Page 5 of 19
IM15.{4-5,7-8} | GI Bleeding Clinical Evaluation — SDL Guide (Part 2)
Physical Examination: Volume Assessment and Abdominal Examination
The physical examination of a patient with GI bleeding has a dual purpose: quantifying the severity of volume loss (the safety assessment) and identifying signs pointing toward a specific aetiology (the diagnostic examination). These must be performed simultaneously and systematically, and the findings documented in a structured format. The examination follows the standard sequence: general appearance, vital signs, postural blood pressure, specific system examination — but GI bleeding imposes a hierarchy within this sequence: the volume assessment must come first because an unstable patient cannot cooperate with or tolerate a detailed examination until at least initial resuscitation has begun.
General appearance and vital signs: The immediate impression tells you a great deal — a pallid, diaphoretic, restless patient who is difficult to rouse suggests haemodynamic compromise. Record: heart rate, blood pressure (lying and sitting if the patient can cooperate — a drop in systolic BP of ≥20 mmHg or rise in pulse of ≥20 bpm on sitting indicates significant postural hypotension, consistent with ≥1 litre of volume deficit), respiratory rate, oxygen saturation, and capillary refill time. Capillary refill >3 seconds at the fingertip indicates peripheral vasoconstriction and poor perfusion. A postural blood pressure drop is one of the most sensitive clinical signs of volume depletion and should never be omitted in a patient with GI bleeding who can safely stand.
Stigmata of chronic liver disease: These findings, if present, raise the probability of variceal bleeding and immediately alter management (vasoactive drugs and antibiotic prophylaxis become mandatory). Examine systematically for: spider naevi (spider angiomas — >5 are significant; located in the distribution of the superior vena cava, i.e. above the nipple line), palmar erythema, Dupuytren's contracture (associated with alcohol-related disease), leukonychia (white nails — hypoalbuminaemia), clubbing (less specific), parotid enlargement (chronic alcohol use), gynaecomastia, jaundice (scleral icterus), bruising (coagulopathy), and abdominal findings: hepatomegaly (early cirrhosis) or shrunken nodular liver (advanced cirrhosis), splenomegaly (portal hypertension), ascites (shifting dullness, fluid thrill in tense ascites), caput medusae (dilated periumbilical veins — rarely seen in advanced portal hypertension), and peripheral oedema (hypoalbuminaemia).
Abdominal examination: Inspect for distension (ascites, obstruction), prior surgical scars (previous gastrointestinal surgery, prior aortic graft), and stomas. Auscultate for bowel sounds — hyperactive bowel sounds may be heard in UGIB because blood acts as an osmotic cathartic, accelerating intestinal motility. Palpate for tenderness (epigastric = PUD/gastritis; right iliac fossa tenderness with rebound may suggest Crohn's disease or right-sided colonic pathology; a palpable hepatic or splenic mass; a firm right iliac fossa mass = possible caecal carcinoma). Percuss for dullness in the flanks (ascites). In any patient with a history of aortic surgery or an aortic abdominal aneurysm who presents with GI bleeding, a pulsatile abdominal mass must be specifically sought — its presence with GI bleeding should raise the alarm for aortoenteric fistula.
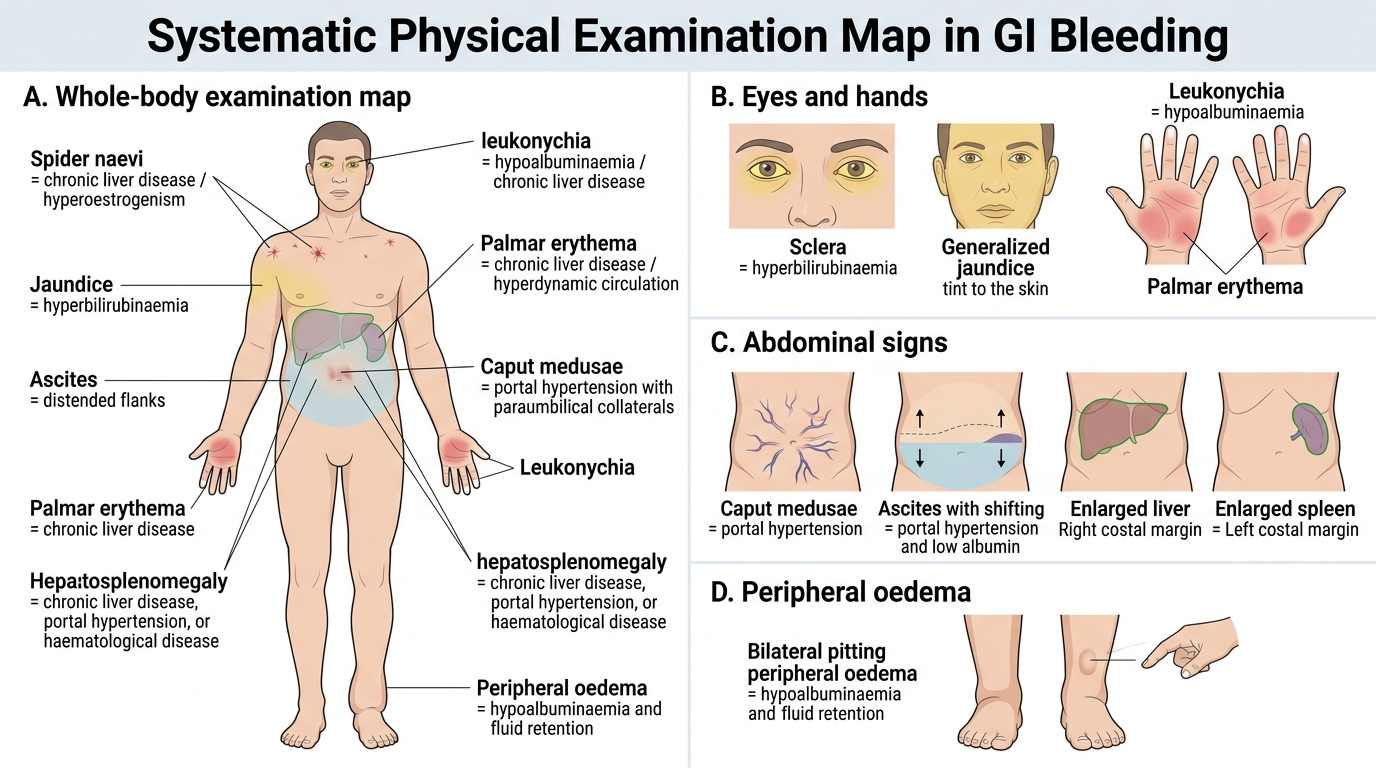
Physical Examination Map for GI Bleeding
Anal and Rectal Examination
The digital rectal examination (DRE) is an indispensable component of GI bleeding evaluation and is required by NMC competency IM15.7 to be performed competently. Yet it remains one of the most consistently omitted clinical skills in practice, often because it is uncomfortable for both patient and examiner, or because the physician believes the result will not change management. This belief is incorrect — the DRE can identify haemorrhoids, a rectal carcinoma within 7–8 cm of the anal verge, melaena on the examining finger confirming an upper source, or fresh blood suggesting an active lower bleed. It is non-negotiable in any patient with suspected lower GI bleeding or unexplained iron-deficiency anaemia.
Patient positioning: The left lateral (Sims') position is standard for medical DRE in India and the UK — patient lies on the left side with knees drawn up toward the chest (the hips and knees at approximately 90 degrees). Alternatively, the supine (modified lithotomy) or knee-elbow position may be used. Ensure adequate lighting, patient privacy, and a chaperone in all cases. Explain the procedure clearly to the patient, obtain verbal consent, and maintain dignity throughout.
Inspection: Before inserting the finger, inspect the perianal area carefully. Look for: external haemorrhoids (soft vascular cushions prolapsed at the anus, typically from 3, 7, and 11 o'clock positions); skin tags (fibroepithelial tags, remnants of thrombosed external haemorrhoids); anal fissure (a linear tear in the anoderm, typically at the 6 o'clock or 12 o'clock position posteriorly or anteriorly — fresh bright-red blood on the paper and severe perianal pain on defecation); fistula-in-ano openings (external openings of anal fistulae); condylomata; rectal prolapse; and skin changes of inflammatory bowel disease (perianal Crohn's disease — skin tags, multiple fistula openings, oedematous skin folds).
Digital palpation: Apply a lubricant generously on the examining finger (gloved) and over the anal verge. Ask the patient to take a deep breath and relax, then gently insert the index finger into the anal canal, first pointing posteriorly toward the coccyx to follow the natural axis of the anal canal, then rotating forward once past the sphincter. Assess: (a) Sphincter tone — normal, reduced (autonomic neuropathy, rectal prolapse, prior surgery), or increased (fissure, anxiety); (b) Anterior structures — in males, the prostate (size, consistency, presence of nodules or induration suggesting carcinoma, median sulcus); in females, the posterior vaginal wall and cervix; (c) Lateral and posterior walls — palpate systematically for mucosal irregularity, induration, or masses (tumour may be felt as a firm irregular mass within 7–8 cm of the anal verge); (d) Any stool in the rectum — assess its character: if faeces is present, is it blood-stained? On withdrawal, inspect the glove: note any blood (fresh red vs dark/melaena), mucus, or faeces. A melaena-stained glove confirms an upper or proximal source; fresh blood suggests a distal cause.
Common findings and their significance: A nodular firm mass in the rectal wall warrants urgent colonoscopy or sigmoidoscopy for formal biopsy (rectal carcinoma until proved otherwise). Soft reducible vascular masses at the classical positions with fresh blood but otherwise normal examination suggest haemorrhoids. Tenderness in the right iliac fossa appreciated on DRE suggests right-sided colonic pathology. A Blumer's shelf — a hard shelf-like palpable mass in the pouch of Douglas anteriorly felt on DRE — suggests peritoneal carcinomatosis from a gastric or ovarian primary.
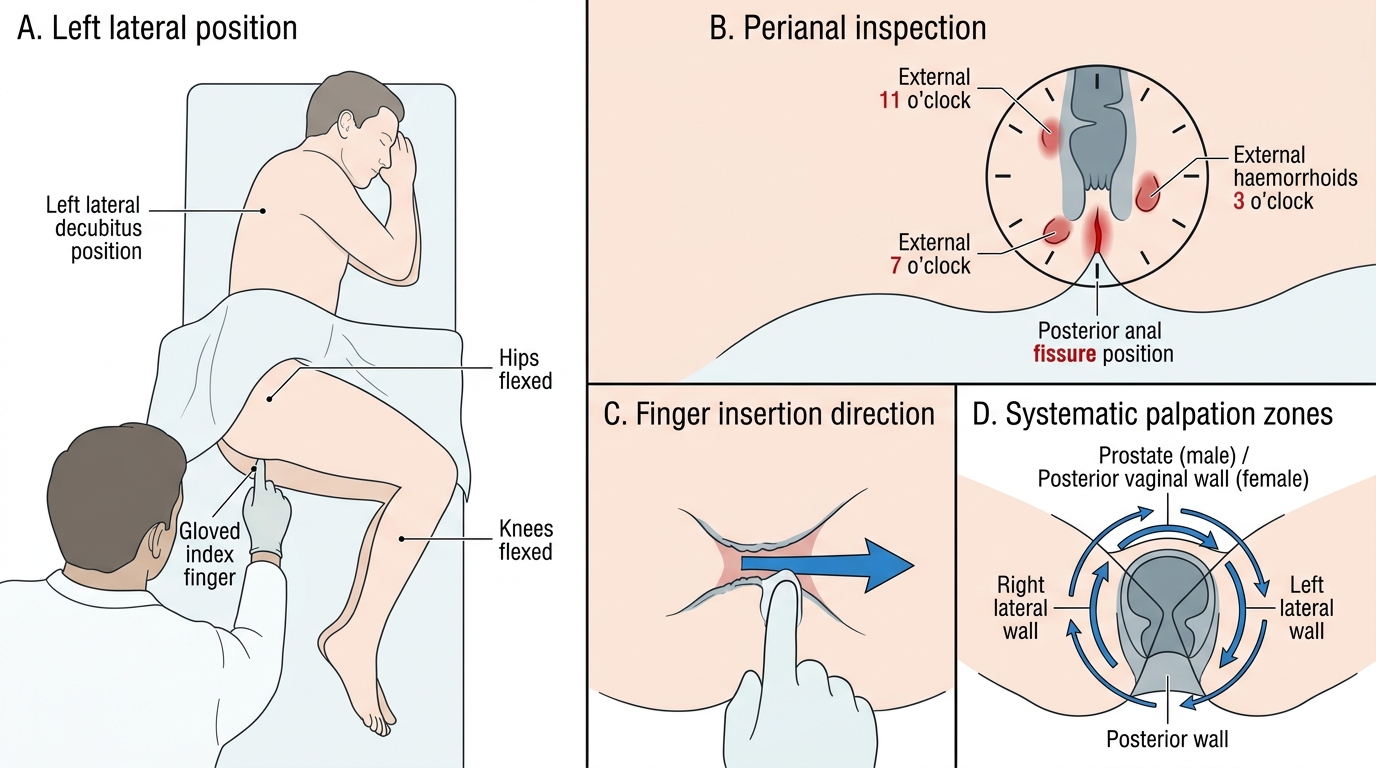
Step-by-Step Digital Rectal Examination Technique
SELF-CHECK
On performing a digital rectal examination in a 70-year-old man with haematochezia, you palpate a firm, irregular 3 cm mass on the right posterior rectal wall. Your glove shows fresh red blood. What is the MOST important next step?
A. Proceed directly to surgical resection — the mass is clearly malignant
B. Refer for urgent lower GI endoscopy (flexible sigmoidoscopy or colonoscopy) for direct visualisation and biopsy
C. Order a CT chest-abdomen-pelvis as the primary investigation
D. Prescribe haemorrhoid creams and arrange an outpatient appointment in 3 months
Reveal Answer
Answer: B. Refer for urgent lower GI endoscopy (flexible sigmoidoscopy or colonoscopy) for direct visualisation and biopsy
A firm irregular rectal mass on DRE is carcinoma until proved otherwise and requires formal endoscopic assessment with direct visualisation, biopsy for tissue diagnosis, and staging. Flexible sigmoidoscopy or colonoscopy is the investigation of choice. CT can be done for staging once tissue diagnosis is confirmed, but endoscopy with biopsy must come first. Surgical resection without tissue diagnosis and staging would be inappropriate. Haemorrhoid treatment would dangerously delay diagnosis of a malignancy.
Differential Diagnosis Generation and Prioritisation
After completing the history and examination, the clinical task shifts to constructing and prioritising the differential diagnosis. Effective differential construction in GI bleeding follows a two-step framework: first, generate the complete differential for the anatomical compartment most likely based on the clinical features (upper vs lower), then rank the diagnoses by probability and urgency. Probability is assessed from the clinical pattern (history features, examination findings, demographic risk factors); urgency is assessed from the haemodynamic status and the risk of rapid deterioration from each diagnosis. The most dangerous diagnosis that fits the clinical picture must always be prominently considered, even if it is less common — this is the 'must-not-miss' principle.
For an upper GI bleed presentation (haematemesis ± melaena): Construct the differential starting with the three most common causes — peptic ulcer disease (NSAID/H. pylori, 30–50%), variceal bleeding (portal hypertension from liver disease, 20–30% in India), and Mallory–Weiss tear (post-retching, typically self-limiting). Assign higher probability to peptic ulcer if there is NSAID use and epigastric ulcer-type pain; assign higher probability to varices if there are stigmata of chronic liver disease, known hepatitis, or heavy alcohol use. Then consider the less common but important causes: erosive gastritis (stress ulceration, NSAID-induced), Dieulafoy lesion (no warning, sudden massive haematemesis without prior symptoms), GAVE (gastric antral vascular ectasia — associated with cirrhosis and connective tissue disease), and aortoenteric fistula (must-not-miss in any patient with prior aortic graft surgery). The Glasgow-Blatchford Score numerically operationalises this clinical risk assessment for UGIB by incorporating BUN, haemoglobin, systolic BP, pulse, melaena, syncope, hepatic disease, and cardiac failure — a score of 0–1 identifies patients suitable for outpatient management, while a score ≥6 indicates high risk for clinical intervention.
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
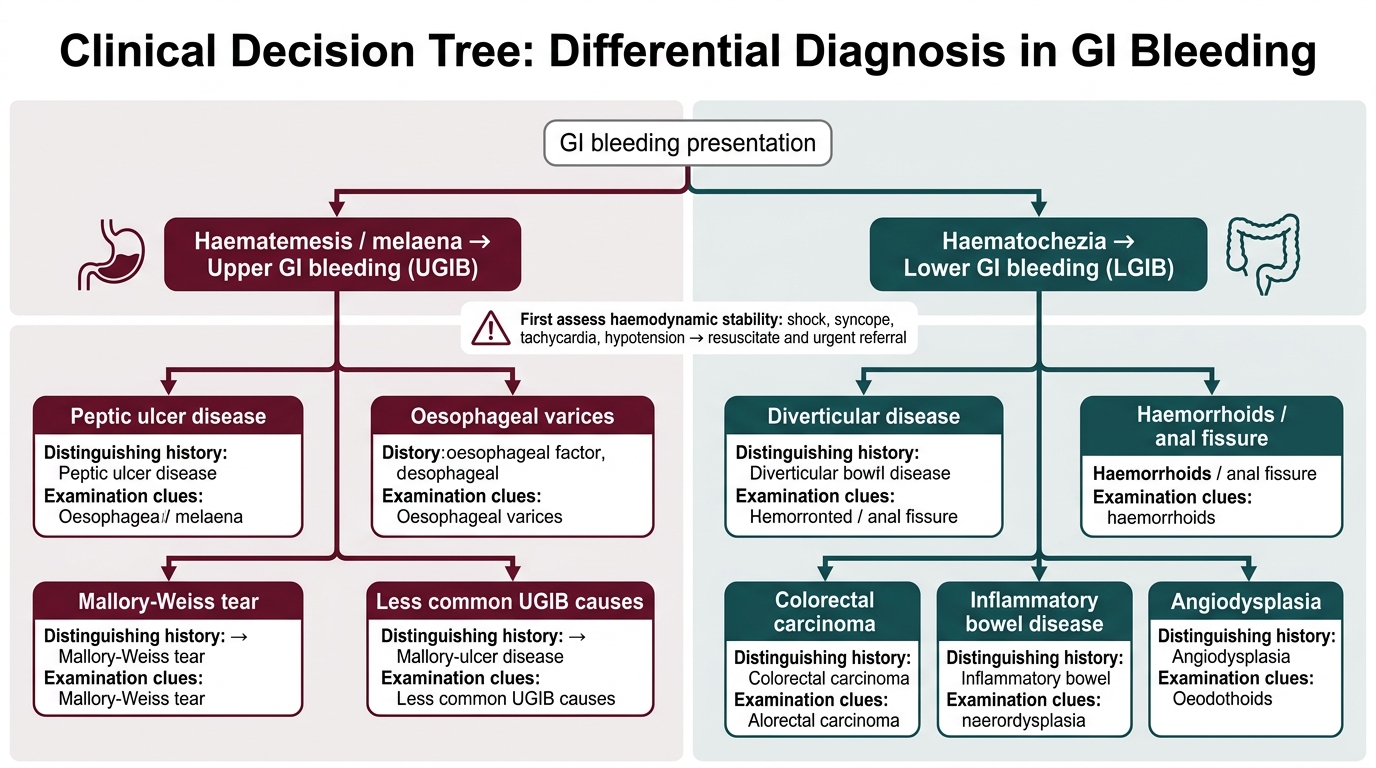
Differential Diagnosis of GI Bleeding
For a lower GI bleed presentation (haematochezia without haematemesis): The differential is stratified by age, chronicity, and associated features. In patients over 50 with acute painless large-volume haematochezia: diverticular disease leads the differential (sudden, copious, painless, ceases spontaneously), followed by angiodysplasia (recurrent, painless, in elderly patients often with chronic renal failure or aortic stenosis). In patients with chronic or intermittent rectal bleeding with change in bowel habit, weight loss, or tenesmus: colorectal carcinoma is the must-not-miss diagnosis, particularly if over 40 or with family history. In younger patients with bloody diarrhoea, mucus, and systemic symptoms (fever, joint pain): IBD (ulcerative colitis, Crohn's) is the leading diagnosis. Anorectal causes (haemorrhoids, anal fissure) are the most prevalent cause of rectal bleeding overall but are diagnoses of exclusion in the older patient — never assume haemorrhoids are responsible without excluding proximal pathology.
Prioritisation principles: (1) Any haemodynamically unstable patient's differential must place the highest-probability rapidly fatal diagnosis first — variceal haemorrhage in a cirrhotic, arterial peptic ulcer bleed in an NSAID user. (2) A first presentation of rectal bleeding in an adult over 45 must always include colorectal carcinoma in the differential regardless of how classic the haemorrhoid story sounds — a colonoscopy is mandatory unless an alternative definitive cause is established. (3) The must-not-miss diagnoses — aortoenteric fistula, ruptured viscus with haemorrhage — require specific contextual history questions (prior aortic surgery, prior peptic ulcer, anticoagulant use) without which they will be systematically missed.
SELF-CHECK
A 38-year-old woman presents with a 4-week history of bloody diarrhoea with mucus, crampy lower abdominal pain, fever, and 4 kg weight loss. She has had similar but milder episodes twice before over the past 2 years. Her physical examination shows mild left iliac fossa tenderness. Which diagnosis should lead the differential?
A. Diverticular disease
B. Colorectal carcinoma
C. Inflammatory bowel disease (ulcerative colitis or Crohn's disease)
D. Internal haemorrhoids
Reveal Answer
Answer: C. Inflammatory bowel disease (ulcerative colitis or Crohn's disease)
Bloody diarrhoea with mucus, crampy abdominal pain, fever, and weight loss in a young patient with episodic recurrence over 2 years strongly suggests inflammatory bowel disease (IBD) — specifically ulcerative colitis (left-sided colitis, mucus and blood mixed with diarrhoea) or Crohn's disease (any segment, may include extraintestinal manifestations). Diverticular disease in a 38-year-old would be unusual and typically presents with a single episode of painless large-volume bleeding, not recurrent bloody diarrhoea with mucus. Colorectal carcinoma is less common at 38 without family history and usually presents with progressive change in bowel habit rather than episodic flares. Haemorrhoids do not cause fever or systemic symptoms.
CLINICAL PEARL
The postural blood pressure measurement is the single most informative clinical sign you can elicit at the bedside in GI bleeding, yet it is systematically omitted in busy emergency settings. A drop in systolic BP of ≥20 mmHg on standing (or sitting in a patient too unwell to stand), combined with a rise in pulse of ≥20 bpm, indicates significant intravascular volume depletion — typically ≥1 litre in an adult. This finding, in a patient who 'looks stable' lying down, should immediately escalate your management response. The absence of a postural drop does NOT guarantee adequate volume status — it merely indicates early or compensated haemorrhage. Always measure postural BP before declaring a GI bleed patient 'stable.'