Page 11 of 19
IM16.{13-14,16-17} | Diarrheal Disorder Treatment — SDL Guide
Learning Objectives
- Describe the universal treatment framework for diarrhoeal disease — dehydration assessment first, then aetiology-specific pharmacotherapy — and apply WHO Plan A/B/C rehydration protocols
- Describe and enumerate the indications, pharmacology, and side effects of pharmacotherapy for parasitic diarrhoea including the mandatory two-drug protocol for amoebiasis (metronidazole + diloxanide furoate)
- Describe and enumerate the indications, pharmacology, and side effects of antibiotics for bacterial diarrhoea — including the correct agents for Shigella (ciprofloxacin), cholera (doxycycline/azithromycin), and C. difficile (metronidazole/vancomycin) — and explain why viral gastroenteritis requires no antibiotic
- Describe the step-up pharmacological treatment of IBD including 5-ASA, corticosteroids, immunomodulators (azathioprine/6-MP), and biological agents (anti-TNF, vedolizumab, ustekinumab), including mandatory pre-biologic TB screening
- Enumerate the indications for surgery in UC (toxic megacolon, perforation, refractory disease, high-grade dysplasia) and CD (stricture, fistula, abscess, perforation) and distinguish the curative potential of surgery in UC from its palliative/complication-management role in CD
INSTRUCTIONS
This module develops treatment decision-making in diarrhoeal disorders — from acute rehydration through anti-parasitic drug protocols to biologic therapy in IBD and surgical timing. Apply the treatment ladder actively: for each drug mentioned, know its mechanism, its side effects, its contraindications, and whether it requires a follow-on drug to be complete.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 43 — Diarrhoea and Constipation; Ch. 331 — Inflammatory Bowel Disease (textbook)
- API Textbook of Medicine, 10th ed., Ch. 7 — Gastroenterology (textbook)
- Davidson's Principles & Practice of Medicine, 24th ed., Ch. 24 — Alimentary Tract (textbook)
- ECCO Guidelines on UC Management, 2022 (guideline)
- ECCO Guidelines on Crohn's Disease Management, 2022 (guideline)
- WHO Guidelines for the Control of Cholera, 2017 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old man is brought to the emergency department with 12 hours of profuse watery diarrhoea. He has passed approximately 8 litres of rice-water stools since midnight during a cholera outbreak at a college hostel. His BP is 80/50 mmHg lying down, pulse 130/min and thready, eyes are sunken, skin pinch recoils in more than 2 seconds, and he cannot drink because of persistent vomiting. In this patient, the first treatment decision is not about which antibiotic to use — it is a race against hypovolaemic shock. Within the same shift, a 38-year-old woman presents requesting a prescription for metronidazole for her 'amoeba tablets' — she has watery stools for 2 days after a food-stall meal, no blood, no fever, and looks well. She wants antibiotics. Both presentations are infectious diarrhoea, but one demands immediate parenteral fluid resuscitation and targeted antibiotics, while the other requires only reassurance, oral rehydration, and no antibiotics whatsoever. Treatment in diarrhoeal disorders is not a single protocol — it is a layered decision framework that begins with severity assessment and builds outward to aetiology-specific therapy.
WHY THIS MATTERS
IM16.13 covers the pharmacotherapy of parasitic diarrhoea — indications, pharmacology, and side effects of anti-parasitic agents. IM16.14 covers the pharmacotherapy of bacterial and viral diarrhoea. IM16.16 covers treatment of chronic diarrhoea, including immunotherapy (biologics in IBD). IM16.17 specifically addresses the surgical indications in inflammatory bowel disease. These competencies are at the Knowledge with Application (KH) level — you must not only name the drugs but apply them correctly to a clinical scenario, know their side effects, and understand why some drugs are contraindicated in specific settings. The final-year student must be prepared to counsel a patient on oral rehydration therapy in a primary health centre, to select the correct antibiotic for bacterial dysentery in a district hospital, and to recognise when a patient with IBD needs surgical consultation rather than further medical therapy.
RECALL
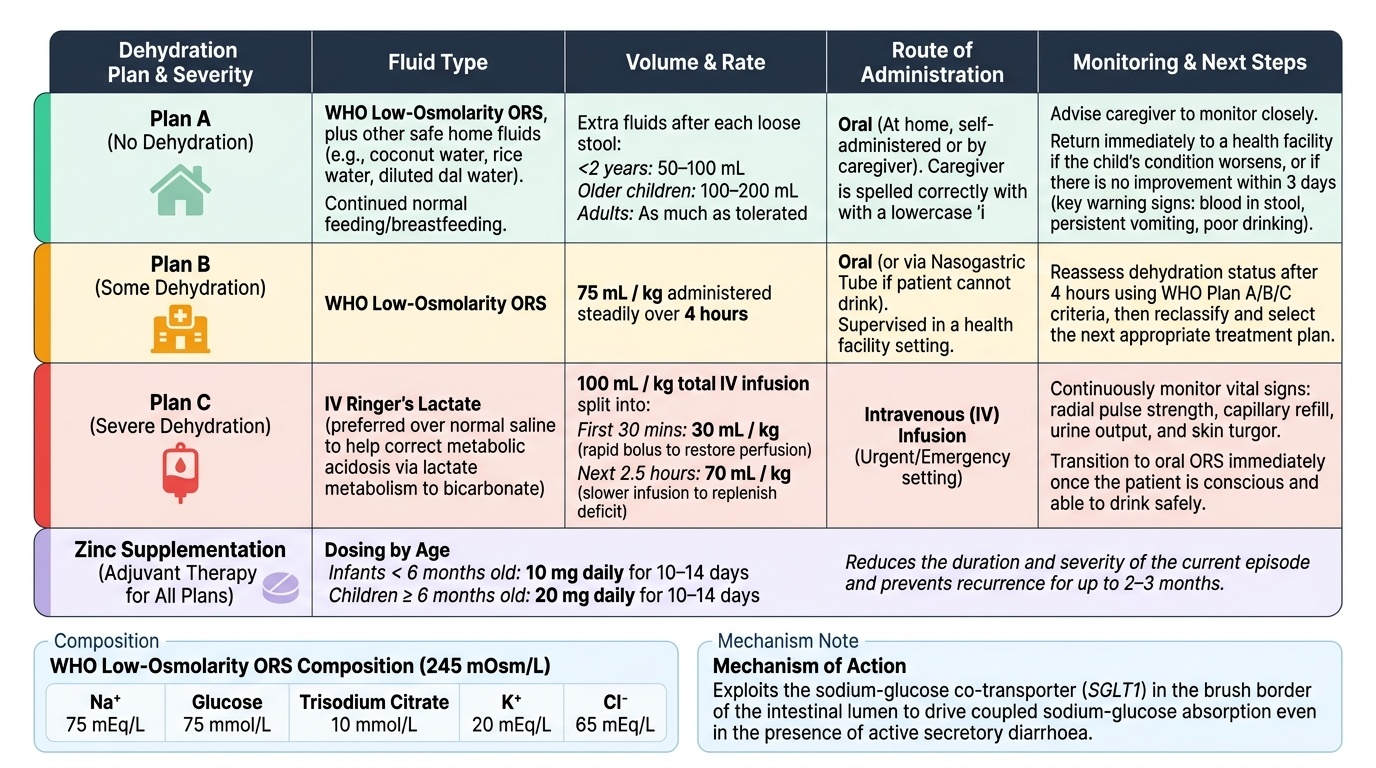
From the Foundations SDL, recall: WHO ORS composition — 245 mOsm/L total; Na 75, glucose 75, K 20, Cl 65, citrate 10 (mEq/L or mmol/L as appropriate). WHO Plan A = ORS at home; Plan B = 75 mL/kg over 4 hours supervised; Plan C = IV Ringer's Lactate 100 mL/kg (30 mL/kg over 30 min + 70 mL/kg over 2.5 hr). From your Pharmacology training: metronidazole is a 5-nitroimidazole that requires activation in anaerobic organisms; ciprofloxacin is a fluoroquinolone (DNA gyrase + topoisomerase IV inhibitor); azithromycin is a macrolide (50S ribosomal inhibitor). From the Diagnostics SDL: recall that antimotility agents are contraindicated in dysentery and invasive infection. These pharmacological foundations are the starting point for the treatment decisions in this module.
Clinical Presentation and Rehydration: The Universal First Step
Regardless of aetiology, the treatment of diarrhoeal disease begins with the same universal first principle: assess and correct dehydration. No antibiotic, anti-parasitic, or anti-inflammatory agent can be effective in a patient who is haemodynamically compromised from volume depletion — and in secretory diarrhoea (particularly cholera), the fluid loss itself is the primary life threat, not the organism. The decision sequence in treatment therefore always runs: (1) assess dehydration severity using WHO Plan A/B/C criteria, (2) initiate rehydration at the appropriate route and rate, (3) then and only then layer aetiology-specific pharmacotherapy on top of the rehydration scaffold. Reversing this order — giving antibiotics before addressing dehydration in a shocked patient — represents a dangerous clinical error.
Provided image
Oral Rehydration Therapy (ORT) is one of the most cost-effective medical interventions ever developed and the cornerstone of diarrhoea management globally. The WHO low-osmolarity ORS (245 mOsm/L) — containing Na 75 mEq/L, glucose 75 mmol/L, K 20 mEq/L, Cl 65 mEq/L, and trisodium citrate 10 mmol/L — exploits the sodium-glucose co-transporter (SGLT1) mechanism to drive coupled sodium-glucose absorption even in the presence of active secretion. ORS reduces all-cause diarrhoeal mortality and reduces the need for unscheduled IV therapy. For Plan A (no dehydration): advise the caregiver to give extra fluids at home — ORS plus other safe fluids (coconut water, rice water, diluted dal water), continue normal feeding, and return immediately if the child's condition worsens or if there is no improvement in 3 days. For Plan B (some dehydration): provide 75 mL/kg of WHO ORS over 4 hours in a supervised health facility setting; after 4 hours, reassess dehydration status and reclassify.
For Plan C (severe dehydration): immediately initiate IV Ringer's Lactate (preferred over normal saline because it contains lactate which is metabolised to bicarbonate, helping correct the metabolic acidosis of severe diarrhoea). Regimen: 30 mL/kg in 30 minutes (rapid bolus to restore perfusion), then 70 mL/kg in 2.5 hours (slower infusion to replenish remaining deficit). Monitor response — radial pulse strength, capillary refill, urine output, skin turgor. Once the patient can drink, transition to ORS to complete rehydration. Electrolyte monitoring: serum Na, K, bicarbonate, and creatinine at baseline and after initial resuscitation. Hypokalaemia (from stool potassium loss) must be corrected — add potassium chloride to IV fluid or start oral potassium supplementation as soon as the patient can drink.
Zinc supplementation in children under 5 with acute diarrhoea: 20 mg/day for 10–14 days (10 mg for infants <6 months) — a WHO/UNICEF recommendation shown to reduce diarrhoea duration and severity, reduce diarrhoea recurrence in the following 2–3 months, and reduce all-cause under-5 mortality. Mechanism: zinc is a cofactor for intestinal metalloproteases involved in mucosal repair; deficiency (endemic in India) impairs epithelial regeneration.
Feeding during diarrhoea: Continue age-appropriate feeding throughout. The old practice of bowel rest ('starvation for 24–48 hours') is not only unsupported by evidence but harmful — fasting delays intestinal mucosal healing, worsens nutritional deficit, and prolongs the illness. In breastfed infants, breastfeeding should be continued without interruption. In older children and adults, a normal diet (avoiding high-fat, high-sugar foods that osmotically worsen diarrhoea) is recommended throughout the illness.
Pathophysiology of Infection and Antibiotic Principles in Diarrhoeal Disease
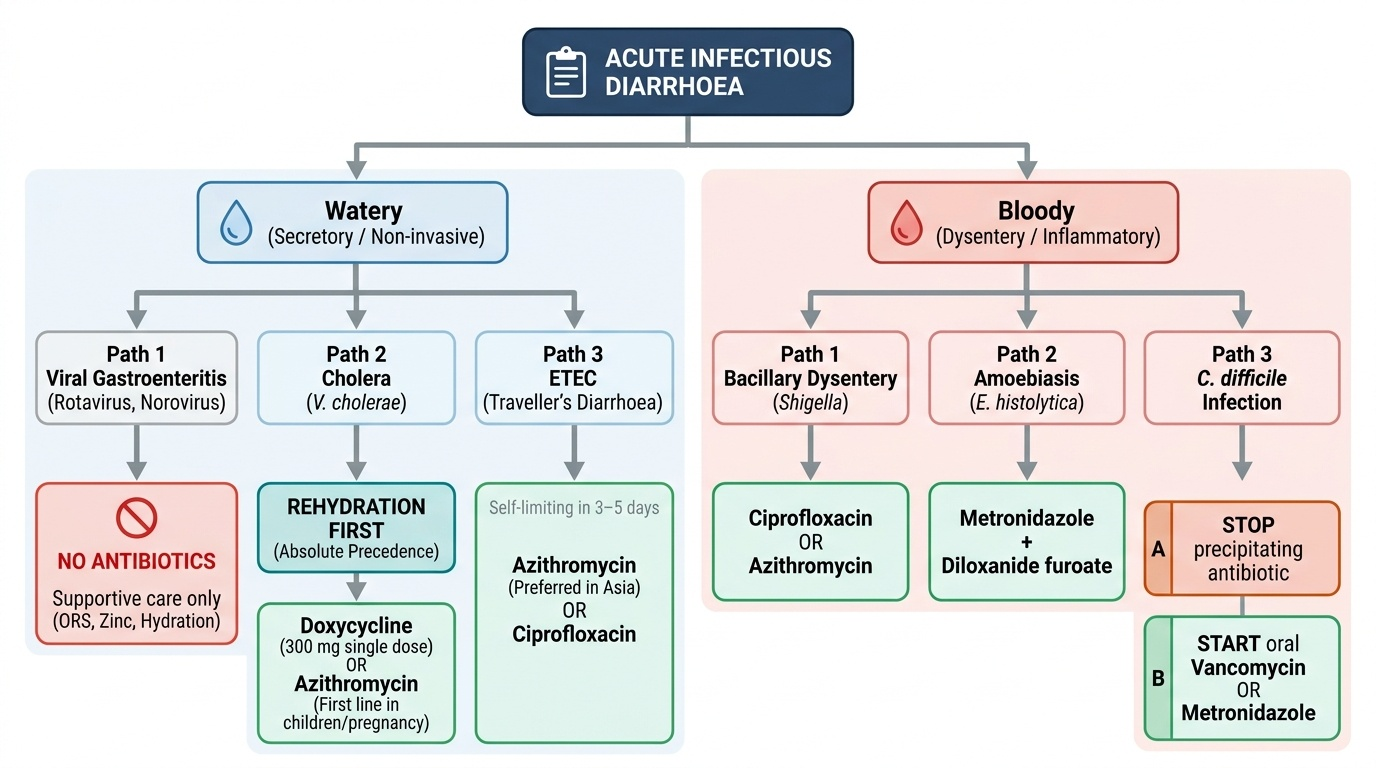
The pathophysiology of infectious diarrhoea divides cleanly into two mechanistic groups that determine the role of antibiotics: toxin-mediated secretory diarrhoea (where the pathogen produces an exotoxin but does not invade the mucosa — antibiotics reduce toxin production and shorten illness but are not essential for survival), and invasive/inflammatory diarrhoea (where the pathogen invades the mucosa or produces cytotoxins that damage the colonic epithelium — antibiotics shorten illness, reduce bacteraemia risk, and in some pathogens, prevent systemic complications). This pathophysiological distinction is the intellectual basis for the antibiotic prescribing decision in every infectious diarrhoeal presentation. The clinician who understands this does not need to memorise a list of 'infections that need antibiotics' — they can derive the answer from mechanism.
Provided image
Toxin-mediated, non-invasive infections — antibiotics used adjunctively (not primary treatment):
- Cholera (V. cholerae): rehydration is primary and life-saving; antibiotic is adjunctive. Oral doxycycline 300 mg single dose in adults shortens illness by 1–2 days and reduces stool output (V5 cholerae toxin production continues until the organism is eliminated). Alternatives: azithromycin 1 g single dose (first choice in pregnancy and children); ciprofloxacin (if susceptibility known). Note: V. cholerae resistance to tetracyclines and fluoroquinolones is increasing; current national surveillance guides empirical choice. Antibiotic is NEVER given before or instead of rehydration — rehydration takes absolute precedence.
- ETEC (traveller's diarrhoea): self-limiting in 3–5 days in immunocompetent adults; antibiotics shorten duration. Empirical azithromycin 500 mg once daily × 3 days (preferred in Asia due to fluoroquinolone-resistant ETEC) or ciprofloxacin 500 mg BD × 3 days (in regions with lower fluoroquinolone resistance). Prophylactic antibiotics for travel are NOT routinely recommended.
- Viral gastroenteritis (rotavirus, norovirus): NO ANTIBIOTICS. Treatment is purely supportive — ORS, continued feeding, zinc (children). Antibiotics have no role and add unnecessary adverse effects and resistance pressure.
Invasive/inflammatory infections — antibiotics are indicated:
- Shigella dysentery: empirical ciprofloxacin 500 mg twice daily × 3–5 days (adults); or azithromycin 500 mg daily × 3 days (children, or where fluoroquinolone resistance is documented). Ampicillin and co-trimoxazole have high resistance rates in India — do NOT use empirically. The rationale: Shigella invades colonic epithelial cells; antibiotics reduce the duration of illness, shorten infectivity, and decrease the risk of systemic complications (HUS from Shiga toxin in S. dysenteriae type 1, reactive arthritis)
- Campylobacter: usually self-limiting; antibiotics indicated for severe disease (high fever, bloody stools, systemic illness). Azithromycin 500 mg daily × 3 days — use azithromycin over ciprofloxacin (high fluoroquinolone resistance in Campylobacter). Rarely needs IV treatment
- Non-typhoidal Salmonella: most uncomplicated cases are self-limiting — antibiotics are NOT routinely recommended (they may prolong carriage). Antibiotic indications: age <12 months or >50 years, immunocompromised (HIV, chemotherapy, transplant), sickle cell disease, valvular heart disease, severe illness, or suspected bacteraemia. Drug of choice: ciprofloxacin 500 mg BD × 5–7 days; or azithromycin as alternative
- C. difficile: stop the precipitating antibiotic if possible; oral metronidazole 400 mg TDS × 10 days (mild-moderate disease); oral vancomycin 125 mg four times daily × 10 days (severe disease or relapse). Fidaxomicin (if available) for recurrent C. diff.
SELF-CHECK
A 16-year-old girl presents with 2 days of fever (38.8°C), mucoid bloody stools (8 stools per day), tenesmus, and left lower quadrant abdominal cramps following a school picnic. There is an ongoing outbreak of dysentery in her school. You suspect Shigella. What is the MOST APPROPRIATE antibiotic choice in India, and what is the rationale for avoiding the drug class that was previously first-line?
A. Ampicillin 500 mg every 6 hours × 5 days; it is the most cost-effective regimen
B. Co-trimoxazole (trimethoprim-sulfamethoxazole) DS twice daily × 5 days; it covers Gram-negative enteric organisms
C. Ciprofloxacin 500 mg twice daily × 3–5 days; ampicillin and co-trimoxazole have high resistance rates in India
D. Metronidazole 400 mg three times daily × 5 days; it covers both Shigella and E. histolytica
Reveal Answer
Answer: C. Ciprofloxacin 500 mg twice daily × 3–5 days; ampicillin and co-trimoxazole have high resistance rates in India
For Shigella dysentery in India, the current recommended antibiotic is ciprofloxacin (or azithromycin as an alternative). Ampicillin and co-trimoxazole (both previously first-line agents for Shigella) have unacceptably high resistance rates in India and should not be used empirically. Ciprofloxacin has maintained better activity, though fluoroquinolone resistance is increasing — azithromycin is the preferred choice in children and when fluoroquinolone resistance is suspected. Metronidazole has no activity against Shigella; it is the drug of choice for amoebiasis and anaerobic infections, not invasive bacterial dysentery. The two entities (Shigella vs E. histolytica) often need to be distinguished before committing to treatment, as metronidazole would treat amoebiasis but not Shigella.
Targeted Investigation to Guide Treatment Selection
Before pharmacotherapy is selected, the clinician must have sufficient diagnostic information to choose the correct treatment, avoid contraindicated therapies, and not delay treatment in emergencies. In diarrhoeal disease, the investigation burden before starting treatment is deliberately lean for acute presentations — because most high-morbidity decisions (rehydration plan, antibiotic for dysentery) are made on clinical grounds and must not be delayed for laboratory confirmation. However, the investigation results available at the time of treatment initiation directly determine whether aetiology-specific pharmacotherapy is appropriate, whether empirical therapy needs to be modified, and whether a contraindicated drug class (antimotility agents in dysentery, or biologics without TB exclusion in IBD) is being considered. This section covers the key diagnostic-to-treatment linkages: what you need to confirm before prescribing, and what result triggers which pharmacological decision in Indian clinical practice where time and resources must be used precisely.
Provided image
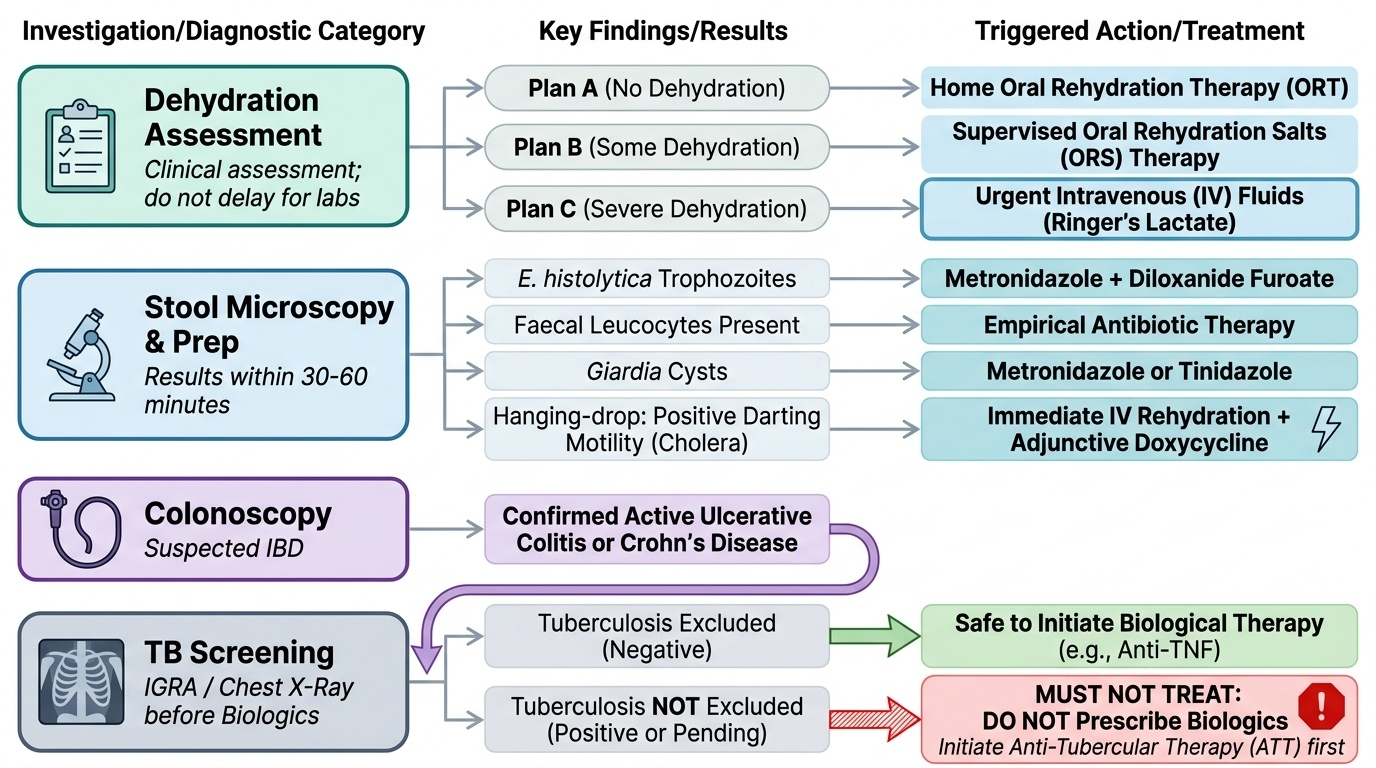
For acute infectious diarrhoea, the critical pre-treatment investigations are:
- Dehydration assessment (clinical — not laboratory): determines whether treatment is Plan A, B, or C. This is the first decision point.
- Stool microscopy (saline wet preparation + iodine): identifies E. histolytica trophozoites (triggers metronidazole + diloxanide furoate), faecal leucocytes (confirms invasive mechanism — antibiotic indicated), Giardia cysts (triggers metronidazole/tinidazole). Available within 30–60 minutes.
- Hanging-drop preparation (cholera suspected): positive darting motility → initiate IV rehydration immediately + adjunctive doxycycline
- Blood culture (enteric fever week 1): positive → targeted antibiotic; negative → treat empirically if clinical picture fits
- Acute watery non-bloody diarrhoea without fever: no investigation needed before starting ORS
For chronic diarrhoea, investigation results directly determine pharmacological choice: positive anti-tTG IgA + villous atrophy on duodenal biopsy → gluten-free diet (no drug); colonoscopy showing UC → 5-ASA; Crohn confirmed → limited 5-ASA, steroids; biologic initiation requires TB screening results (Mantoux, IGRA, CXR) reviewed before first infusion. In India, Crohn vs intestinal TB distinction must be resolved before immunosuppression — starting infliximab in undiagnosed TB is life-threatening.