Page 6 of 19
IM15.{4-5,7-8} | GI Bleeding Clinical Evaluation — SDL Guide (Part 3)
Applied Practice: Clinical Evaluation Case Scenarios
The clinical evaluation skills developed in this module — structured history, systematic volume assessment and abdominal examination, DRE technique, and differential prioritisation — are best consolidated through their application to case-based scenarios that replicate the real clinical encounter. Each of the following cases requires you to apply the governing principles and structured techniques covered in the preceding sections: identify the haemodynamic priority, conduct the structured history mentally, interpret the examination findings, and generate a prioritised differential before reading the analysis. The goal is to develop the pattern-recognition speed and clinical confidence that comes from repeated application of a consistent evaluation framework under realistic clinical conditions. After working through each case, calculate the approximate Glasgow-Blatchford Score from the data provided and determine the appropriate management disposition.
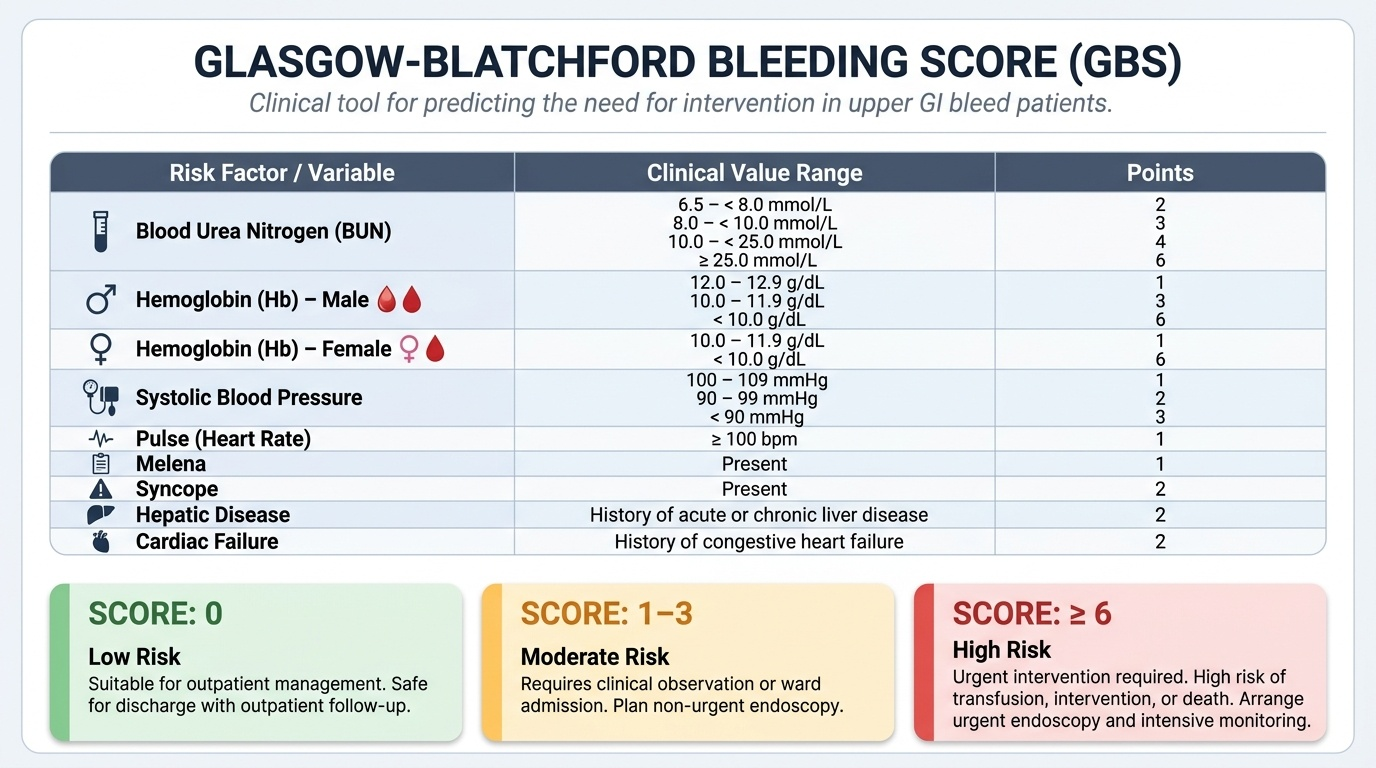
Provided image
Scenario A: A 52-year-old man presents with two episodes of haematemesis (each approximately 200 mL fresh blood) over 3 hours. He reports heavy alcohol use for 20 years, recent jaundice 2 months ago, and increasing abdominal distension. On examination: HR 108, BP 95/65 mmHg lying (drops to 80/50 sitting); abdomen is distended with shifting dullness; you note spider naevi on the chest and bilateral palmar erythema; spleen is palpable 4 cm below the costal margin.
Assessment: The dominant differential diagnosis is variceal haemorrhage — chronic alcohol-related liver disease with signs of portal hypertension (ascites, splenomegaly, spider naevi, palmar erythema), active haematemesis, and significant haemodynamic compromise (postural BP drop 15 mmHg, tachycardia, hypotension). Secondary differentials include Mallory–Weiss tear (common in alcoholic patients who vomit) and GAVE. PUD from NSAIDs is less likely without that history. Documented differential priority: (1) variceal haemorrhage — manage with vasoactive drug (terlipressin or octreotide), IV antibiotics (ceftriaxone), and urgent endoscopic band ligation; (2) Mallory–Weiss tear — usually self-limiting but may require endoscopic treatment if significant; (3) PUD/erosive gastritis — IV PPI may be added but is not the primary intervention.
Scenario B: A 35-year-old woman presents with a 6-month history of intermittent bright-red blood on the toilet paper after defecation, associated with constipation and straining. No haematochezia, no melaena, no weight loss, no change in bowel habit. On DRE: sphincter tone normal, no mass palpable, fresh blood on the glove. On perianal inspection: grade 2 haemorrhoids visible at 3, 7, and 11 o'clock.
Assessment: Clinical picture is consistent with symptomatic haemorrhoids — young woman, bright-red blood on paper after straining, no systemic symptoms, no palpable mass, haemorrhoids visible and confirmed on DRE. However, at age 35 with an otherwise classic presentation, a trial of conservative management (dietary fibre, hydration, stool softeners, topical cream) is reasonable — but if symptoms persist beyond 6–8 weeks or if there is any atypical feature (change in bowel habit, weight loss, mucus, tenesmus, family history of CRC), lower GI endoscopy (flexible sigmoidoscopy or colonoscopy) should be arranged.
Self-Assessment: Consolidating Clinical Evaluation Competencies
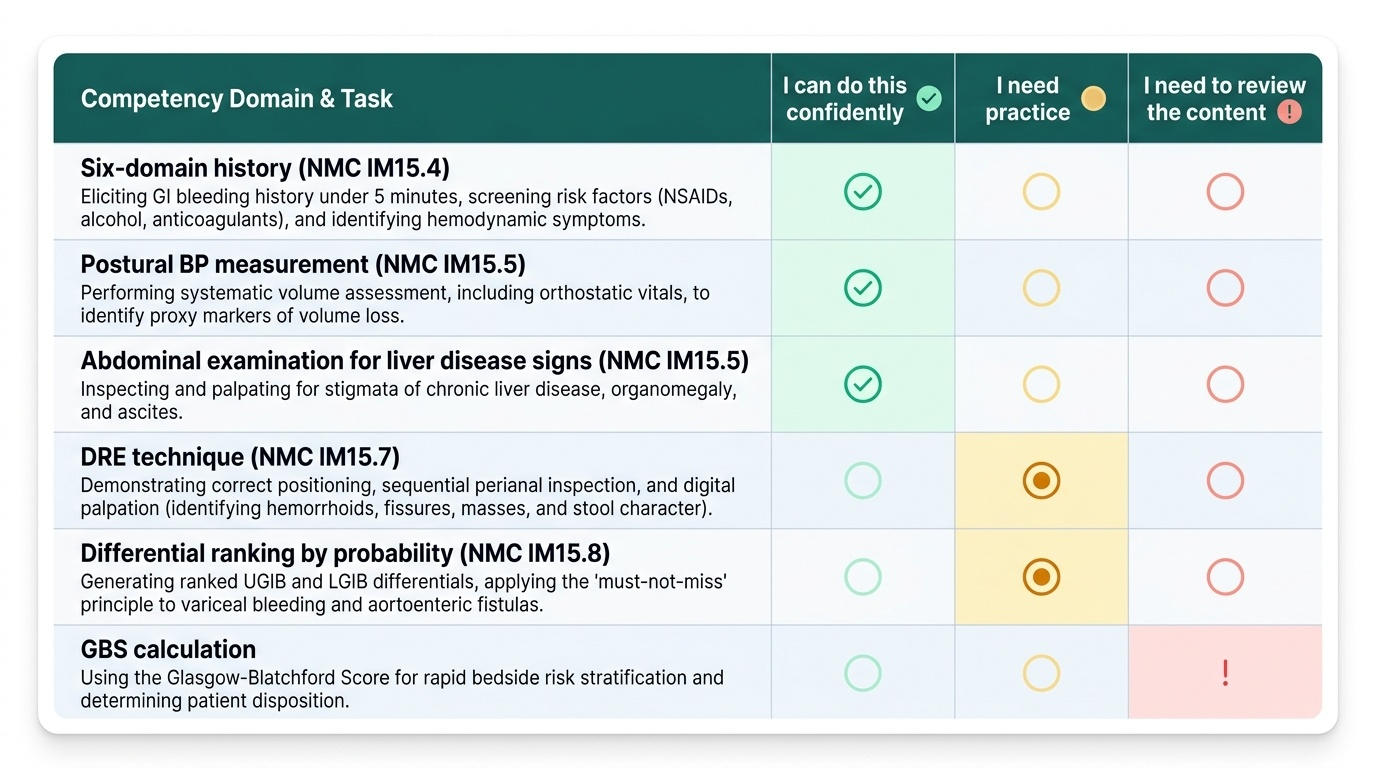
Having worked through the governing principles, structured history framework, physical examination technique including DRE, and differential construction, you are now at the point where you can assess your overall clinical evaluation competency against the NMC IM15.4, IM15.5, IM15.7, and IM15.8 standards. The self-assessment below maps directly to the key performance indicators that would be assessed in an OSCE station or a clinical viva on GI bleeding evaluation. Review each domain systematically and identify any areas where your confidence or knowledge gaps remain — these should direct your revision focus. Use the Glasgow-Blatchford Score to practise rapid bedside risk stratification on each of the applied cases you encountered in the preceding section: given the clinical data presented in Scenarios A and B, calculate the approximate GBS and determine whether each patient warrants urgent admission, standard admission, or outpatient management.
Provided image
Key self-assessment questions for each domain: History (IM15.4) — Can you elicit the six-domain history for GI bleeding in under 5 minutes, including a complete risk factor screen for NSAID use, alcohol, liver disease, prior surgery, and anticoagulants? Can you identify haemodynamic symptoms (postural presyncope, palpitation, breathlessness) as proxy markers of volume loss? Examination (IM15.5) — Can you perform a systematic volume assessment including postural BP measurement, and accurately examine the abdomen for stigmata of chronic liver disease, organomegaly, and ascites? DRE (IM15.7) — Can you demonstrate the correct positioning, perianal inspection sequence, and digital palpation technique, and accurately describe findings including haemorrhoids, fissure, mass, and stool character? Differential construction (IM15.8) — Can you generate a ranked differential for both UGIB and LGIB presentations, applying the must-not-miss principle and correctly placing variceal bleeding, aortoenteric fistula, and colorectal carcinoma in appropriate clinical contexts?