Page 11 of 19
IM15.{11-15,17-18} | GI Bleeding Treatment and Transfusion — SDL Guide
Learning Objectives
- Develop and document a treatment plan for acute GI bleeding including fluid resuscitation, blood and blood component transfusion, and specific haemostatic therapy
- Enumerate the indications for whole blood, packed red cells, FFP, platelets, and cryoprecipitate transfusion and describe the management of a mismatched transfusion
- Describe the pharmacology, indications, and side effects of vasopressors and vasoactive drugs used in upper GI bleeding (terlipressin, octreotide/somatostatin, vasopressin)
- Describe the indications, pharmacology, and adverse effects of acid-peptic disease pharmacotherapy including PPIs, H2 blockers, and H. pylori eradication regimens
- Determine appropriate specialist consultation based on haemodynamic status
- Counsel the patient and family about GI bleeding diagnosis and therapeutic options
INSTRUCTIONS
Treatment of GI bleeding requires coordinated decision-making across resuscitation, pharmacotherapy, transfusion medicine, endoscopy, and surgical consultation. This module gives you the complete pharmacological and clinical framework for every treatment modality used in UGIB and LGIB, and develops your skills in patient communication in a high-stakes emergency setting.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 47 — Gastrointestinal Bleeding (textbook)
- API Textbook of Medicine, 10th ed. — Gastrointestinal Haemorrhage (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed., Ch. 21 (textbook)
- British Society of Gastroenterology: UK guidelines on the management of upper GI bleeding, 2021 (guideline)
- EASL Clinical Practice Guidelines on the management of patients with decompensated cirrhosis, 2018 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the medical officer on call when the blood bank nurse phones you at 2 AM. A 60-year-old woman with oesophageal varices has received 3 units of packed red cells in the past 4 hours and is still bleeding. The gastroenterologist asks whether she is on terlipressin — you realise it was not started because the intern thought IV omeprazole was the same treatment. The haematologist asks for the latest platelet count — it is 38 × 10⁹/L. She has not had antibiotic prophylaxis. These are not one error — they are four separate, compounding treatment errors, each correctable with knowledge. The treatment of GI bleeding is pharmacologically nuanced: variceal and non-variceal bleeding require different drugs, transfusion decisions are evidence-based, and the patient and family need clear and compassionate communication in the middle of a frightening night. This module ensures you can provide all of this.
WHY THIS MATTERS
NMC competencies IM15.11 through IM15.18 represent the most clinically weighty portion of the GI bleeding curriculum — the treatment decisions. These encompass fluid resuscitation and blood product thresholds (IM15.11, IM15.12, IM15.13), vasoactive pharmacotherapy for variceal bleeding (IM15.14), acid-peptic pharmacotherapy and H. pylori eradication (IM15.15), specialist consultation triggers (IM15.17), and patient and family counselling (IM15.18). Getting any one of these wrong in clinical practice — omitting prophylactic antibiotics in variceal bleeding, using a liberal transfusion threshold when restrictive is indicated, confusing somatostatin with a PPI — contributes to measurable patient harm. This module synthesises the treatment framework that allows you to manage GI bleeding with confidence from the resuscitation room to the ward round.
RECALL
Recall the restrictive transfusion threshold of Hb <7 g/dL (or <8 g/dL in cardiovascular disease) from Module 1. Recall the Forrest classification of peptic ulcer stigmata and that high-dose IV PPI is indicated after endoscopic haemostasis for Forrest Ia/Ib/IIa/IIb lesions. Recall the variceal bleeding management framework: portal hypertension → oesophageal varices → rupture triggered by the portal pressure gradient exceeding 12 mmHg → management requires both portal pressure reduction (vasoactive drugs) and endoscopic haemostasis (band ligation). Recall that Helicobacter pylori infection and NSAID use are the two most important modifiable risk factors for peptic ulcer disease, and that eradication of H. pylori with appropriate antibiotics reduces the long-term rebleeding risk by 80–90%.
Clinical Presentation: Recognising Treatment-Determining Features
The treatment of GI bleeding is not monolithic — it is stratified by the type of bleeding (variceal vs non-variceal upper GI; lower GI), the severity of haemodynamic compromise, the patient's comorbidities, and the endoscopic findings. Before considering any specific pharmacotherapy, the treating physician must rapidly identify the treatment-determining features of each patient's presentation that switch between two fundamentally different treatment pathways.
The most consequential clinical branch point is variceal versus non-variceal UGIB. These two categories require different pharmacotherapy from the outset — before endoscopy confirms the source. When variceal bleeding is suspected clinically (stigmata of chronic liver disease, known portal hypertension, heavy alcohol use, prior variceal banding), a vasoactive drug should be started immediately without waiting for endoscopic confirmation. The treatment-determining features of the clinical presentation are therefore: (1) Does the patient have stigmata of chronic liver disease or known portal hypertension? → start vasoactive therapy (terlipressin or octreotide) and prophylactic antibiotics immediately. (2) Is the most likely cause peptic ulcer disease? → start high-dose IV PPI. (3) What is the haemodynamic status? → guides transfusion urgency and resuscitation intensity. (4) Are there complicating factors (anticoagulant use, thrombocytopaenia, coagulopathy, renal failure, cardiovascular disease) that require specific intervention adjustments?
For lower GI bleeding, the treatment-determining features are: haemodynamic status (whether emergency resuscitation is needed), rate of bleeding (whether the patient is stabilising or accelerating), and aetiology (diverticular bleeding typically self-resolves, while bleeding from a colorectal carcinoma or IBD requires disease-specific treatment). The majority of acute LGIB episodes (approximately 80%) resolve spontaneously with supportive care, and the physician's role is to support the patient haemodynamically, prevent transfusion-related complications, and ensure the source is identified before discharge.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
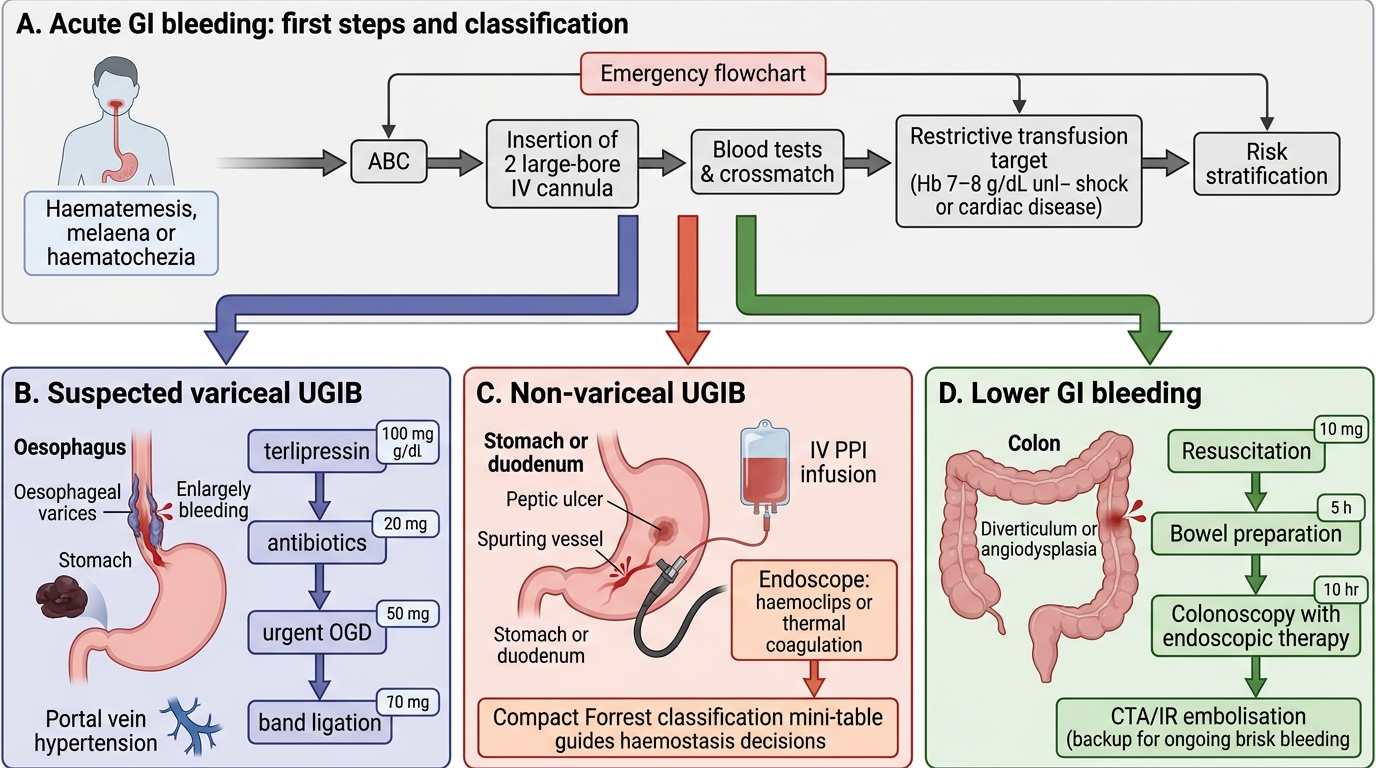
Acute GI Bleeding Treatment Decision Tree
Pathophysiology of Haemorrhage and the Rationale for Treatment
Understanding why each treatment modality works requires a clear model of the pathophysiology being targeted. The treatment choices in GI bleeding — vasoactive drugs, blood products, acid suppression, endoscopic haemostasis — are not arbitrary protocols; they are mechanistic interventions designed to interrupt specific pathophysiological processes. Internalising this causal chain transforms treatment from rote memorisation into a logical application of physiological principles, which is more durable and more adaptable when a patient presents atypically.
Variceal haemorrhage pathophysiology: Portal hypertension (portal venous pressure >12 mmHg) drives the formation of portosystemic collateral veins — oesophageal and gastric varices — as blood seeks low-resistance bypass routes around the congested portal system. When portal pressure exceeds the tensile strength of the variceal wall (governed by the Laplace relationship: tension = pressure × radius / wall thickness), the varix ruptures and haemorrhage occurs. The pharmacological rationale for vasoactive drugs (terlipressin, octreotide) is to reduce splanchnic blood flow and hence portal venous inflow, thereby lowering portal pressure and facilitating haemostasis at the variceal wall. Endoscopic band ligation physically ligates the varix, causing ischaemic necrosis and fibrosis that obliterates the vessel. Prophylactic antibiotics (ceftriaxone) address a secondary but equally important pathophysiological loop: bacterial infections in cirrhosis trigger the release of vasodilatory cytokines that raise portal pressure and dissolve platelet plugs, precipitating rebleeding — blocking this loop with antibiotics reduces early rebleeding mortality by approximately 10% independently of haemostasis.
Peptic ulcer haemorrhage pathophysiology: A peptic ulcer erodes through the gastric or duodenal mucosa into submucosal vessels. The severity of haemorrhage depends on the vessel calibre: small mucosal vessels produce oozing (Forrest Ib); a visible vessel represents an arterial stump that has temporarily thrombosed (Forrest IIa — high rebleed risk because gastric acid dissolves the thrombus); an actively spurting artery represents a failure of primary haemostasis (Forrest Ia — highest rebleed risk). The pharmacological rationale for high-dose IV PPI is to maintain gastric pH >6, the threshold above which platelet aggregation and fibrin clot formation are physiologically optimal — acid below pH 6 impairs platelet function and fibrinogen cross-linking. Endoscopic haemostasis (thermal coagulation, haemoclip) mechanically occludes the bleeding vessel. H. pylori eradication addresses the root cause — by eliminating the inflammatory stimulus that drives mucosal erosion, it removes the recurrence risk.
Haemorrhagic shock pathophysiology and treatment rationale: As outlined in the foundations module, blood loss triggers sympathoadrenal compensation (tachycardia, vasoconstriction) that maintains blood pressure until approximately 30% of circulating volume is lost. Beyond this, the lethal triad of hypothermia, metabolic acidosis, and coagulopathy becomes self-amplifying. Blood product therapy targets each component: packed red cells restore oxygen-carrying capacity and haemostatic platelet supply; FFP replaces coagulation factors depleted by haemorrhage, dilution, and hepatic dysfunction; cryoprecipitate restores fibrinogen; platelet transfusion restores primary haemostasis. The rationale for a restrictive transfusion strategy is not merely cost-reduction — it prevents the paradox of over-transfusion worsening outcomes: in variceal bleeding, raising haematocrit abruptly increases portal pressure via increased blood viscosity and flow, promoting rebleeding at the very site where haemostasis has just been achieved.
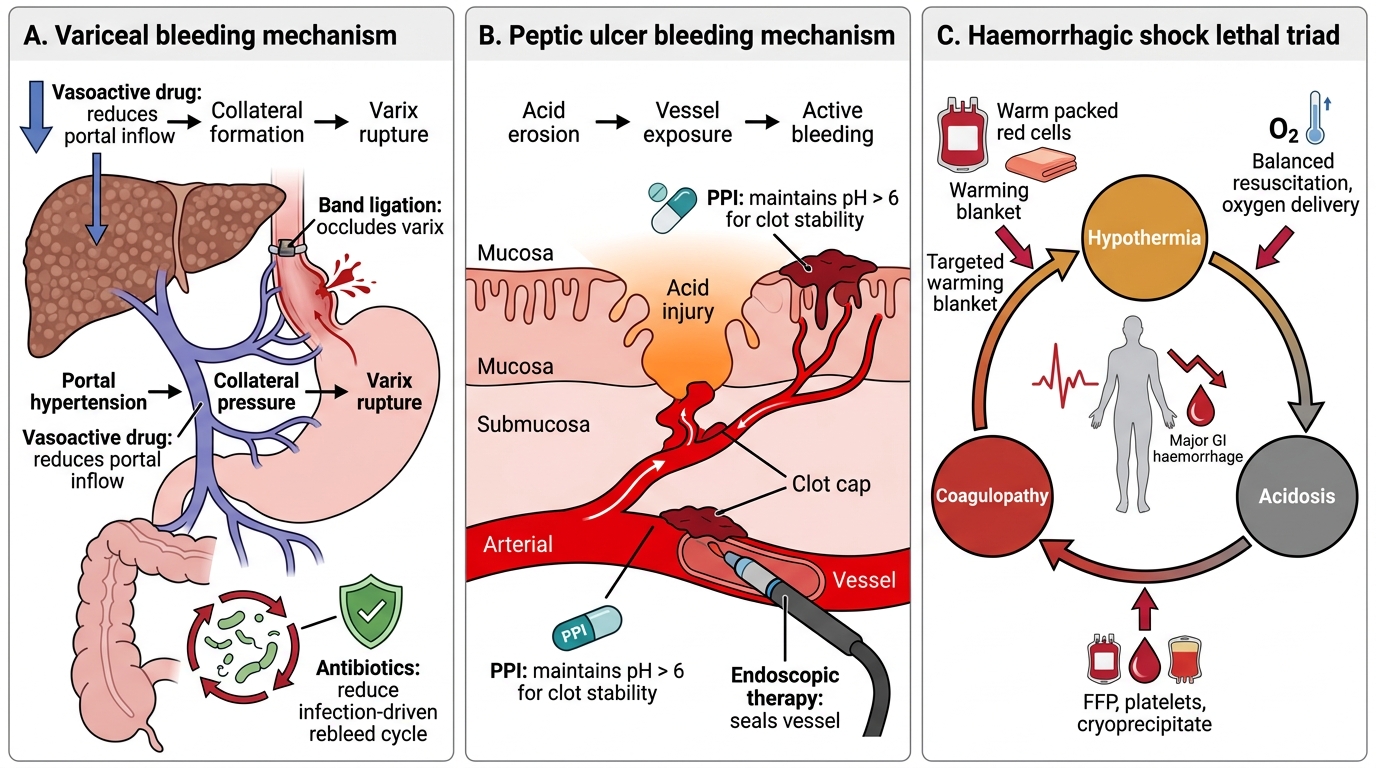
Mechanisms and Treatment Targets in Acute GI Bleeding
Risk Stratification and Investigation Before Treatment: Key Decision Points
Before initiating treatment, two diagnostic and risk-stratification decisions must be made explicitly, because they determine which treatment pathway is activated. These decisions draw on the investigation framework from the previous module, applied now specifically to guide treatment selection. Getting these decisions right — or failing to make them explicitly — is the difference between a coherent treatment plan and an accumulation of disconnected interventions.
Decision 1 — Is this variceal or non-variceal bleeding? This is the most consequential treatment-directing question in UGIB. The treatment bundles for these two categories are fundamentally different and must not be mixed. Variceal bleeding requires: terlipressin or octreotide (portal pressure reduction), IV ceftriaxone (antibiotic prophylaxis), endoscopic band ligation. Non-variceal peptic ulcer bleeding requires: high-dose IV PPI, endoscopic haemostasis guided by Forrest class, and H. pylori eradication. The clinical data that drive this decision come from the history (chronic liver disease, alcohol use, known portal hypertension) and examination (stigmata of portal hypertension — spider naevi, ascites, splenomegaly) gathered before endoscopy. When there is clinical uncertainty, start both a vasoactive drug (terlipressin or octreotide) AND a PPI simultaneously — this is the recommended practice for clinically ambiguous UGIB awaiting endoscopic diagnosis, because the risk of withholding a vasoactive drug in a variceal bleed (avoidable death) outweighs the modest cost of administering an unnecessary PPI in a non-variceal bleed.
Decision 2 — What is the Rockall Score / rebleeding risk after endoscopy? After OGD, the full Rockall Score (combining pre-endoscopy variables: age, shock, comorbidities — with endoscopic findings: diagnosis and stigmata by Forrest classification) provides the definitive risk stratification. A full Rockall Score of ≤2 identifies patients suitable for early discharge (within 24 hours of OGD) with outpatient follow-up — they have a very low rebleeding risk and very low mortality. A full Rockall Score of ≥5 identifies high-risk patients who require at least 72 hours of monitoring, high-dose IV PPI infusion (for peptic ulcer), and a low threshold for ICU escalation. The Rockall Score at this point is not merely academic — it determines the length of IV PPI treatment, the intensity of monitoring, and the threshold for surgical consultation.
Decision 3 — What complicating factors require protocol adjustment? Three specific patient populations require explicit investigation and treatment adjustments before the standard protocol is applied: (a) patients on anticoagulants or antiplatelets — hold or reverse anticoagulation (warfarin: vitamin K + FFP; DOACs: specific reversal agents if available — idarucizumab for dabigatran, andexanet alfa for factor Xa inhibitors); aspirin for a cardiac indication should generally be continued or restarted within 3–5 days of haemostasis, but clopidogrel/ticagrelor can usually be held for up to 5–7 days in low-thrombotic-risk patients; (b) cirrhotic patients — Child-Pugh and MELD scores must be calculated to risk-stratify the 30-day mortality and identify patients who may need TIPS; (c) patients with renal failure — avoid nephrotoxic contrast agents; dose-adjust medications; monitor fluid balance more closely to prevent TACO during resuscitation.
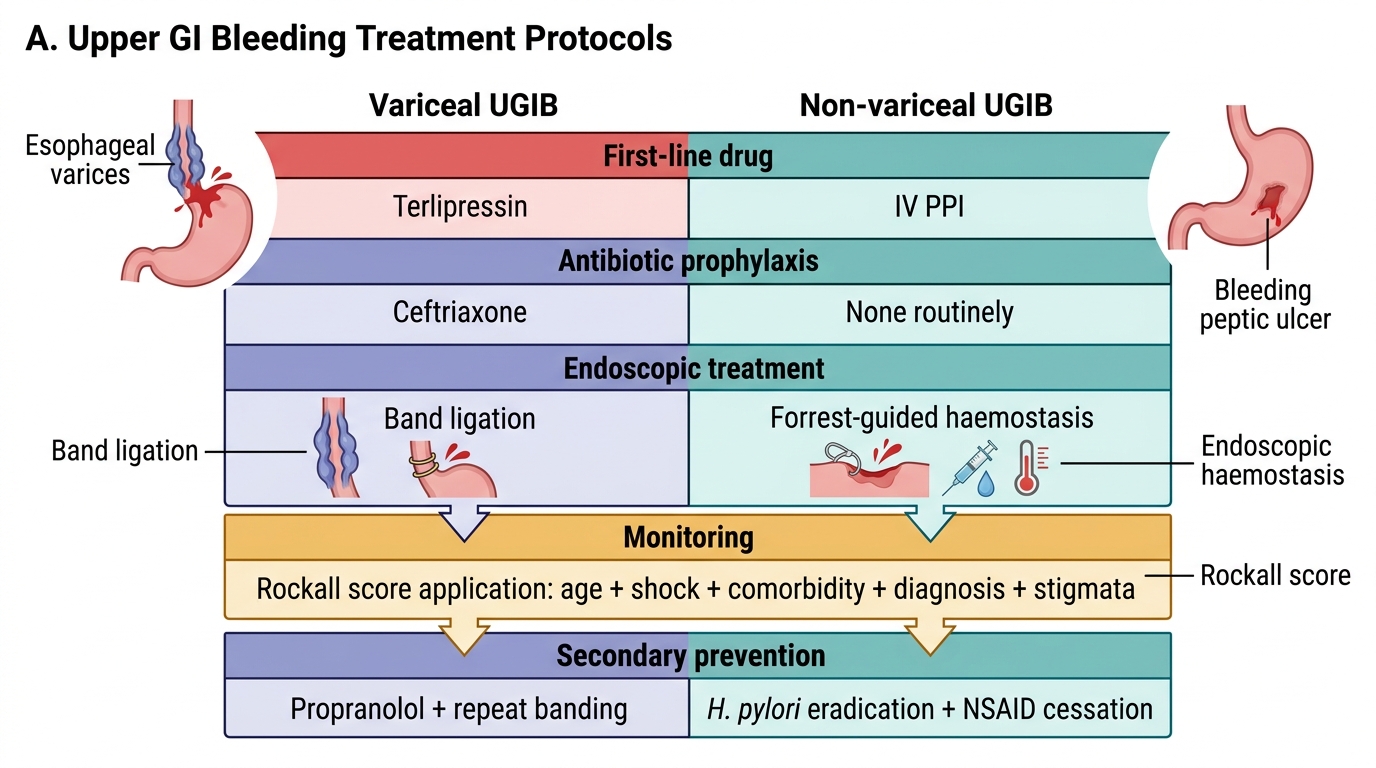
Variceal vs Non-variceal UGIB Treatment