with GI bleeding that identifies the route, quantity, grade, duration, aetiology, and risk factors
- Perform and document a targeted physical examination including volume status assessment, general examination, and abdominal examination
- Demonstrate correct technique for anal and rectal examination
- Generate and prioritise a differential diagnosis based on clinical features
INSTRUCTIONS
Clinical evaluation of GI bleeding is a skill that combines history-taking, systematic examination, and pattern recognition to localise the source, estimate severity, and construct a prioritised differential. This module teaches you to do this efficiently and accurately in a time-pressured clinical setting.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 47 — Gastrointestinal Bleeding (textbook)
- API Textbook of Medicine, 10th ed. — Gastrointestinal Haemorrhage (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed., Ch. 21 (textbook)
- British Society of Gastroenterology: UK guidelines on the management of upper gastrointestinal bleeding, 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients present to your medical ward on the same afternoon. The first is a 45-year-old man who reports 'passing some blood in his stool' — he mentions it almost as an aside at the end of a consultation for back pain. The second is a 62-year-old woman brought in by ambulance with one episode of fresh haematemesis, now feeling faint and dizzy when she tries to sit up. Both have 'GI bleeding' written on their referral slips. Yet the history alone — route of bleeding, its volume, the haemodynamic symptoms — tells you within 30 seconds that one patient needs reassurance and an outpatient colonoscopy referral, while the other needs two large-bore cannulae and an urgent endoscopy call tonight. The clinical evaluation skills in this module are not just academic requirements — they are the diagnostic tools that create this triage distinction in real time.
WHY THIS MATTERS
The structured clinical evaluation of GI bleeding — history, examination, and differential construction — is the gateway to every downstream decision: investigation ordering, risk stratification using validated scores, timing of endoscopy, and decisions about admission versus discharge. NMC competencies IM15.4, IM15.5, IM15.7, and IM15.8 target these skills at the SH (Skills with Supervision under Observation) level, meaning you are expected to demonstrate competent performance in the clinical encounter with appropriate guidance — not merely describe what should be done. The Glasgow-Blatchford Score, which stratifies patients for early discharge versus urgent intervention, is based entirely on clinical history and basic investigations that you can obtain at the bedside in under five minutes. Getting the clinical evaluation right literally determines whether a patient goes home or gets admitted to the ICU.
RECALL
Recall that GI bleeding is classified by anatomical origin: upper GI (proximal to the ligament of Treitz) versus lower GI (distal). The classic presentations are haematemesis and melaena for upper, and haematochezia for lower — though massive upper bleeding can present with haematochezia. Recall also the four phases of haemorrhagic shock: the compensated phase (tachycardia, preserved BP), the uncompensated phase (falling systolic, narrowed pulse pressure), decompensated shock, and irreversible shock. From your anatomy teaching, recall that the anus and rectum are examined with a digital rectal examination (DRE) — the index finger palpates the prostate or posterior vaginal wall, the rectal walls, the sphincter tone, and any mucosal abnormality. Any blood on the examining finger must be interpreted in the context of the full clinical picture.
Clinical Indication and Approach to GI Bleeding Evaluation
The clinical evaluation of a patient with suspected GI bleeding serves three simultaneous purposes: localisation (upper vs lower, and narrowing the aetiology within each), severity assessment (current haemodynamic state and estimated volume loss), and risk stratification (likelihood of rebleeding, need for intervention, mortality risk). These three purposes must be pursued in parallel rather than sequentially, because the approach to a haemodynamically compromised patient differs fundamentally from the calm, structured clerking of a stable outpatient with occult blood loss.
Provided image
The first clinical decision upon encountering a patient with GI bleeding is whether the evaluation needs to proceed immediately alongside resuscitation (haemodynamic instability, active haematemesis, altered mental state), or whether it can be conducted in the standard structured manner (patient alert, stable vitals, no active bleeding). The primary survey — assessing airway, breathing, and circulation before any detailed history — takes absolute precedence in the unstable patient. A patient who cannot maintain their airway due to ongoing haematemesis requires intubation before endoscopy or even a detailed history; a patient in frank hypotensive shock needs IV access and crystalloid infusion before the history beyond the minimum essentials (What happened? Any medications — anticoagulants, NSAIDs? Any liver disease?). Once the immediate survival threat is managed, the full structured evaluation proceeds.
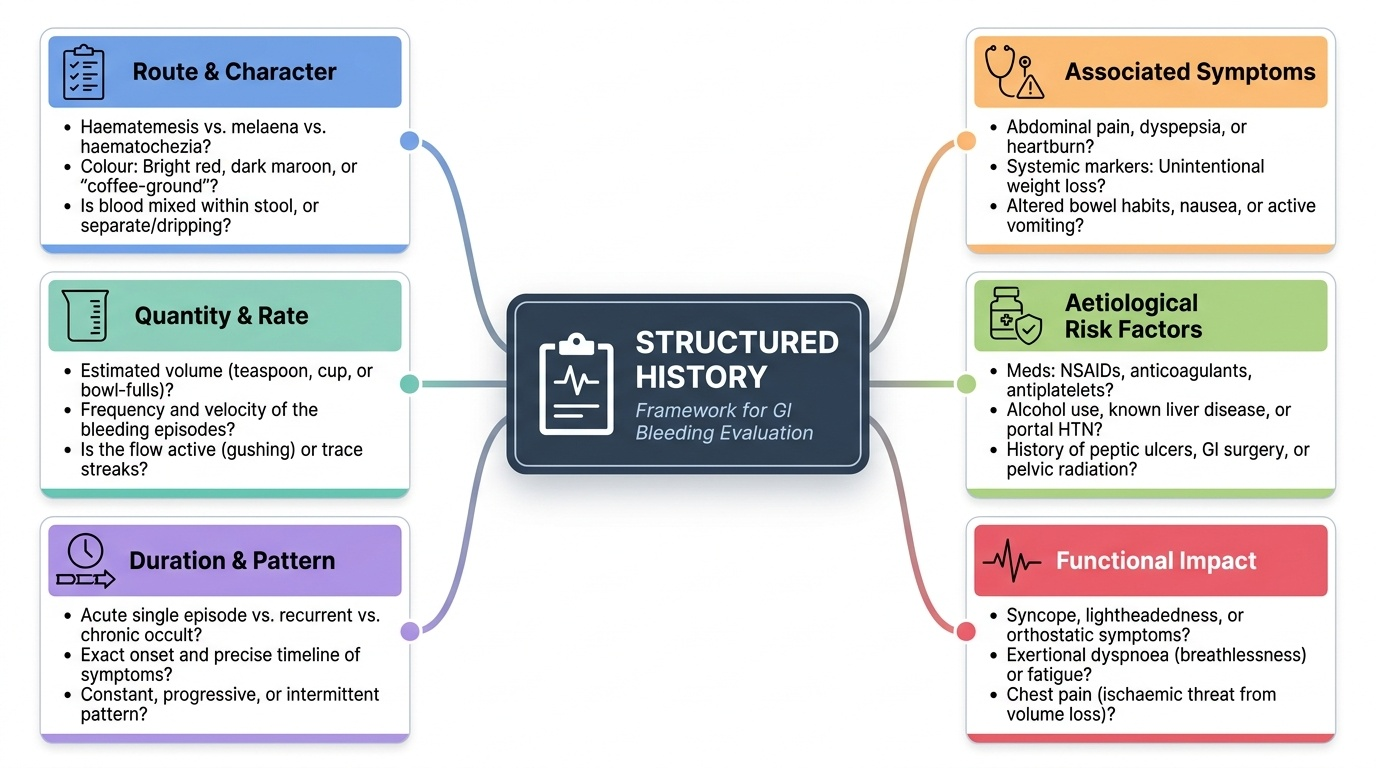
In the stable patient, however, the history and examination are not merely confirming what is already suspected — they are generating the differential diagnosis and directing the diagnostic workup. Approximately 70–80% of GI bleeding diagnoses can be correctly predicted from a well-taken clinical history alone. The structured history format for GI bleeding should cover six domains: route and character of the bleed, quantity and rate of blood loss, duration and pattern (acute single episode vs recurrent vs chronic occult), associated symptoms (pain, weight loss, altered bowel habit, vomiting), aetiological risk factors (medications, alcohol, liver disease, prior ulcers, prior abdominal surgery, radiation history), and functional impact (syncope, breathlessness, chest pain — markers of systemic volume loss and end-organ effect).
Governing Principles of GI Bleeding Clinical Evaluation
Effective clinical evaluation of GI bleeding is governed by a small number of organising principles that apply regardless of the specific cause or presentation. Understanding these principles — rather than memorising a symptom list — is what allows the clinician to adapt the evaluation framework to any patient, including the highly atypical or complex case. These governing principles are the bridge between the theoretical knowledge of GI bleeding aetiology and the practical competency of performing a focused, diagnostically efficient clinical encounter.
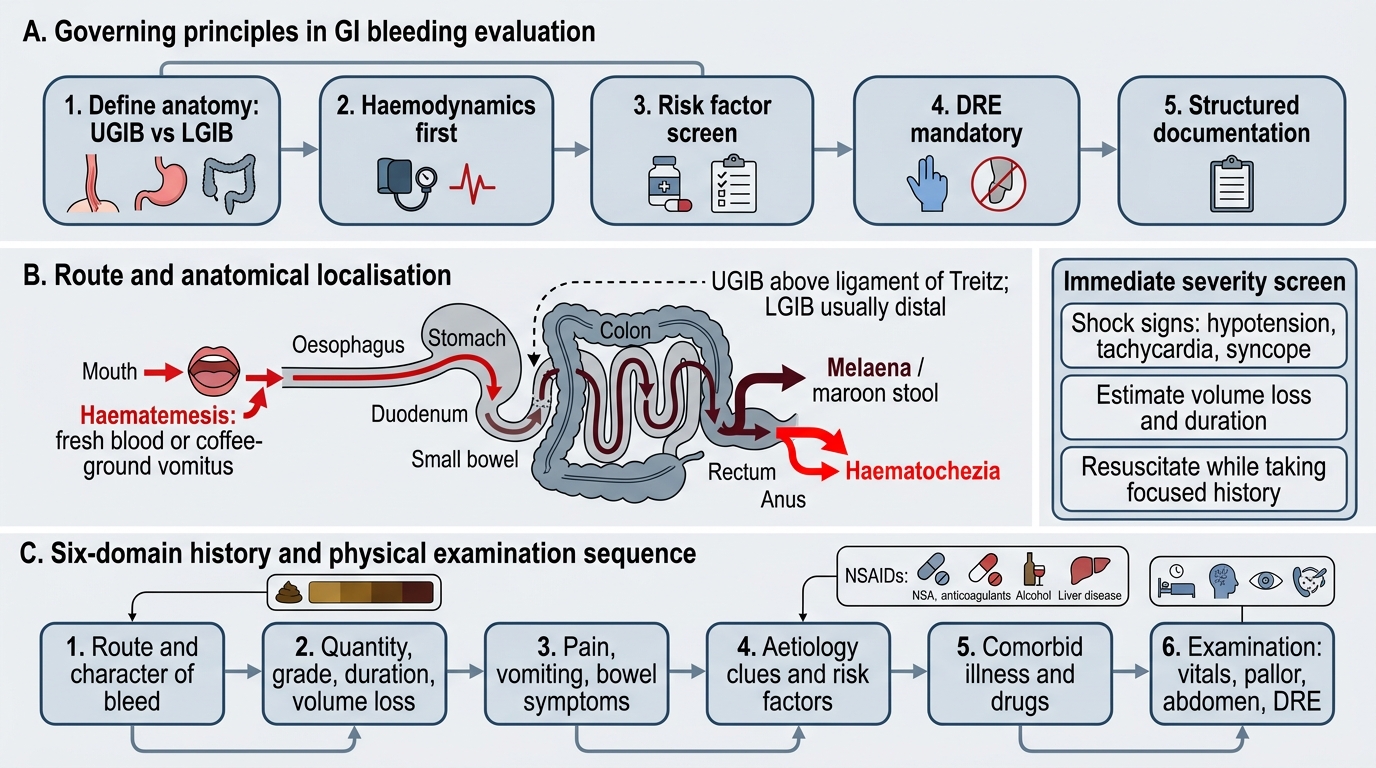
Principle 1 — Anatomy drives the evaluation structure. The division of the GI tract at the ligament of Treitz into upper and lower compartments is not merely anatomical trivia — it determines which symptoms, signs, and investigations are relevant for localisation. Every element of the history and examination should be consciously mapped to the question: does this finding support an upper or lower source? An elevated BUN:creatinine ratio, coffee-ground vomiting, or haemodynamic instability in the context of suspected diverticular disease should immediately trigger upper GI re-evaluation. The anatomical framework is the single most powerful organiser of the clinical evaluation.
Principle 2 — Haemodynamics before diagnosis. The clinical evaluation must always begin with the assessment of haemodynamic stability, because this governs the entire pace and priorities of the encounter. A haemodynamically compromised patient requires abbreviated targeted assessment (minimum history: what happened, any anticoagulants, any liver disease?) and immediate resuscitation simultaneously. A stable patient can be clerked fully and systematically. Conflating these two modes — performing a leisurely full history in a patient who is actively deteriorating — is one of the most dangerous errors in clinical medicine.
Principle 3 — Risk factors are aetiological keys. In GI bleeding, the clinical history is extraordinarily aetiologically informative because the major causes each have highly specific predisposing factors: NSAIDs and aspirin for peptic ulcer disease; chronic alcohol use and liver disease for variceal haemorrhage; age over 50 and prior diverticulosis for diverticular bleeding; prior pelvic radiation for radiation proctitis; prior aortic graft surgery for aortoenteric fistula. A systematic five-minute risk factor screen can narrow the differential from six diagnoses to one or two with high probability.
Principle 4 — The examination must be complete, including the rectum. No examination of a patient with lower GI bleeding or unexplained anaemia is complete without a digital rectal examination. Approximately 10% of colorectal carcinomas are palpable within 7–8 cm of the anal verge and will be missed by a physician who omits this examination. The DRE is neither invasive nor time-consuming when performed with proper technique, patient positioning, and explanation — it should be as routine as auscultating the chest.
Principle 5 — Documentation drives communication. NMC competency IM15.4 specifically requires that the history is not only elicited but documented and presented. A well-documented GI bleeding clerking note creates a shared record of findings, risk stratification scores, and differential priority for the endoscopy team, surgical team, and ICU — all of whom may manage this patient in sequence. Always document: the type, volume, and character of the bleed; the haemodynamic status at presentation; the risk factor screen; and the initial differential priority.
Clinical Evaluation Framework for GI Bleeding
History-Taking in GI Bleeding: Structured Approach
A focused history in GI bleeding proceeds through a structured sequence that extracts the maximum diagnostic information in the minimum time. Each domain of the history contributes specific aetiological probabilities and guides the differential prioritisation that follows. The following framework maps directly to NMC competency IM15.4's requirement to identify 'the route of bleeding, quantity, grade, volume loss, duration, etiology, comorbid illnesses and risk factors.'
1. Route and character of the bleed: Ask first whether the patient has vomited blood (haematemesis) or passed blood per rectum — and if both, establish which came first and which is the larger component. For haematemesis: Was the blood fresh bright red (current arterial haemorrhage) or like 'coffee grounds' (digested blood, slower bleeding or cessation)? Was it mixed with food or bile? How many episodes? Estimated volume per episode? For rectal bleeding: Was the blood bright red coating the stool, mixed with stool, in the toilet pan alone, or dark/maroon (melaena)? Was there blood mixed with mucus (IBD pattern) or associated with straining and perianal pain (haemorrhoids, fissure)? Has the patient noticed any black tarry stools (melaena)?
2. Quantity and haemodynamic symptoms: Quantifying blood loss from history alone is notoriously inaccurate, but haemodynamic symptoms provide reliable proxy indicators of significant volume loss. Ask directly: 'Did you feel faint or dizzy, especially when you stood up?' (postural presyncope = significant volume depletion — >1 litre blood loss in most adults). Did the patient actually lose consciousness? Is there palpitation (sympathetically driven tachycardia)? Breathlessness on minimal exertion (anaemia + low cardiac output)? Chest pain (myocardial ischaemia triggered by anaemia in a patient with underlying coronary disease)?
3. Duration and pattern: A first episode of acute haematemesis has a very different differential than recurrent episodes over years. Recurrent bright-red per-rectal bleeding in a young person points to haemorrhoids or a polyp; recurrent melaena in an elderly patient on NSAIDs points to PUD. Chronic gradual blood loss causing iron-deficiency anaemia (fatigue, dyspnoea) without overt haemorrhage points to occult bleeding from a colonic polyp, carcinoma, or angiodysplasia.
4. Associated symptoms: Pain is a highly discriminating feature: epigastric pain worse with hunger relieved by eating or antacids (duodenal ulcer); gnawing epigastric or left upper quadrant pain exacerbated by meals (gastric ulcer); sudden severe tearing back pain (consider aortic dissection or aortoenteric fistula — rare but must not be missed); crampy lower abdominal pain with bloody diarrhoea (IBD, infective colitis, ischaemic colitis — distinguishes from painless diverticular haemorrhage). Weight loss and change in bowel habit (alternating constipation and diarrhoea, pencil-thin stools, tenesmus) raise suspicion for colorectal carcinoma.
5. Aetiological risk factors: This is the domain with the highest aetiological yield. Ask systematically about: (a) NSAIDs, aspirin, and anticoagulants — the most modifiable risk factor for peptic ulcer bleeding; verify dose, duration, and whether taken with food or a gastroprotectant; (b) alcohol use — quantity, duration, type; chronic heavy alcohol use in a patient with haematemesis raises variceal probability and alters management fundamentally; (c) known peptic ulcer disease — prior diagnosis, prior H. pylori testing/treatment, prior bleed; (d) liver disease — jaundice, ascites, prior hepatitis, prior variceal banding; (e) previous abdominal or vascular surgery — aortic graft surgery (aortoenteric fistula), bowel resection, bariatric surgery (marginal ulcer), gastric surgery (stomal ulcer); (f) radiation therapy to the pelvis or abdomen (radiation proctitis or enteritis — presents as bloody diarrhoea months to years after radiation); (g) family history of colorectal cancer, polyps, or IBD.
6. Comorbidities: Cardiovascular disease, renal failure, diabetes, and haematological disorders all affect both the severity of clinical deterioration and the decisions about transfusion and intervention. A patient with a recent acute coronary syndrome has a higher anaemia intolerance threshold and may require a more liberal transfusion approach.
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
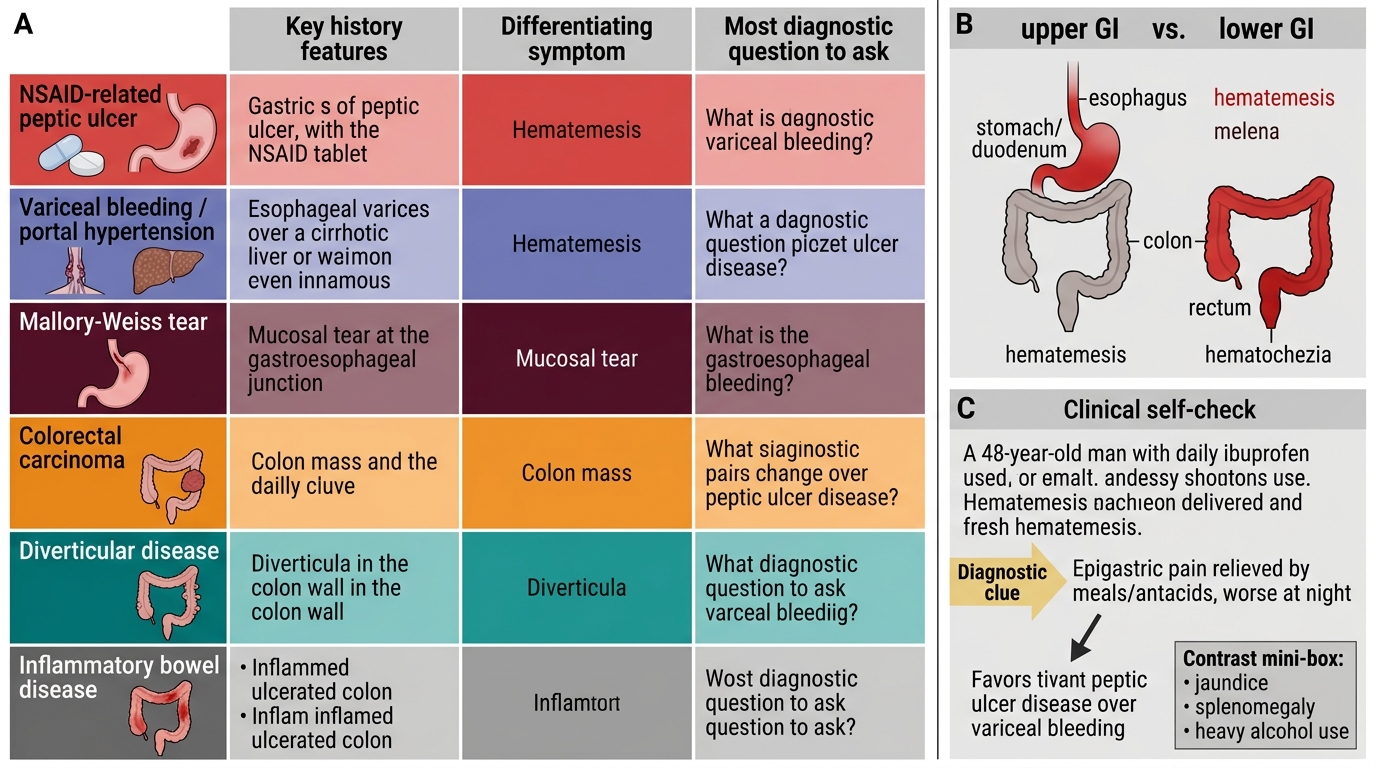
Clinical History Matrix for Gastrointestinal Bleeding
SELF-CHECK
A 48-year-old man with a two-week history of daily ibuprofen use for back pain presents with fresh haematemesis. Which additional history finding would MOST increase your suspicion for peptic ulcer disease over variceal bleeding?
A. History of jaundice six months ago
B. Epigastric pain relieved by meals and antacids, worse at night
C. Known splenomegaly on a previous ultrasound
D. Heavy alcohol use for 15 years
Reveal Answer
Answer: B. Epigastric pain relieved by meals and antacids, worse at night
Classic duodenal ulcer pain is epigastric, worse when the stomach is empty (classically 2–3 hours after meals and waking the patient at night), and partially relieved by food or antacids — this is the 'hunger pain food relief' pattern. Combined with active NSAID use (a direct mucosal cause of peptic ulceration), this strongly suggests PUD. Jaundice, splenomegaly, and chronic alcohol use all point towards chronic liver disease and portal hypertension, making variceal bleeding more likely in that context. The NSAID history alone raises PUD probability, but the typical pain pattern clinches it.