Page 12 of 19
IM15.{11-15,17-18} | GI Bleeding Treatment and Transfusion — SDL Guide (Part 2)
Blood and Blood Product Transfusion
Transfusion medicine in GI bleeding encompasses four distinct clinical decisions: when to transfuse red cells, which blood product(s) are needed, what the specific indications for each product are, and how to recognise and manage a transfusion reaction. Getting these decisions right has a direct and measurable impact on patient outcomes, because both under-transfusion (inadequate oxygen delivery, end-organ ischaemia) and over-transfusion (increased portal pressure, rebleeding risk, transfusion-related lung injury) are harmful.
Provided image
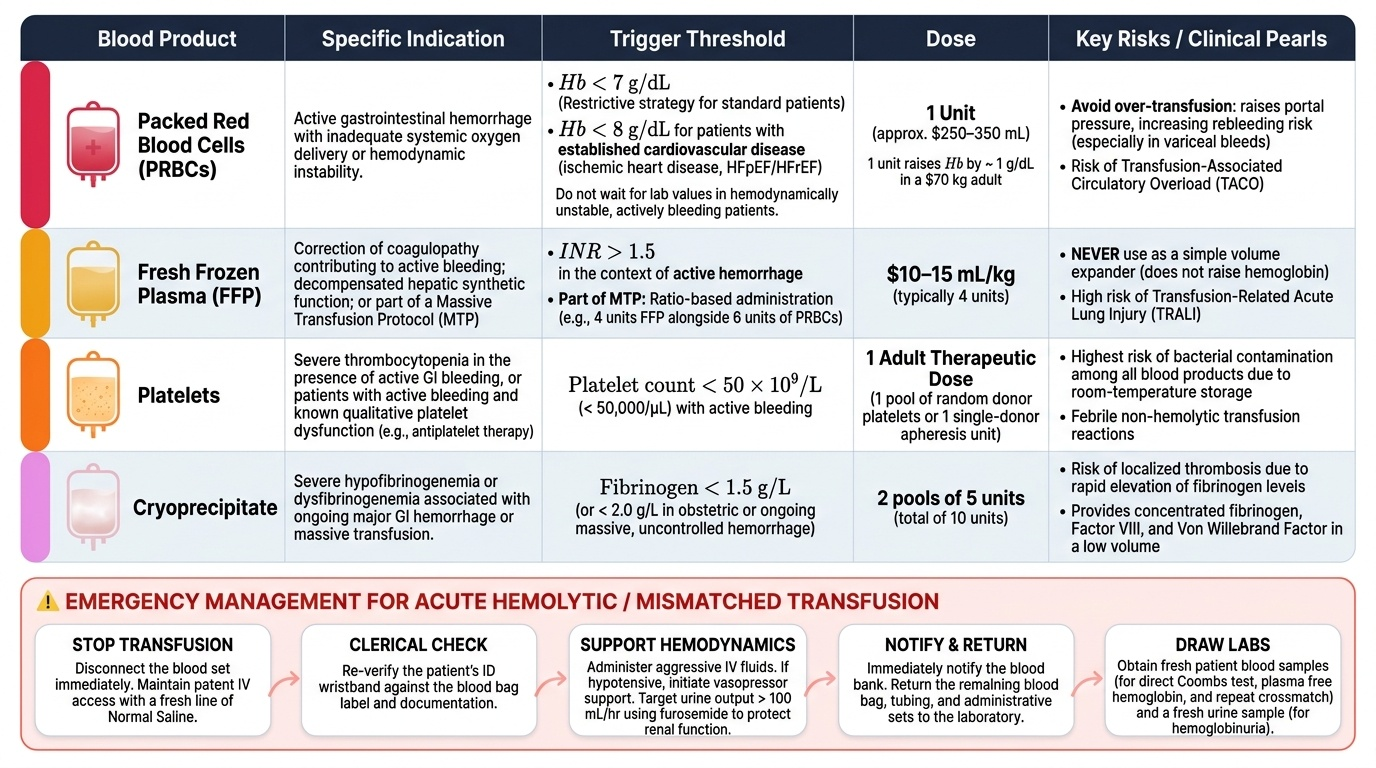
Packed red blood cells (PRBCs): The evidence-based restrictive transfusion strategy — transfusing PRBCs only when haemoglobin falls below 7 g/dL — is supported by the landmark Villanueva (2013) NEJM trial in UGIB, which demonstrated that a restrictive strategy reduced 45-day mortality from 10% to 5% and reduced rebleeding from 16% to 10% compared with a liberal threshold (Hb <9 g/dL). The restrictive strategy works by avoiding the adverse haemodynamic effects of over-transfusion (especially in variceal bleeding, where raising haematocrit transiently increases portal pressure). The threshold is modified upward to Hb <8 g/dL in patients with established cardiovascular disease (ischaemic heart disease, heart failure with reduced ejection fraction) where myocardial oxygen demand is higher and anaemia is less well tolerated. In the actively bleeding haemodynamically unstable patient, transfuse to haemodynamic restoration without waiting for a specific Hb level. Each unit of PRBCs (approximately 250–350 mL) raises haemoglobin by approximately 1 g/dL in a 70 kg adult without ongoing haemorrhage.
Fresh frozen plasma (FFP): FFP contains all coagulation factors and is indicated when coagulopathy contributes to haemorrhage. Specific indications in GI bleeding: (1) INR >1.5 in the context of active haemorrhage (give 4 units FFP); (2) Liver disease with decompensated hepatic synthetic function causing multifactorial coagulopathy; (3) Massive transfusion protocol (give 4 units FFP alongside every 6 units of PRBCs to prevent dilutional coagulopathy). Standard FFP dose is 10–15 mL/kg (typically 4 units). Note: FFP does NOT significantly raise haemoglobin and should NOT be used as a volume expander. It has risks including transfusion-related acute lung injury (TRALI) and must be used with clear coagulation indication.
Platelet concentrate: Transfuse platelets when the platelet count falls below 50 × 10⁹/L in a patient with active GI bleeding. The threshold is raised to 100 × 10⁹/L in patients with central nervous system bleeding (traumatic brain injury, intracranial haemorrhage). In cirrhotic patients with chronic thrombocytopaenia from hypersplenism, platelet transfusion is often needed if the count falls below 50 × 10⁹/L during an acute variceal bleed. Platelets are also indicated prior to invasive procedures (endoscopy, endotracheal intubation) if the count is below 50 × 10⁹/L. Each unit of platelet concentrate raises the platelet count by approximately 20–30 × 10⁹/L in the absence of ongoing consumption.
Cryoprecipitate: Cryoprecipitate is rich in fibrinogen, von Willebrand factor, factor VIII, and factor XIII. It is indicated when fibrinogen falls below 1.0–1.5 g/L (as occurs in severe liver disease, dilutional coagulopathy after massive transfusion, or disseminated intravascular coagulation). In GI bleeding with coagulopathy, fibrinogen should be specifically measured (not just INR/PT) and replaced if low — a fibrinogen below 1.5 g/L in the context of active haemorrhage is a significant independent predictor of ongoing bleeding.
Whole blood: Whole blood (containing red cells, plasma, and platelets) is rarely used in India outside of immediate military or emergency field settings. Component therapy (PRBCs, FFP, platelets, cryoprecipitate individually) is the standard of care in hospital settings and allows targeted replacement of specific deficits.
Mismatched blood transfusion (acute haemolytic transfusion reaction): An ABO-incompatible transfusion causes complement-mediated intravascular haemolysis — the most severe and potentially fatal transfusion complication. Clinical features develop within minutes of starting the transfusion: fever, rigors, lower back pain (from renal tubular haemoglobin deposition), haemoglobinuria (red or pink urine), hypotension, and in severe cases, disseminated intravascular coagulation (DIC) and acute renal failure. Management: stop the transfusion immediately, disconnect the unit, maintain IV access with normal saline, send the blood bag and a fresh sample from the patient to the blood bank for repeat crossmatch and culture, check a direct Coombs test, plasma-free haemoglobin, and urine dipstick. Maintain urine output with aggressive fluid hydration (target >1 mL/kg/hour); furosemide if oliguric; renal support if AKI develops. Other transfusion reactions — febrile non-haemolytic reactions, allergic reactions (urticaria), anaphylaxis (IgA-deficient patient receiving IgA-containing blood products), transfusion-associated circulatory overload (TACO), and TRALI — should all be recognised and managed according to the severity of reaction.
SELF-CHECK
A 52-year-old woman with a history of peptic ulcer disease presents with haematemesis. After initial resuscitation, her haemoglobin is 7.6 g/dL. She has no known cardiovascular disease. Her INR is 1.2 and platelet count is 195 × 10⁹/L. She is haemodynamically stable (BP 114/72, HR 88). What is the correct transfusion approach?
A. Transfuse 2 units PRBCs immediately — Hb 7.6 is low enough to require correction
B. Hold transfusion — Hb 7.6 g/dL is above the 7 g/dL restrictive threshold; she does not need blood right now
C. Transfuse 2 units PRBCs and 4 units FFP to cover the INR
D. Transfuse when Hb drops below 9 g/dL — that is the safer liberal threshold
Reveal Answer
Answer: B. Hold transfusion — Hb 7.6 g/dL is above the 7 g/dL restrictive threshold; she does not need blood right now
The restrictive transfusion threshold of Hb <7 g/dL applies to haemodynamically stable GI bleed patients without cardiovascular disease. This patient's Hb is 7.6 g/dL — above the 7 g/dL threshold. Withholding transfusion is correct and evidence-based (Villanueva 2013 trial showed harm with liberal strategies in UGIB). FFP is NOT indicated for INR 1.2 (threshold is >1.5 in active bleeding). Transfusing to Hb 9 g/dL is the discredited liberal strategy associated with higher rebleeding rates, especially in variceal bleeding where it raises portal pressure.
Vasoactive Pharmacotherapy for Upper GI Bleeding
Vasoactive drugs that reduce portal pressure are an essential component of variceal bleeding management. NMC competency IM15.14 requires knowledge of the indications, pharmacology, and side effects of vasopressors used in upper GI bleeding. Three classes of agents are clinically relevant: vasopressin analogues (terlipressin), somatostatin analogues (octreotide, somatostatin), and the older agent vasopressin itself (now largely replaced). These drugs work by reducing splanchnic blood flow and therefore portal venous inflow, decreasing portal pressure and promoting variceal haemostasis.
Provided image
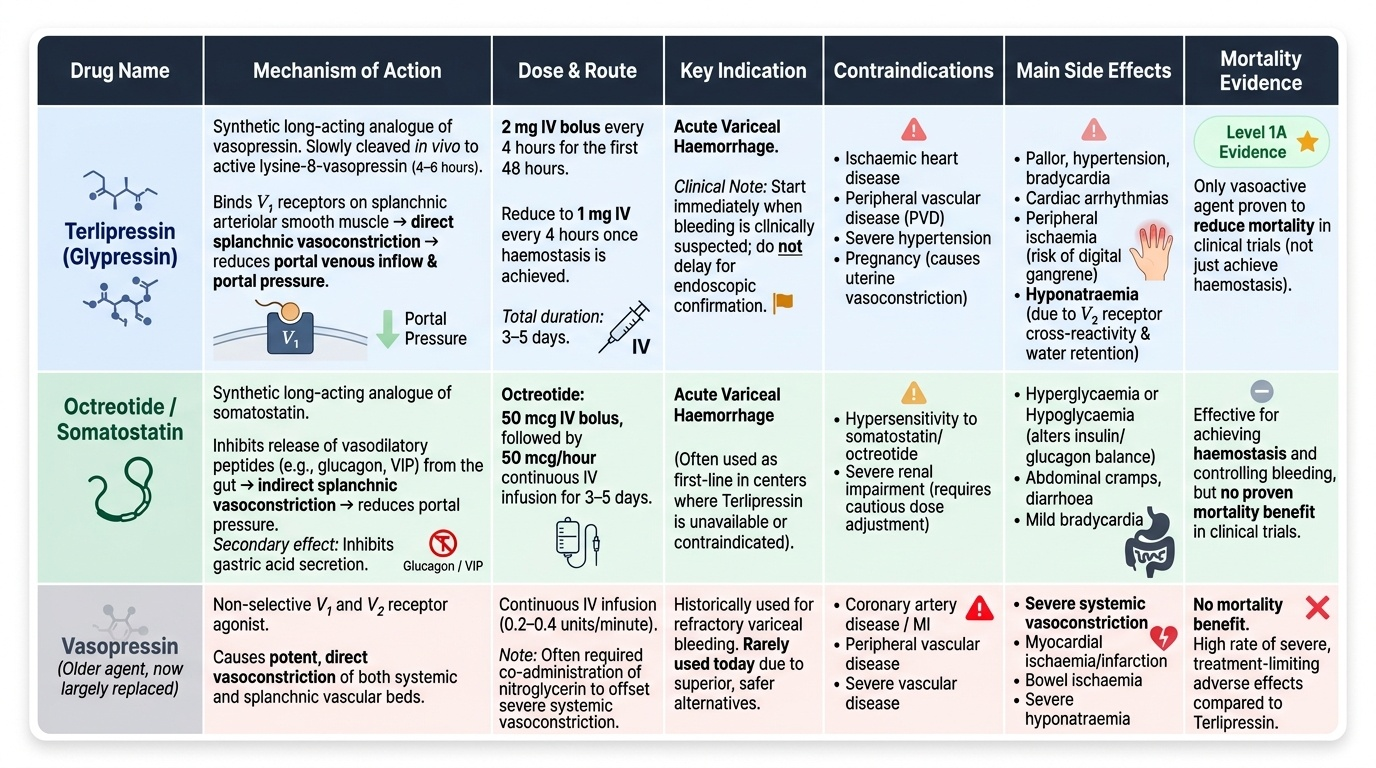
Terlipressin (glypressin): Terlipressin is a synthetic long-acting analogue of vasopressin. It is slowly cleaved in vivo to the active compound lysine-8-vasopressin over approximately 4–6 hours, providing a sustained portal pressure–lowering effect. Mechanism of action: binds to V1 receptors on splanchnic arteriolar smooth muscle, causing vasoconstriction of the splanchnic vasculature, reducing portal venous inflow and portal pressure. Indications: acute variceal haemorrhage — terlipressin is the only vasoactive agent with Level 1A evidence for reducing mortality from variceal bleeding in clinical trials, not merely for haemostasis. Dose: 2 mg IV every 4 hours for the first 48 hours, then 1 mg every 4 hours if haemostasis achieved, for a total of 3–5 days. Contraindications: ischaemic heart disease, peripheral vascular disease, hypertension, pregnancy (causes uterine vasoconstriction). Side effects: peripheral vasoconstriction causing pallor, hypertension, and bradycardia; more serious: cardiac arrhythmias, peripheral ischaemia (digital gangrene in high-dose or prolonged use), hyponatraemia (from water retention via V2 receptor cross-reactivity). Terlipressin should be started as soon as variceal bleeding is clinically suspected — it should not be withheld pending endoscopic confirmation.
Octreotide (and somatostatin): Octreotide is a synthetic long-acting analogue of somatostatin. Mechanism of action: inhibits the release of vasodilatory peptides (glucagon, VIP — vasoactive intestinal peptide) from the gut, causing indirect splanchnic vasoconstriction and reduced portal pressure; also inhibits gastric acid secretion. Dose of octreotide: 50 mcg IV bolus, followed by 50 mcg/hour continuous IV infusion for 3–5 days. Somatostatin (the parent molecule) has a shorter half-life and is given as a 250 mcg bolus followed by 250 mcg/hour infusion. Advantages over terlipressin: fewer cardiovascular side effects, safe in ischaemic heart disease (it does not cause coronary vasoconstriction). Side effects: nausea, abdominal cramps, headache, hyperglycaemia (inhibits insulin release), hypoglycaemia (inhibits glucagon), QT prolongation (rare). Evidence base for octreotide: it reduces portal pressure and improves haemostasis control, but unlike terlipressin, it has NOT shown a consistent mortality benefit as monotherapy in individual trials — it is used as an adjunct to endoscopic therapy and is the preferred agent where terlipressin is contraindicated.
Vasopressin: The original portal-hypotensive agent, vasopressin (ADH) acts on V1 receptors to cause splanchnic and systemic vasoconstriction. It has largely been replaced by terlipressin because of its very high rate of cardiovascular side effects (myocardial ischaemia, hypertension, mesenteric ischaemia, hyponatraemia). If used at all, it must be combined with nitroglycerin (glyceryl trinitrate infusion) to reduce the systemic vasoconstriction and cardiac afterload toxicity, at the cost of significantly increased monitoring requirements.
Prophylactic antibiotics in variceal bleeding: While not a vasopressor, antibiotic prophylaxis is an inseparable part of the variceal bleeding pharmacological bundle. Patients with cirrhosis who have variceal haemorrhage have a high risk of bacterial infection (spontaneous bacterial peritonitis, bacteraemia) in the perihaemorrhagic period, and infections trigger rebleeding and increase mortality. IV ceftriaxone 1 g/day for 7 days is the standard prophylaxis in patients with advanced cirrhosis (Child-Pugh B/C) or in settings with high prevalence of quinolone-resistant bacteria. Oral norfloxacin 400 mg twice daily for 7 days is an alternative in patients with less advanced disease and in settings without quinolone-resistant organisms. Antibiotic prophylaxis has Level 1A evidence for reducing bacterial infections, early rebleeding, and mortality in cirrhotic variceal bleeding and should not be omitted.
Acid-Peptic Disease Pharmacotherapy and H. pylori Eradication
For non-variceal UGIB — primarily peptic ulcer disease — pharmacological management centres on acid suppression to create an environment that supports haemostasis, and on H. pylori eradication to remove the causative infection and prevent recurrence. NMC competency IM15.15 requires knowledge of the indications, pharmacology, and side effects of acid-peptic disease pharmacotherapy. This knowledge is relevant beyond the emergency setting — it forms the backbone of long-term PUD management and secondary prevention of GI bleeding.
Proton pump inhibitors (PPIs): PPIs are the cornerstone of pharmacotherapy for peptic ulcer disease and UGIB from peptic ulcers. Mechanism of action: PPIs are prodrugs activated in the acidic environment of the parietal cell canaliculus to form reactive sulfonamide compounds that covalently and irreversibly inhibit the H⁺/K⁺-ATPase (proton pump) — the final enzyme in gastric acid secretion. Because the inhibition is irreversible, the duration of acid suppression outlasts the drug's plasma half-life, and full acid suppression requires 3–5 days of daily dosing (time for all parietal cell proton pumps to be cycled through and inhibited). Dosing in acute UGIB: IV pantoprazole or omeprazole 80 mg IV bolus, then 8 mg/hour continuous infusion for 72 hours (post-endoscopic therapy for Forrest Ia/Ib/IIa/IIb lesions). The rationale: gastric pH >6 is required for optimal platelet aggregation and fibrin clot stability — PPIs achieve and maintain this pH, reducing rebleeding risk. After 72 hours, switch to oral PPI once daily (omeprazole 20–40 mg, pantoprazole 40 mg, lansoprazole 30 mg, rabeprazole 20 mg, esomeprazole 40 mg). Side effects of PPIs: generally well tolerated; long-term use risks include: hypomagnesaemia (from intestinal magnesium malabsorption — particularly with prolonged use, causing tetany or arrhythmia); increased risk of Clostridioides difficile colitis (stomach acid normally kills ingested C. difficile spores); osteoporosis and fracture risk (long-term — impairs calcium absorption); community-acquired pneumonia (marginally increased by reduced acid barrier to oral colonisation); and nutritional deficiencies (B12, iron — acid required for absorption). Drug interactions: PPIs reduce clopidogrel efficacy (CYP2C19 inhibition reduces bioactivation of clopidogrel to its active metabolite) — omeprazole/esomeprazole have the most clinically significant interaction; pantoprazole or rabeprazole are preferred in patients on clopidogrel.
H2-receptor antagonists (H2RAs): Ranitidine, famotidine, and cimetidine block histamine H2 receptors on parietal cells, reducing gastric acid secretion but less completely than PPIs. They have largely been replaced by PPIs in acute GI bleeding management. Role in current practice: step-down therapy from IV PPI in inpatients, or as an alternative in patients with PPI hypersensitivity. Ranitidine was withdrawn from the market in 2020 due to contamination with N-nitrosodimethylamine (NDMA). Famotidine and nizatidine remain available. Tolerance (tachyphylaxis) develops with H2RAs — loss of efficacy with continuous use — which does not occur with PPIs.
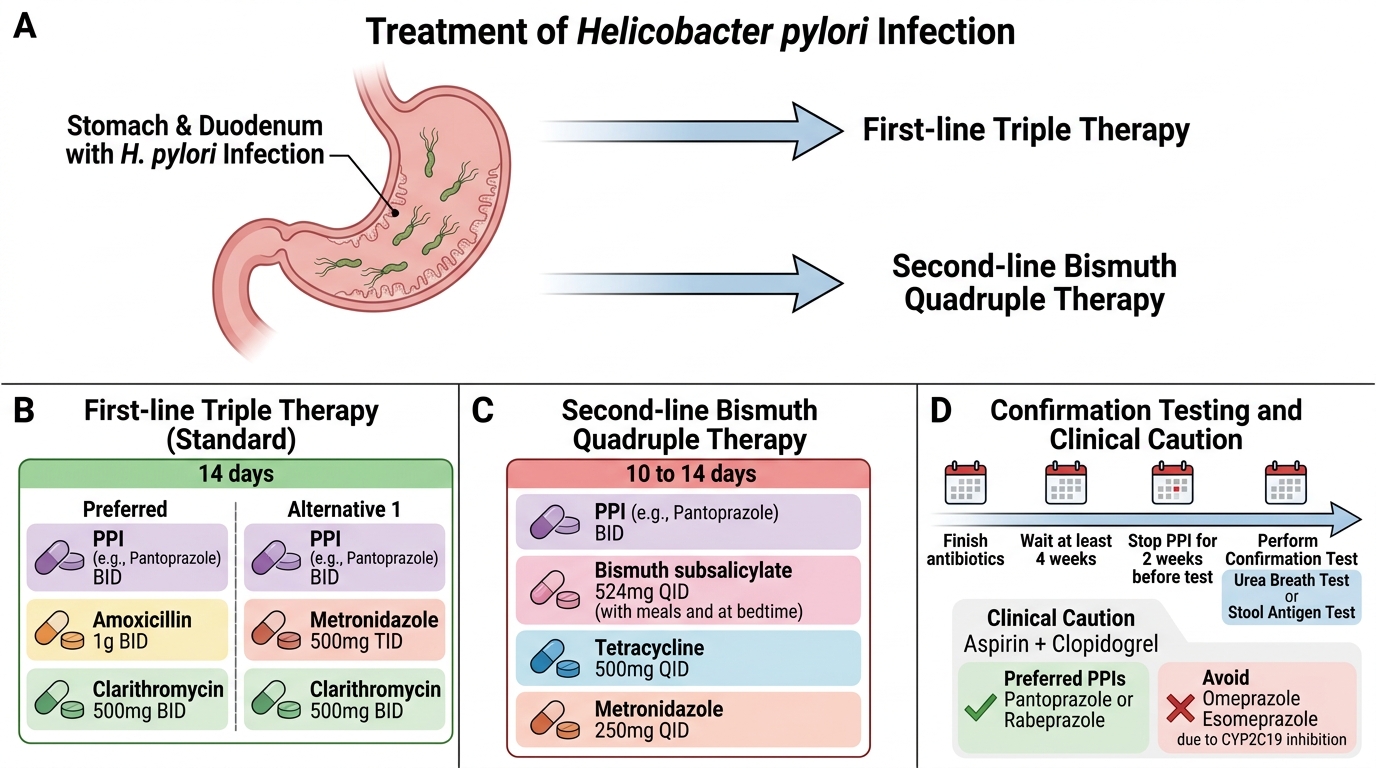
H. pylori eradication regimens: Testing for H. pylori should be performed in all patients with peptic ulcer disease presenting with GI bleeding. When confirmed positive, eradication therapy is mandatory — it reduces long-term rebleeding risk by approximately 80% and is far more cost-effective than lifelong PPI. Standard first-line triple therapy (7–14 days): PPI (standard dose twice daily) + clarithromycin 500 mg twice daily + amoxicillin 1 g twice daily (or metronidazole 400 mg twice daily if penicillin-allergic). Recommended duration: 14 days achieves higher eradication rates than 7 days in most populations and is the current NICE/Indian recommendation. Eradication rates with standard triple therapy are approximately 75–85% — declining due to increasing clarithromycin resistance. Bismuth quadruple therapy (for clarithromycin-resistant strains or second-line therapy): bismuth subcitrate 120 mg four times daily + tetracycline 500 mg four times daily + metronidazole 400 mg three times daily + PPI twice daily for 10–14 days — eradication rates approximately 85–90%. Confirm eradication using urea breath test or stool antigen test at least 4 weeks after completing eradication therapy and at least 2 weeks after stopping PPI (to avoid false-negatives). Do NOT use serology — it remains positive indefinitely after eradication and cannot confirm cure.
H. pylori Eradication Regimen Summary
SELF-CHECK
A 55-year-old man with a bleeding peptic ulcer on antiplatelet therapy (aspirin + clopidogrel) is started on an IV PPI infusion after successful endoscopic haemostasis. Which PPI is most appropriate given his dual antiplatelet use?
A. Omeprazole — it is the most potent PPI
B. Esomeprazole — it has the longest half-life
C. Pantoprazole or rabeprazole — they have the least CYP2C19 inhibition and therefore minimise the interaction with clopidogrel
D. Ranitidine — H2 blockers do not interact with clopidogrel
Reveal Answer
Answer: C. Pantoprazole or rabeprazole — they have the least CYP2C19 inhibition and therefore minimise the interaction with clopidogrel
Omeprazole and esomeprazole are potent CYP2C19 inhibitors. Clopidogrel is a prodrug requiring CYP2C19-mediated bioactivation to its active antiplatelet metabolite — CYP2C19 inhibition by omeprazole/esomeprazole reduces the active metabolite level and antiplatelet efficacy. Pantoprazole and rabeprazole have minimal CYP2C19 inhibition and are the preferred PPIs in patients on clopidogrel. Ranitidine (an H2 blocker) was withdrawn from the market in 2020 due to NDMA contamination and is no longer available.