Page 8 of 19
IM16.8-12 | Diarrheal Disorder Diagnostic Testing — SDL Guide
Learning Objectives
- Choose and interpret CBC and stool examination (physical, saline wet preparation, iodine preparation, modified Ziehl-Neelsen) in a patient with acute and chronic diarrhoea
- Identify common parasitic causes of diarrhoea under the microscope including Entamoeba histolytica (trophozoite with erythrophagocytosis; cyst with 4 nuclei), Giardia intestinalis (pear-shaped trophozoite; cyst with 4 nuclei and median bodies), and Cryptosporidium parvum (pink oocysts on MZN stain)
- Describe the hanging-drop preparation technique for Vibrio cholerae and identify its characteristic darting motility
- Enumerate the specific indications for stool and blood cultures in acute diarrhoeal disease
- Discuss the indications for advanced investigations (serology, colonoscopy, imaging, biopsy) in chronic diarrhoea, applying each to a clinical scenario
INSTRUCTIONS
This module builds practical diagnostic skills in diarrhoeal disorders — stool microscopy morphology, hanging-drop technique, and the clinical logic of selecting advanced investigations. For the microscopy sections, supplement reading with laboratory sessions: identify E. histolytica, Giardia, and Cryptosporidium on actual microscopy slides or validated digital image banks. The investigation selection principles should be practised on clinical vignettes.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 43 — Diarrhoea and Constipation; Ch. 228 — Infections of the Gastrointestinal Tract (textbook)
- API Textbook of Medicine, 10th ed., Ch. 7 — Gastroenterology (textbook)
- Ananthanarayan and Paniker's Textbook of Microbiology, 10th ed., Ch. 35 — Vibrio; Ch. 49 — Intestinal Protozoa (textbook)
- British Society of Gastroenterology Guidelines on Inflammatory Bowel Disease, 2019 (guideline)
- European Society for the Study of Coeliac Disease (ESsCD) Guideline, 2019 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A junior doctor in a district hospital in rural Karnataka is facing three patients with diarrhoea simultaneously. The first is a 7-year-old girl with acute watery diarrhoea and moderate dehydration. The second is a 42-year-old man with two weeks of mucoid bloody stools and fever. The third is a 28-year-old returning from a six-month rural posting with 3 months of fatty, floating stools and a 9 kg weight loss. The hospital has a basic laboratory: a microscope, Gram stain reagents, Ziehl-Neelsen stain, routine culture plates, and a basic haematology analyser. No colonoscope. No serological tests on site. The doctor needs to decide — for each patient — which tests to order, which to skip, and what results to actively look for under the microscope. Ordering every available test on every patient is not care; it is noise. This module teaches you to select, perform, interpret, and prioritise diagnostic tests in diarrhoeal disorders — matching the test to the clinical question and the setting.
WHY THIS MATTERS
Diagnostic competencies IM16.8–IM16.12 span five distinct skills: choosing and interpreting CBC and stool examination (IM16.8), identifying parasitic causes under the microscope (IM16.9), identifying Vibrio cholerae on hanging-drop preparation (IM16.10), knowing the indications for stool and blood cultures (IM16.11), and knowing when to request advanced investigation — serology, colonoscopy, imaging, and biopsy — for chronic diarrhoea (IM16.12). The first three are Skills with Hands competencies (SH) — assessed by performance, not just knowledge. You may be asked to identify a specific organism on a microscopy image in the professional examination, to interpret a stool result report, or to justify your choice of investigation in a clinical vignette. IM16.11 and IM16.12 are Knowledge with Application (KH) — you must not only recall the indications but apply them to a clinical scenario and explain why the test is ordered at that point in the workup, not earlier.
RECALL
From the Foundations SDL: stool osmotic gap = measured stool osmolality − 2×(stool Na + stool K); <50 = secretory; >125 = osmotic. From the Clinical Evaluation SDL: faecal leucocytes indicate mucosal invasion (inflammatory/invasive mechanism). From your Microbiology training: recall the basic morphological features of the principal protozoan parasites relevant to diarrhoea — Giardia intestinalis (pear-shaped trophozoite with two nuclei, central axoneme; cyst is oval with four nuclei), Entamoeba histolytica (trophozoite with ingested erythrocytes — erythrophagocytosis — pathognomonic; cyst with four nuclei), Cryptosporidium parvum (small 4–6 µm oocyst; modified Ziehl-Neelsen staining only). For Vibrio cholerae: recall that cholera is diagnosed clinically in outbreaks; the hanging-drop wet preparation demonstrates characteristic darting motility of the comma-shaped bacillus, which is the key identification feature in the field or district laboratory. These morphological features are what you must be able to identify under the microscope, as assessed in IM16.9 and IM16.10.
Complete Blood Count and Stool Examination: Indication and Technique
The complete blood count (CBC) and stool examination form the first-line diagnostic pair in diarrhoeal disease for most clinical settings. Understanding their indication, technique, and interpretation together provides rapid, actionable diagnostic information. These tests are available at every district hospital and most primary health centres in India, making them the practical cornerstone of diarrhoeal diagnosis in resource-limited settings. The result of a stool examination, properly performed and interpreted, can confirm a specific aetiological diagnosis in many cases within 30 minutes of sample collection — faster than any molecular test, at a fraction of the cost, and without any special infrastructure. Developing this skill — including knowledge of what each test detects, what preparation technique each requires, and what morphological features constitute a positive result — is essential for a physician practising in India. The key clinical skill is not to order them on every patient with loose stools, but to understand which component of each result is diagnostically informative for the specific clinical presentation — and to actively look for those signals rather than accepting a report passively.
Indications for CBC in diarrhoeal disease:
- All patients with moderate-to-severe dehydration: baseline haematocrit (haemoconcentration in severe dehydration), electrolytes (hyponatraemia, hypokalaemia), creatinine and urea (pre-renal AKI)
- Patients with fever and acute diarrhoea: white cell count differential — leucocytosis with neutrophilia suggests bacterial invasion; leucopenia with relative lymphocytosis suggests enteric fever (typhoid) — the classic 'relative bradycardia' on examination + leucopenia on CBC is a significant pointer to Salmonella typhi
- Patients with chronic diarrhoea or suspected malabsorption: haemoglobin, MCV (microcytic = iron deficiency; macrocytic = B12/folate deficiency; dimorphic = combined), eosinophilia (suggests helminthic parasitosis — hook-worm, strongyloides, ascariasis)
- Patients with bloody diarrhoea (dysentery): platelet count and renal function — to screen for HUS (haemolytic uraemic syndrome) when diarrhoea is caused by STEC; blood film for fragmented RBCs (schistocytes)
- IBD suspected: inflammatory markers (CRP, ESR), serum albumin, iron studies
Stool examination (physical, microscopic, chemical) is the single most informative first-line test for infectious diarrhoea. A properly performed stool examination yields more diagnostic information than any other bedside investigation. The examination has three levels:
Level 1 — Physical (macroscopic) examination:
Examine the stool sample for: (a) consistency (watery/liquid, loose/semi-formed, formed); (b) colour — pale/yellow-green (viral, ETEC), rice-water (cholera), bright-red blood (lower GI — dysentery, IBD, rectal carcinoma), dark-maroon (mid GI), tarry/black (melaena = upper GI), pale/greasy (steatorrhoea = malabsorption); (c) presence of visible blood, mucus, and/or pus; (d) odour — foul-smelling = steatorrhoea; distinctive foul = C. difficile.
Level 2 — Microscopic examination:
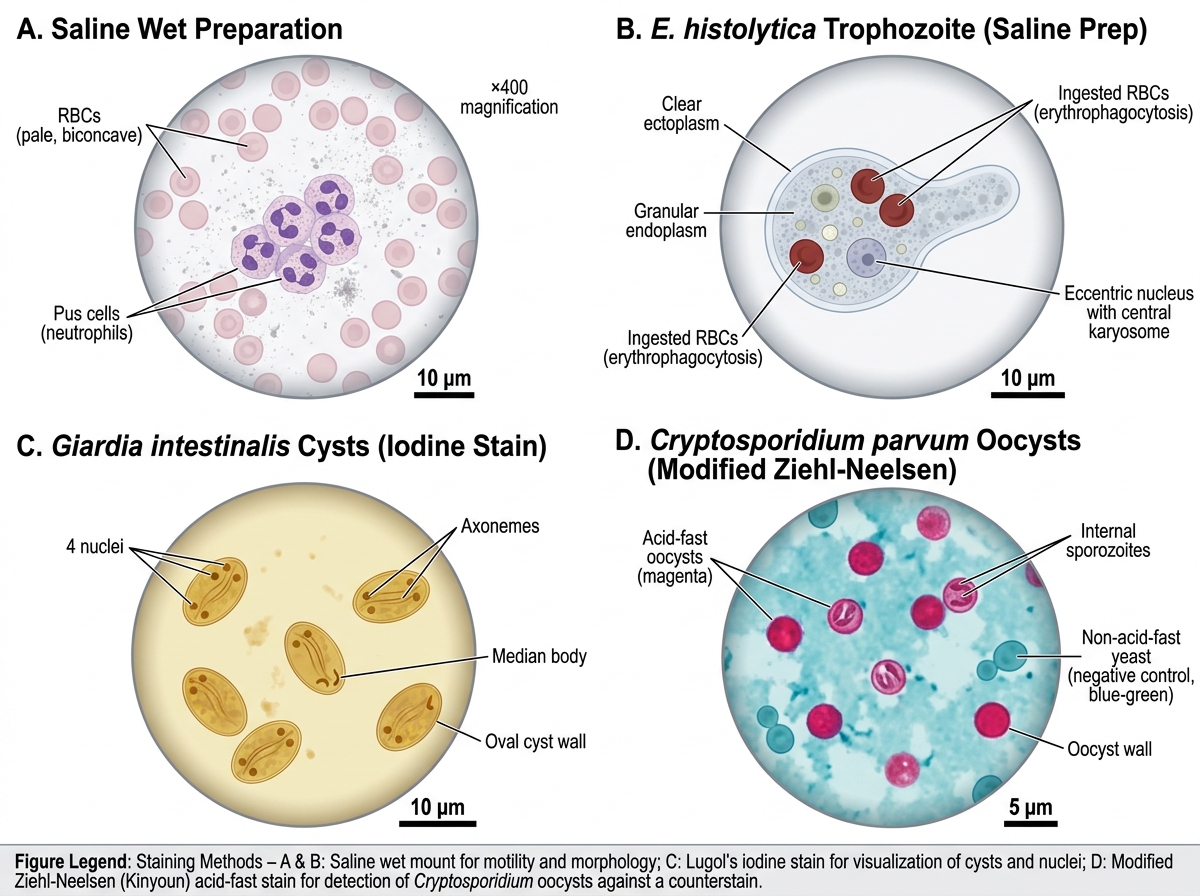
- Saline wet preparation: place a small amount of fresh stool in a drop of normal saline on a glass slide, cover with coverslip, examine under ×10 and ×40 objective. Identify: red blood cells (dysentery/IBD — normally absent in stool), white blood cells/pus cells (faecal leucocytes — present in invasive bacterial diarrhoea and IBD, absent in secretory diarrhoea), Entamoeba histolytica trophozoites (motile, with ingested RBCs — erythrophagocytosis), Giardia trophozoites (pear-shaped, tumbling motility on fresh sample), helminth eggs and larvae (hookworm ova, Ascaris ova, Strongyloides larvae)
- Iodine preparation (Lugol's iodine added to saline wet preparation): stains cysts for identification — Giardia cysts (oval, 4 nuclei, median bodies visible), E. histolytica cysts (round, 4 nuclei, chromatoid bodies), E. coli cysts (8 nuclei, non-pathogenic — distinguish from E. histolytica)
- Modified Ziehl-Neelsen (cold acid-fast stain): specifically for Cryptosporidium parvum and Cyclospora cayetanensis — appear as pink/red oocysts against a blue background
Level 3 — Chemical test: Faecal occult blood (FOB / guaiac test) detects non-visible blood; useful in chronic diarrhoea workup when colorectal carcinoma is suspected and no gross bleeding is seen.
Stool Microscopy Reference Plate: Parasitic and Cellular Findings
Identifying Parasites Under the Microscope
The identification of parasitic causes of diarrhoea under the microscope is a core procedural skill (IM16.9) that is tested in the MBBS professional examinations both as practical microscopy and as image-based MCQs. The three most important parasites to recognise in a stool specimen for the purposes of this competency are Entamoeba histolytica, Giardia intestinalis (lamblia), and Cryptosporidium parvum. Each has specific morphological features that must be memorised precisely, and each requires a specific preparation technique to be identified reliably. Additional parasites relevant to Indian practice are also covered below for comprehensive competency. The consequence of missing a parasitic diagnosis — sending a patient home after a negative routine culture when giardiasis or amoebiasis was causing malabsorptive or invasive diarrhoea — is continued illness, nutritional deficiency, and in the case of amoebiasis, the risk of invasive extraintestinal disease. Confidence at the microscope is therefore not an optional laboratory skill; it is a frontline clinical competency.
Entamoeba histolytica (IM16.9 — primary target):
Stool examination demonstrates two forms depending on whether the infection is invasive or colonisation:
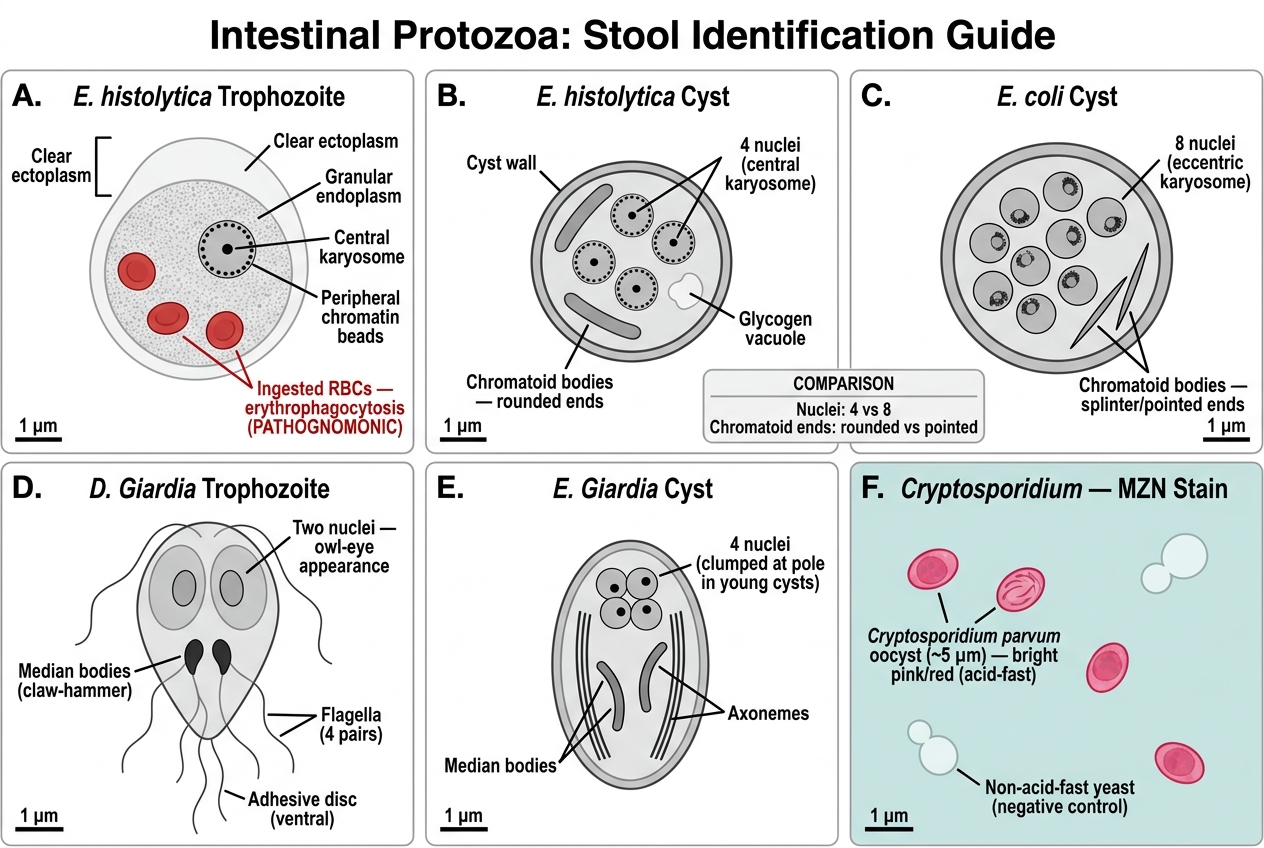
- Trophozoite (invasive disease, fresh liquid stool, immediate examination essential): Size 15–20 µm in diameter in the active form. Morphological hallmark: erythrophagocytosis — engulfed intact red blood cells within the trophozoite's cytoplasm. No other intestinal protozoan trophozoite engulfs RBCs — this feature is pathognomonic for E. histolytica. The trophozoite shows directional, progressive, 'ameboid' motility with a clear ectoplasm and granular endoplasm (glass morphology). The nucleus has a central karyosome and fine, uniformly distributed chromatin around the nuclear membrane. Examination must be performed within 30 minutes of sample collection (trophozoites lyse rapidly in cooled stool).
- Cyst (formed or semi-formed stool, carrier/non-invasive stage): Size 10–15 µm, spherical/round. Lugol's iodine stain reveals: 4 nuclei (mature cyst) with fine peripheral chromatin and central karyosomes; chromatoid bodies (sausage-shaped crystalline RNA collections with rounded ends, visible in early cysts — pathognomonic when present; absent in the morphologically similar non-pathogenic Entamoeba coli which has 8 nuclei in mature cyst).
- Differentiation from E. coli (non-pathogenic): E. coli trophozoite has a 'dirty cytoplasm' (contains ingested bacteria and debris but NOT red blood cells — the key distinction); mature cyst has 8 nuclei (not 4); chromatoid bodies have pointed/splinter-shaped ends (vs rounded ends in E. histolytica).
Giardia intestinalis (lamblia):
- Trophozoite (duodenal aspirate or fresh diarrhoeal stool): Size 10–20 µm long, 5–15 µm wide. Characteristic pear-shaped (pyriform) body, bilaterally symmetrical. Two nuclei (one on each side — the 'owleye' appearance in anterior view). Four pairs of flagella (one pair anterior, one ventral, one caudal, one posterior-lateral). A ventral adhesive disc (sucking disc) for attachment to intestinal villi. Tumbling/falling-leaf motility on fresh wet preparation.
- Cyst (formed stool — more commonly found, does not require rush microscopy): Size 8–19 µm, oval. 4 nuclei (often at one pole). Median bodies (two curved sausage-shaped structures) visible on iodine stain. Flagella may be visible as thin fibrils within the cyst wall.
- Clinical context: giardiasis causes upper small intestinal malabsorption — no blood, no fever, pale/fatty/floating stools, abdominal bloating, flatulence. Diagnosis sometimes requires examination of three separate stool samples (sensitivity of single stool for cysts is 70–75%; three samples achieve ~90%).
Cryptosporidium parvum:
- Standard wet preparation is UNRELIABLE — oocysts are small (4–6 µm) and easily missed
- Modified Ziehl-Neelsen (MZN) or modified Kinyoun staining — required for specific diagnosis. On MZN: oocysts stain pink/red (acid-fast), appear as small bright pink dots against a blue background from the counterstain. Spherical, with a visible internal sporozoite granulation pattern in some oocysts.
- Clinical context: self-limiting (1–2 weeks) in immunocompetent; severe, potentially fatal chronic diarrhoea in HIV/AIDS (CD4 <200) — a WHO AIDS-defining illness.
Other relevant parasites (India-specific):
- Hookworm (Ancylostoma duodenale, Necator americanus): ova on saline wet preparation — thin-shelled, oval, 4–8 cell embryo stage at passage; iron-deficiency anaemia from chronic small-intestinal blood loss
- Ascaris lumbricoides: large ova (60–75 µm), thick outer mammillated (bumpy) cortex; fertile = bile-stained brown, thick shell; infertile = elongated, irregular
- Strongyloides stercoralis: rhabditiform larvae (short buccal cavity) in fresh stool — distinction from hookworm larvae (longer buccal cavity) is important; Strongyloides can cause hyperinfection syndrome in immunocompromised
- Trichuris trichiura (whipworm): barrel/lemon-shaped ova with transparent plugs at both poles
Intestinal Protozoa: Stool Identification Guide
SELF-CHECK
A 30-year-old man presents with 10 days of bloody mucoid diarrhoea and tenesmus. A saline wet preparation of fresh stool is examined immediately. You find motile organisms approximately 18 µm in size with a granular endoplasm, clear ectoplasm, and visible engulfed intact red blood cells within the cytoplasm. What is the DIAGNOSIS, and which morphological feature is PATHOGNOMONIC?
A. Giardia intestinalis trophozoite; pear-shaped body with two nuclei
B. Entamoeba coli trophozoite; dirty cytoplasm with engulfed bacteria
C. Entamoeba histolytica trophozoite; erythrophagocytosis (ingested RBCs in cytoplasm)
D. Cryptosporidium parvum oocyst; pink staining on modified Ziehl-Neelsen
Reveal Answer
Answer: C. Entamoeba histolytica trophozoite; erythrophagocytosis (ingested RBCs in cytoplasm)
Entamoeba histolytica trophozoite — the pathognomonic feature is erythrophagocytosis: ingested intact red blood cells within the trophozoite's cytoplasm. No other intestinal protozoan engulfs red blood cells. The fresh stool with immediate examination is correct technique, as trophozoites lyse within 30 minutes of cooling. Entamoeba coli trophozoites have a 'dirty cytoplasm' containing bacteria and debris but NOT red blood cells — this distinguishes the non-pathogenic E. coli from the pathogenic E. histolytica. Giardia is pear-shaped with two nuclei but causes malabsorptive, non-bloody diarrhoea. Cryptosporidium requires modified Ziehl-Neelsen staining and appears as small pink oocysts, not motile trophozoites.
Identifying Vibrio cholerae on Hanging-Drop Preparation
The hanging-drop preparation for Vibrio cholerae is a specific microbiological technique (IM16.10) used in acute outbreak settings and district hospitals where culture facilities may be limited or delayed. It is a rapid, bedside-compatible examination that provides presumptive identification of V. cholerae based on characteristic motility, allowing prompt initiation of outbreak control measures and appropriate treatment before culture confirmation is available. This technique is no longer the standard for diagnostic confirmation in well-resourced settings (culture on TCBS agar + serological typing is gold standard), but remains a competency requirement in the NMC curriculum because Indian clinicians routinely work in settings where culture is delayed by 24–48 hours and clinical decisions must be made immediately.
Principle of the hanging-drop preparation:
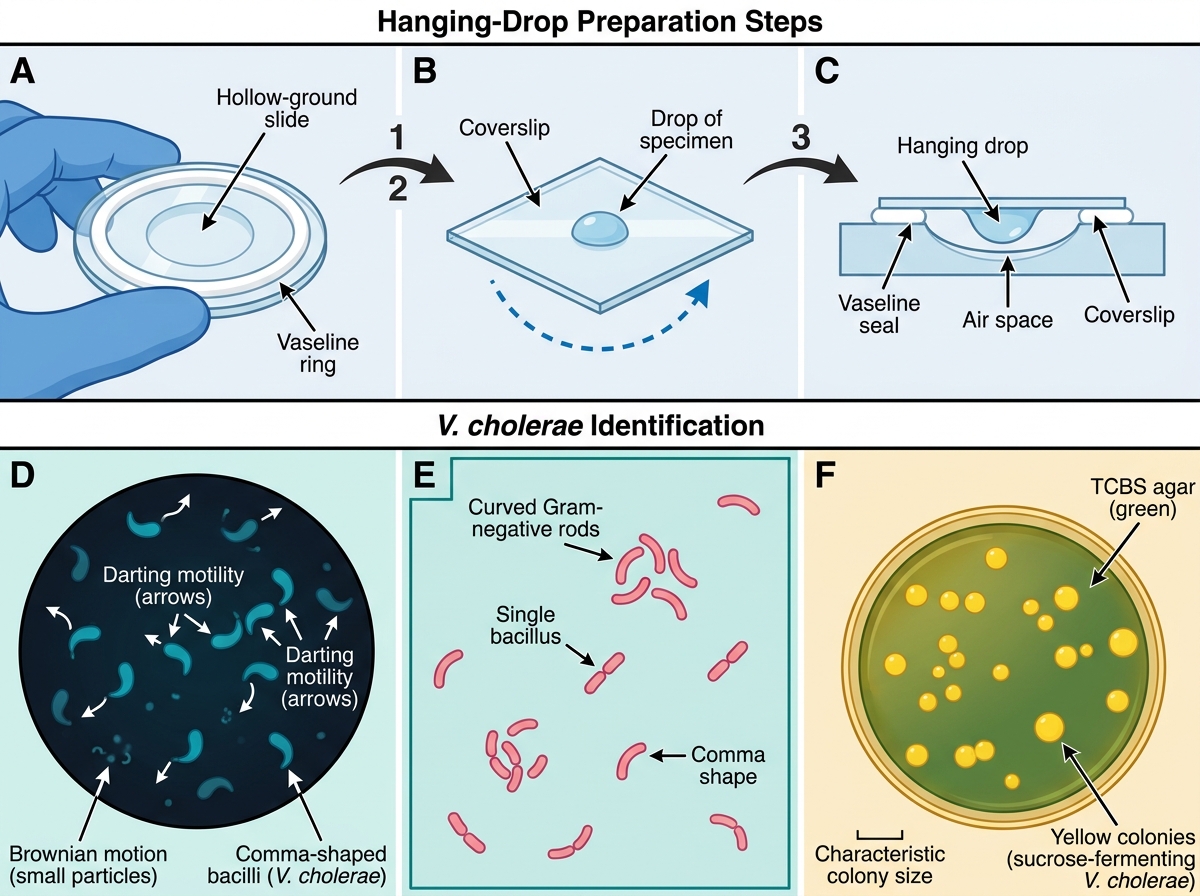
A small drop of liquid stool (or stool suspension) is placed in the centre of a clean coverslip. A hollow-ground or depression slide is prepared with Vaseline on the rim of the well. The coverslip is inverted over the hollow and pressed gently — the drop of specimen now hangs from the underside of the coverslip, suspended in a sealed, moist chamber that prevents desiccation. The preparation is examined under the microscope (×40 objective, darkfield or reduced illumination) immediately after preparation — the key is that the specimen must be examined while organisms are still viable and motile.
Characteristic motility of V. cholerae:
Vibrio cholerae is a Gram-negative, curved rod (comma-shaped: vibrio morphology) approximately 1.5–3 µm long × 0.5 µm wide. It possesses a single polar flagellum that drives rapid, characteristic motility described as 'darting' or 'shooting-star' motility — the organism moves in rapid, straight-line bursts across the field, pausing briefly, then darting again. This is distinct from the slower, tumbling motility of Giardia trophozoites or the ameboid locomotion of E. histolytica. The darting motility is visible at ×40 as brisk, directional, rapid movement — if the preparation contains V. cholerae, the field appears to show organisms shooting across like comets.
Immobilisation test (confirmatory on hanging-drop): If V. cholerae motility is observed, a drop of anti-O1 antiserum can be added to the edge of the coverslip — V. cholerae serogroup O1 (the epidemic strain) will be immobilised within seconds (agglutination). Strains not immobilised by O1 antiserum but immobilised by O139 antiserum are the Bengal serotype (both are epidemic cholera strains). Strains immobilised by neither are non-O1/non-O139 Vibrio (rarely cause epidemic cholera).
Interpretation and limitations:
- Positive darting motility in the clinical context of rice-water diarrhoea during an outbreak = presumptive V. cholerae — initiate outbreak response and treatment
- Send stool for culture on TCBS (thiosulfate-citrate-bile salts-sucrose) agar — V. cholerae grows as large yellow colonies (ferments sucrose, lowering pH, producing yellow colour on TCBS) within 24 hours. This confirms the diagnosis and provides an isolate for antibiotic sensitivity testing.
- Limitations: hanging-drop does not distinguish O1 from O139 cholera strains; other rapidly motile organisms can cause false positives; negative hanging-drop does not rule out V. cholerae (organisms may be dead if stool was refrigerated or delayed)
Gram stain of stool in cholera: V. cholerae appears as small, curved, comma-shaped Gram-negative rods — described as 'flock of seagulls' or 'school of fish' arrangement when many organisms are present. This is supportive but not diagnostic.
Hanging-Drop Preparation and V. cholerae Identification