Page 9 of 19
IM16.8-12 | Diarrheal Disorder Diagnostic Testing — SDL Guide (Part 2)
Indications for Stool and Blood Cultures in Acute Diarrhoea
Not every patient with acute diarrhoea requires stool culture. The majority of acute infectious diarrhoeal episodes resolve within 3–5 days without microbiological identification of the specific pathogen. Selective use of stool culture — guided by specific clinical indications — maximises diagnostic yield while conserving laboratory resources and avoiding unnecessary delays to empirical treatment in severe cases. This principle of selective culture is the content of IM16.11: knowing WHEN to order the culture, not how to perform it technically. In the absence of this selective discipline, laboratories become overwhelmed with low-yield cultures from self-limiting viral illnesses, antibiotics are started on the basis of culture results that were never needed, and the genuinely high-yield cultures — those from patients with invasive bacterial diarrhoea, suspected enteric fever, or immunocompromised states — are delayed or lost in the noise. Mastering the specific indications below gives you the ability to use the laboratory as a precision tool rather than a safety net.
Indications for stool culture in acute diarrhoea (order culture when one or more of the following are present):
- Dysentery (bloody mucoid stools) with fever: inflammatory/invasive diarrhoea requires identification of the specific pathogen (Shigella, Campylobacter, Salmonella, EIEC) for appropriate antibiotic choice, since resistance patterns vary and empirical treatment may need adjustment
- Moderate-to-severe diarrhoea that does not resolve in 7 days: persistence beyond the expected self-limiting course of viral gastroenteritis suggests a bacterial or parasitic cause that may benefit from targeted therapy
- Suspected outbreak (epidemiological importance): culture identifies the causative organism for public health response — the index case and subsequent cases in a common-source outbreak need stool cultures sent to the state referral laboratory
- Diarrhoea in hospitalised patients, especially post-antibiotic: Clostridioides difficile — specifically order C. diff toxin assay (EIA for toxins A and B, or NAAT/PCR) rather than routine bacterial culture; standard stool cultures do not detect C. diff
- Diarrhoea in immunocompromised patients (HIV, transplant, chemotherapy): the pathogen spectrum is different (Salmonella bacteraemia more common in HIV, opportunistic organisms) and culture results directly influence antibacterial choice
- Enteric fever (typhoid/paratyphoid) suspected: stool culture in the second and third week of typhoid has the highest yield (organisms appear in stool as the patient becomes a temporary carrier). In the first week, blood culture is more sensitive (bacteraemia phase). Widal test for agglutinating antibodies is available at most district hospitals but has significant false-positive rates in endemic India — it is supportive, not definitive.
- Travel to endemic cholera area with rice-water diarrhoea: stool culture on TCBS agar for V. cholerae; results inform outbreak control
Indications for blood culture:
- Enteric fever (Salmonella typhi or S. paratyphi): blood culture is the gold standard for diagnosis in the first week — the bacteraemic phase. Draw 2–3 sets of blood cultures (10–15 mL each, aerobic bottle) before initiating antibiotics. Sensitivity: ~70–85% in the first week, declining in subsequent weeks
- Invasive non-typhoidal Salmonella (NTS): NTS septicaemia is common in HIV-positive patients and in sickle cell disease — blood culture is essential
- Suspected bacteraemia in acute dysentery: Shigella bacteraemia rare but occurs in children and immunocompromised; Campylobacter bacteraemia
- Immunocompromised patients with fever and diarrhoea: bacteraemia with enteric Gram-negative organisms, MAC, candida — blood cultures essential alongside stool cultures
- Diarrhoea with systemic sepsis features (hypotension, altered sensorium): blood cultures mandatory before empirical antibiotic initiation
Tests NOT routinely needed for uncomplicated acute watery diarrhoea in a non-immunocompromised adult: stool culture (most will self-resolve), colonoscopy, serology, CT abdomen. The guiding principle is that the investigation should change management — and in self-limiting viral gastroenteritis, no investigation will change the recommendation of oral rehydration and supportive care.
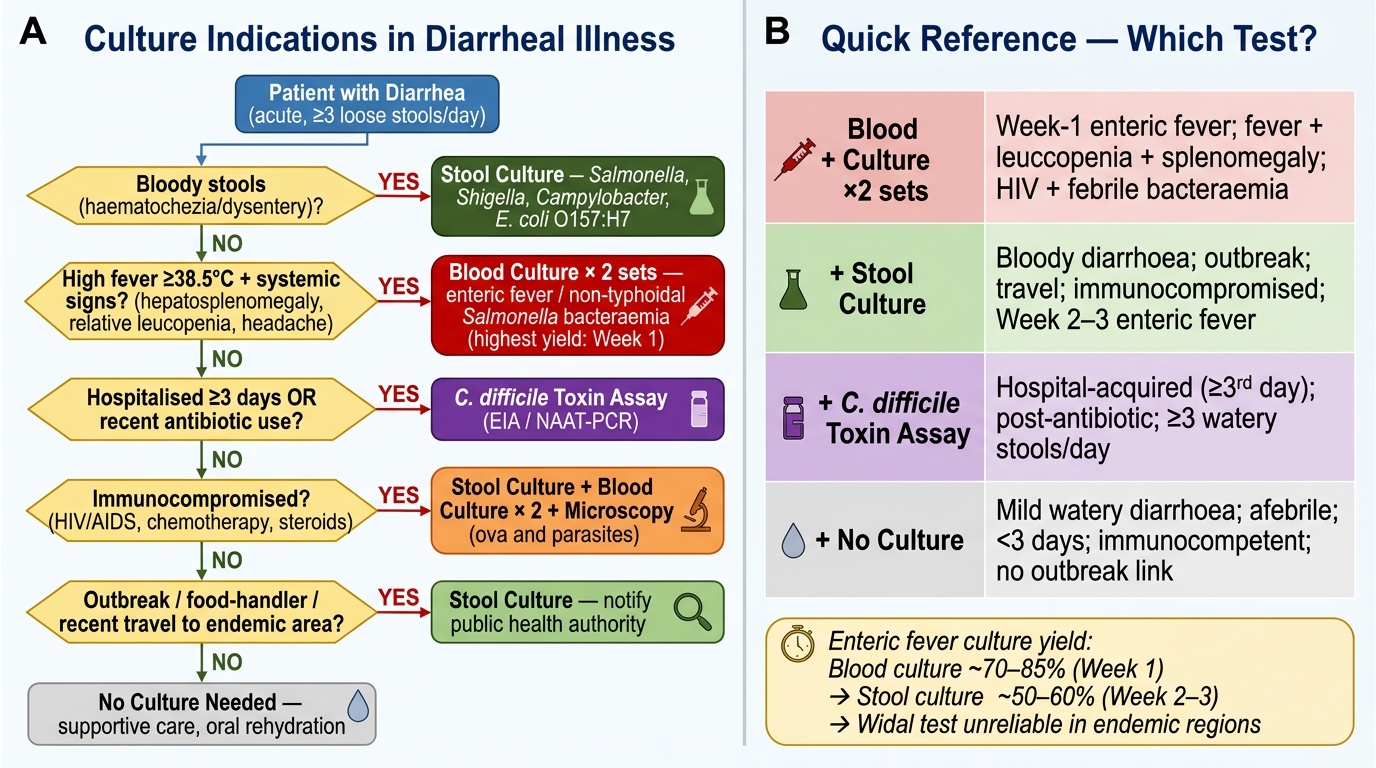
Culture Indications in Diarrheal Illness: Decision Flowchart
SELF-CHECK
A 35-year-old HIV-positive man (CD4 count 180 cells/μL, not on ART) presents with 3 days of high fever (39.5°C), headache, and four watery stools per day. He has hepatosplenomegaly on examination. White cell count is 3.1×10⁹/L (leucopenia). Which investigation has the HIGHEST diagnostic yield for his MOST LIKELY diagnosis at this stage?
A. Stool culture on TCBS agar
B. Stool examination for ova and parasites
C. Blood culture (two sets, aerobic bottles)
D. Widal test for Salmonella antibodies
Reveal Answer
Answer: C. Blood culture (two sets, aerobic bottles)
The clinical picture — high fever, relative leucopenia, hepatosplenomegaly, and watery diarrhoea — is classic for enteric fever (typhoid or paratyphoid). In the FIRST WEEK of enteric fever, the organism is in the bloodstream (bacteraemic phase) and blood culture has the highest sensitivity (~70–85%). The Widal test is unreliable in India due to background high seroprevalence in endemic areas and cross-reactivity — it is not the gold standard. Stool culture is highest yield in week 2–3. TCBS agar is for Vibrio cholerae; this is not a cholera presentation. Stool for O&P would detect parasites but not Salmonella. Additionally, in this HIV-positive patient, non-typhoidal Salmonella bacteraemia must be considered (common complication in HIV) — blood culture is essential.
Advanced Investigations for Chronic Diarrhoea: Indications and Interpretation
Chronic diarrhoea (>4 weeks) represents a diagnostic challenge that requires a systematic progression from non-invasive to invasive investigations, guided by the clinical differential diagnosis established from history and physical examination. The competency IM16.12 requires the student to enumerate and discuss the indications for advanced investigations in chronic diarrhoea — specifically serology, colonoscopy, diagnostic imaging, and biopsy. The key principle is that these investigations are not ordered in sequence simply because the patient has chronic diarrhoea; each one is ordered because the differential hypothesis at that point in the workup predicts a specific finding that would change management.
Serological investigations and their specific indications:
Coeliac disease serology: Indicated when chronic diarrhoea is accompanied by features of malabsorption (steatorrhoea, weight loss, multi-nutrient deficiency, iron-deficiency anaemia refractory to iron therapy). The first-line test is serum anti-tissue transglutaminase IgA (anti-tTG IgA) — sensitivity 97%, specificity >95% in patients with normal serum IgA. Because 2–5% of coeliac patients have IgA deficiency (which would give a falsely negative result), always check total serum IgA simultaneously. If total IgA is deficient, order anti-tTG IgG or deamidated gliadin peptide (DGP) IgG instead. A strongly positive anti-tTG IgA (>10× upper limit of normal) with typical clinical features may be sufficient for diagnosis in some guidelines; however, duodenal biopsy remains the gold standard confirming villous atrophy (Marsh classification: Marsh 3a–c = partial to total villous atrophy).
Serological markers for IBD:
- ASCA (anti-Saccharomyces cerevisiae antibodies) — more common in Crohn's disease
- ANCA (anti-neutrophil cytoplasmic antibodies, perinuclear pattern = p-ANCA) — more common in UC
- Faecal calprotectin: a faecal protein marker of intestinal inflammation — elevated in IBD, not elevated in IBS. Used to distinguish IBD from IBS non-invasively before colonoscopy, and to monitor IBD activity. A faecal calprotectin <50 µg/g effectively excludes significant IBD with high negative predictive value.
Serological tests for amoebiasis: Anti-amoebic antibodies (ELISA) are useful in amoebic liver abscess (positive in >90% of invasive amoebiasis) but less useful in intestinal amoebiasis alone. A positive serology does not distinguish active from past infection in endemic areas; it is most useful when stool microscopy is equivocal.
Colonoscopy — indications in chronic diarrhoea:
Colonoscopy with multiple biopsies is the most powerful diagnostic tool for chronic diarrhoea when the differential includes IBD, colorectal carcinoma, microscopic colitis, or infectious colitis not identified by stool examination. Specific indications:
- Rectal bleeding with chronic diarrhoea (any age, but mandatory >45 years): biopsy any mucosal abnormality or polyp; assess extent and pattern of inflammation
- Suspected UC: colonoscopy characterises the extent (proctitis, left-sided, extensive), scores disease activity, and guides treatment choice (local vs systemic therapy)
- Suspected Crohn's: ileocolonoscopy with terminal ileal intubation and biopsy — ulceration pattern (aphthous ulcers, cobblestone, skip lesions), biopsy for granulomas
- Suspected colorectal carcinoma: direct visualisation + biopsy for histological diagnosis; assessment of extent and synchronous lesions
- Suspected microscopic colitis (watery diarrhoea, normal colonoscopic appearance, typically in older women on NSAIDs or SSRIs): colonoscopy is macroscopically normal — diagnosis is made on biopsy (collagenous colitis: thickened subepithelial collagen band; lymphocytic colitis: increased intraepithelial lymphocytes)
- Chronic diarrhoea after exclusion of other causes: diagnostic colonoscopy with random biopsies to detect microscopic colitis or early IBD
Upper GI endoscopy and duodenal biopsy:
Indicated when small bowel malabsorption is suspected (coeliac disease, giardiasis, tropical sprue, Whipple's disease). Duodenal biopsy shows: villous architecture (normal vs atrophy), intraepithelial lymphocytosis, and specific features (periodic acid-Schiff positive macrophages in Whipple's disease). Capsule endoscopy is used for small bowel visualisation when capsule endoscopy is available and standard endoscopy is non-diagnostic.
Diagnostic imaging:
- CT enterography / CT enteroclysis: superior delineation of the small bowel for Crohn's disease extent, strictures, fistulae, and abscess. Also shows mesenteric lymphadenopathy (Crohn's, lymphoma, TB).
- Abdominal X-ray: limited in routine workup, but useful to detect toxic megacolon (transverse colon diameter >6 cm) in acute severe colitis — an indication for emergency surgical review
- Ultrasound: first-line for amoebic liver abscess (hypoechoic well-defined lesion, right lobe predominance), ascites (chronic malabsorptive states), and bowel wall thickening (IBD, tuberculosis)
- MRI enterography/MRI pelvis: perianal Crohn's disease (fistula tract mapping), pelvic IBD, and small bowel in patients where radiation exposure must be minimised (young patients, pregnancy)
- Technetium-99m white cell scan: delineates active IBD extent in patients who cannot tolerate colonoscopy; rarely used in routine practice in India
Faecal fat quantification (72-hour collection): When steatorrhoea is suspected clinically (pale, floating, foul-smelling stools) but serology is equivocal, a 72-hour faecal fat collection on a 100 g fat/day controlled diet quantifies fat malabsorption directly. Normal: <7 g/day. >14 g/day indicates significant fat malabsorption. Replaced in many centres by Sudan III stain on spot stool (rapid, less sensitive).
Hydrogen breath tests: Detect carbohydrate malabsorption (lactose, fructose) and small intestinal bacterial overgrowth (SIBO). After ingestion of substrate (lactose or lactulose), exhaled hydrogen is measured — a rise >20 ppm above baseline within 2 hours indicates malabsorption or bacterial fermentation in the small bowel.
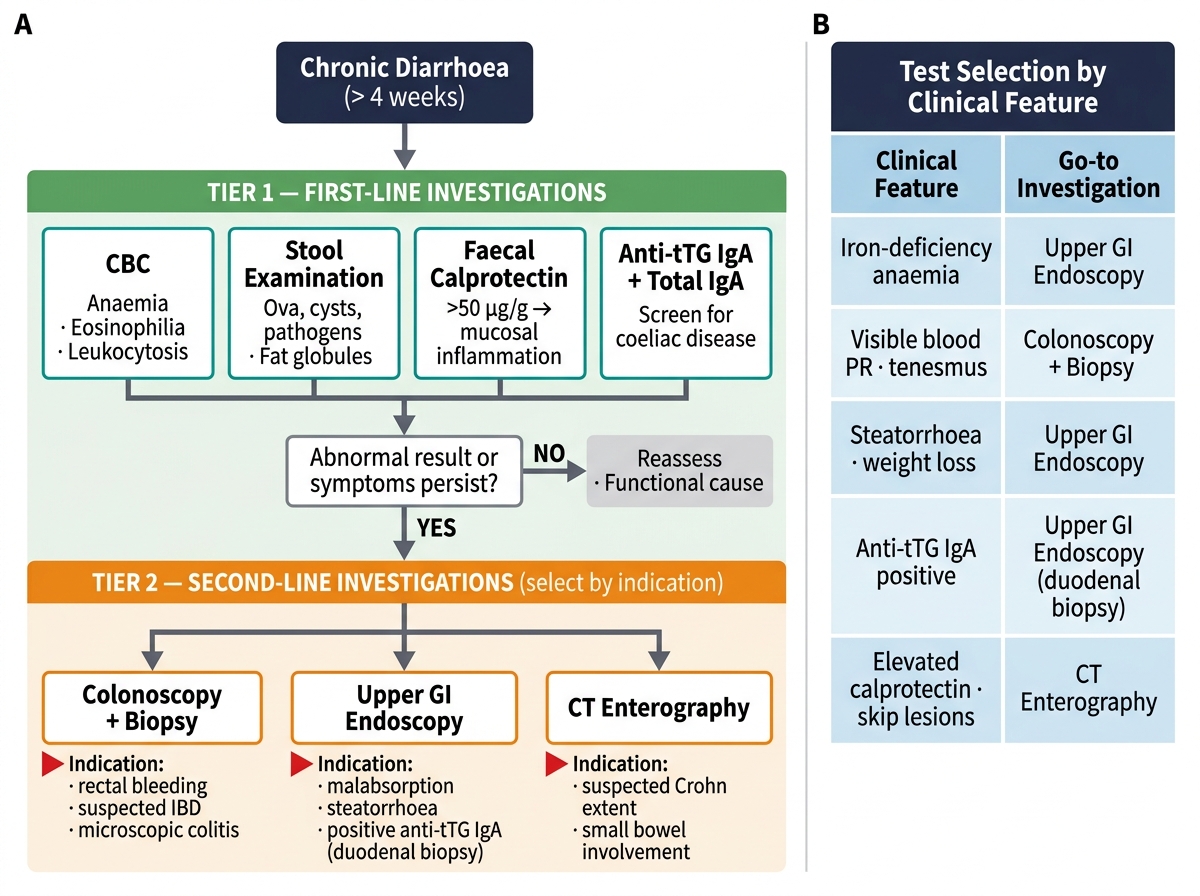
Tiered Investigation Algorithm for Chronic Diarrhoea
SELF-CHECK
A 31-year-old woman presents with a 5-month history of watery diarrhoea (6 stools/day), no blood, no fever, and 4 kg weight loss. She takes ibuprofen daily for chronic back pain. Colonoscopy is performed and appears macroscopically normal throughout the colon. Multiple biopsies are taken. The pathology report shows increased intraepithelial lymphocytes (>20 per 100 epithelial cells) and no thickened subepithelial collagen band. What is the diagnosis?
A. Collagenous colitis — thickened subepithelial collagen band >10 µm
B. Ulcerative colitis — crypt abscesses and goblet cell depletion
C. Lymphocytic colitis — normal macroscopic appearance with increased intraepithelial lymphocytes
D. Normal colon — no investigation required
Reveal Answer
Answer: C. Lymphocytic colitis — normal macroscopic appearance with increased intraepithelial lymphocytes
Microscopic colitis comprises two histological subtypes: collagenous colitis (thickened subepithelial collagen band >10 µm + intraepithelial lymphocytosis) and lymphocytic colitis (increased intraepithelial lymphocytes >20 per 100 epithelial cells WITHOUT thickened collagen). Both subtypes share the classic presentation: chronic watery non-bloody diarrhoea in middle-aged to older adults, macroscopically NORMAL colonoscopy, and diagnosis only on biopsy. Association with NSAIDs (ibuprofen in this patient) and SSRIs is well-documented. UC would show crypt abscesses, goblet cell depletion, and macroscopic mucosal changes. A macroscopically normal colonoscopy does not exclude pathology — biopsy is mandatory in chronic diarrhoea workup even with a normal-appearing colon.
Self-Assessment: Applying Diagnostic Investigation Principles
Apply the diagnostic investigation framework from this module to the following scenarios. For each, identify the key investigations in order of priority, their expected findings, and the diagnostic logic that selects them.
Scenario A: A 45-year-old man presents with 3 weeks of foul-smelling, floating, pale stools with abdominal bloating, and has lost 6 kg. He has angular stomatitis. His Hb is 9.5 g/dL (microcytic). He denies blood in stool and has no fever. What is the diagnostic pathway from first-line to definitive investigation?
Analysis: Malabsorption pattern — steatorrhoea, weight loss, iron-deficiency anaemia (microcytic Hb), angular stomatitis (B-vitamin deficiency). First-line: CBC (confirm anaemia pattern), anti-tTG IgA + total serum IgA (for coeliac), stool examination (excluding Giardia — cysts on iodine preparation, which can also cause malabsorption without blood). If anti-tTG IgA positive: upper GI endoscopy with duodenal biopsy (multiple biopsies from D2 — at least 4, per ESPGHAN protocol). Expect: villous atrophy (Marsh 3), increased intraepithelial lymphocytes, crypt hyperplasia. If anti-tTG negative and Giardia excluded: 72-hour faecal fat (confirm steatorrhoea quantitatively), then CT abdomen (pancreatic causes — chronic pancreatitis), and consider small bowel imaging for Crohn's ileitis.
Scenario B: A 62-year-old woman has had 3 months of watery diarrhoea (5 stools/day), no blood, no fever, and no weight loss. She had a coronary angioplasty 8 months ago and was started on clopidogrel and a statin; she also takes a PPI. Physical examination is entirely normal. CBC, CRP, and stool examination are all normal. What should be the next investigation, and what are the two most likely pathological diagnoses?
Analysis: Chronic watery diarrhoea with normal initial workup in an older patient on multiple medications — the two most likely diagnoses are microscopic colitis (associated with NSAIDs and SSRIs; PPI also associated; normal colonoscopy but abnormal biopsy) and drug-induced diarrhoea (statins, PPIs, clopidogrel all on the list of diarrhoea-causing drugs). First investigation: colonoscopy with multiple biopsies — even with normal macroscopic appearance, biopsy differentiates microscopic colitis (lymphocytic or collagenous) from normal colon. If biopsy normal: review medications systematically and consider a medication trial-off. Faecal calprotectin: elevated in microscopic colitis, distinguishing from pure drug-induced diarrhoea and IBS.
Scenario C: A 26-year-old backpacker returns from 4 weeks in Nepal. She has had gassy, bloating, and foul-smelling loose non-bloody stools for 6 weeks. She denies fever. Standard stool examination ×1 shows no parasites. What is the most likely diagnosis, and what should be done next?
Analysis: Post-travel malabsorptive diarrhoea with bloating and flatulence for 6 weeks — giardiasis is the most likely diagnosis. Giardia cysts are intermittently excreted; a single stool examination has only ~70% sensitivity. Order three separate stool examinations on three different days (cyst examination with iodine preparation); sensitivity of three samples ~90%. If still negative but strong clinical suspicion: duodenal aspirate (passed via upper GI endoscopy — trophozoites at higher density in proximal small bowel; sensitivity ~90% on single aspirate) or giardia antigen ELISA (stool antigen detection — sensitivity >90%, useful where available). Empirical metronidazole can be considered if serially negative but clinical picture is compelling.
CLINICAL PEARL
The most diagnostically damaging error in stool microscopy for amoebiasis is examining a refrigerated, old, or delayed specimen for trophozoites. Entamoeba histolytica trophozoites lyse rapidly on cooling — if the specimen is not examined within 30 minutes of collection, trophozoites are absent. Students and clinicians who receive a 'negative for E. histolytica' result on a 2-hour-old stool sample cannot exclude amoebiasis — they have only excluded motile trophozoites in a viable specimen. The correct protocol: collect the sample in a warm container, transport immediately to the laboratory, and examine within 30 minutes. For cyst detection (carrier state, formed stool), timing is less critical.
A second pearl: colonoscopy with a macroscopically normal appearance does NOT exclude colonic pathology. Microscopic colitis — a common cause of watery diarrhoea in older adults on NSAIDs or SSRIs — appears completely normal on colonoscopy. The diagnosis is made exclusively on biopsy. Never report 'colonoscopy normal — no further investigation needed' in a patient with unexplained chronic watery diarrhoea without taking multiple biopsies from throughout the colon.