Page 12 of 19
IM16.{13-14,16-17} | Diarrheal Disorder Treatment — SDL Guide (Part 2)
Pharmacotherapy of Parasitic Diarrhoea
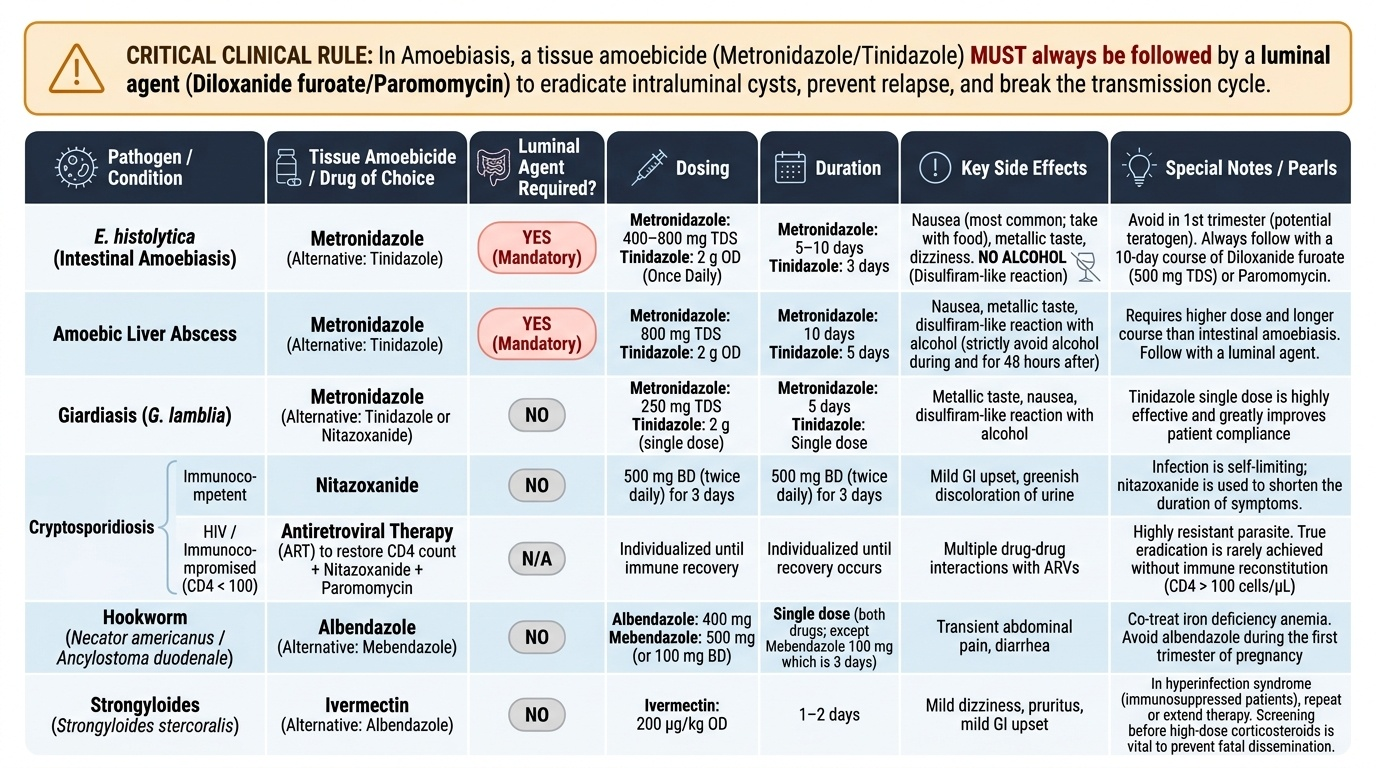
Parasitic infections of the gastrointestinal tract are a major cause of diarrhoeal morbidity in India, and their pharmacotherapy requires understanding not just which drug to use, but the rationale for the dose, the duration, the need for a luminal agent after a tissue agent, and the clinically important side effects that must be discussed with the patient. Each parasitic cause has a specific treatment algorithm, and errors in these algorithms — particularly the failure to follow metronidazole with a luminal agent in amoebiasis — are a commonly tested and clinically important knowledge gap.
Provided image
Amoebiasis (Entamoeba histolytica) — two-drug sequential protocol:
The treatment of intestinal amoebiasis and amoebic liver abscess requires a tissue amoebicide (to kill invasive trophozoites in the bowel wall and liver) followed by a luminal amoebicide (to eradicate intraluminal cysts and prevent relapse or transmission):
Tissue amoebicide:
- Metronidazole 400–800 mg three times daily × 5–10 days (oral) for intestinal amoebiasis; 800 mg TDS × 10 days for amoebic liver abscess. Mechanism: metronidazole is a 5-nitroimidazole; in anaerobic/microaerophilic organisms, it is reduced to a nitroso radical that binds DNA and causes strand breaks. Well-absorbed orally, excellent tissue penetration. Side effects: nausea (most common; advise to take with food), metallic taste, dizziness; potentially teratogenic (avoid in first trimester of pregnancy); disulfiram-like reaction with alcohol — must strictly advise alcohol abstinence during and for 48 hours after completion.
- Alternative: Tinidazole 2 g once daily × 3 days (intestinal amoebiasis) or 2 g OD × 5 days (amoebic liver abscess) — better tolerated than metronidazole (lower rates of nausea), single daily dose improves compliance.
Luminal amoebicide (mandatory to follow tissue treatment):
- Diloxanide furoate 500 mg three times daily × 10 days — acts in the gut lumen, eliminating cysts that metronidazole does not reach at effective concentrations. Side effects: flatulence, nausea, urticaria (rare). Not absorbed systemically — well tolerated. Mandatory after every course of metronidazole for amoebiasis to prevent relapse and break the transmission cycle.
- Alternatives: Paromomycin (aminoglycoside; minimally absorbed; can be used in pregnancy as luminal agent).
Note: Asymptomatic cyst passers (found on stool examination without symptoms) should also receive a luminal amoebicide (diloxanide furoate) to break transmission, as they serve as a reservoir for spread in households and communities.
Giardiasis:
- Metronidazole 400 mg three times daily × 5–7 days — first-line in most settings. Same mechanism as for amoebiasis. Efficacy ~80–95%. Same side effects as above.
- Tinidazole 2 g single dose — superior convenience; efficacy comparable; often preferred for compliance. May be used in children (50 mg/kg single dose, max 2 g).
- Albendazole 400 mg daily × 5 days — alternative; useful in mixed helminthic + giardia infections.
- Nitazoxanide — an alternative when metronidazole/tinidazole resistance is suspected or in immunocompromised patients.
Cryptosporidiosis:
- In immunocompetent adults: self-limiting; supportive treatment (ORS) only; no antiparasitic needed in most cases.
- In HIV/AIDS (CD4 <200): nitazoxanide 500 mg twice daily × 3 days (limited efficacy); ART initiation is the primary treatment — immune reconstitution (CD4 rise to >100 cells/μL) is the most effective intervention; without immune recovery, no antiparasitic provides lasting benefit.
Helminthic infections causing diarrhoea:
- Hookworm (Ancylostoma duodenale): albendazole 400 mg single dose (standard treatment; well-tolerated; minimal systemic absorption). Alternative: mebendazole 100 mg twice daily × 3 days. Also treat associated iron-deficiency anaemia.
- Strongyloides (especially risk of hyperinfection in immunocompromised): ivermectin 200 µg/kg/day × 2 days — drug of choice. Alternative: albendazole 400 mg twice daily × 7 days. Strongyloides requires higher doses and longer treatment than hookworm due to risk of autoinfection cycle.
- Giardia co-infection with helminths: combination treatment with albendazole (covers both giardia + helminths in a single course).
SELF-CHECK
A 32-year-old man is treated with metronidazole 800 mg three times daily for 10 days for amoebic liver abscess. His fever resolves and follow-up ultrasound at 4 weeks shows the abscess has decreased in size. He is asymptomatic. What is the MOST IMPORTANT next step in management, and why?
A. Start a second course of metronidazole at lower dose to prevent relapse
B. Begin diloxanide furoate 500 mg three times daily for 10 days as a luminal amoebicide
C. Order a repeat stool examination to confirm cyst clearance before discharging
D. No further treatment is needed as the liver abscess has responded to metronidazole
Reveal Answer
Answer: B. Begin diloxanide furoate 500 mg three times daily for 10 days as a luminal amoebicide
Metronidazole is a tissue amoebicide — it kills invasive trophozoites in the bowel wall and liver. However, it does not achieve effective luminal concentrations to eradicate intraluminal cysts. If a luminal amoebicide is not added, intraluminal cysts persist and can: (a) cause relapse of invasive amoebiasis, and (b) be passed in stool, transmitting E. histolytica to household contacts. Diloxanide furoate 500 mg TDS × 10 days is the standard luminal amoebicide given after every course of metronidazole for both intestinal and hepatic amoebiasis. A second course of metronidazole would not address the intraluminal cyst reservoir. Repeat stool examination is useful but does not substitute for the luminal drug; cyst persistence is expected until diloxanide treatment is completed.
Pharmacotherapy of Chronic Diarrhoea Including Immunotherapy in IBD
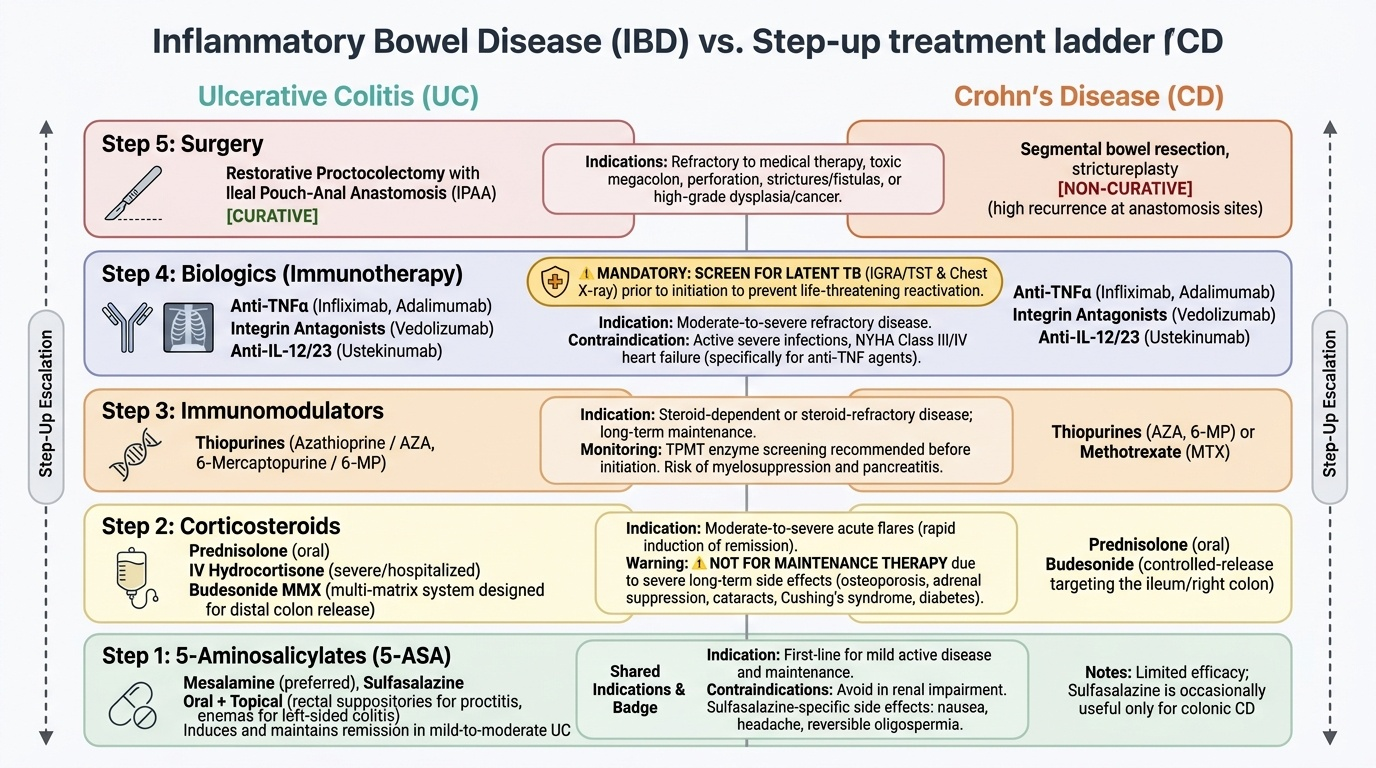
Chronic diarrhoea from non-infectious causes — particularly inflammatory bowel disease — requires a structured pharmacological approach that proceeds through a step-up treatment ladder from anti-inflammatory agents to immunomodulators to biological therapy (immunotherapy), with surgery reserved for refractory disease or life-threatening complications. The competency IM16.16 specifically includes immunotherapy, making knowledge of biological agents (monoclonal antibodies) in IBD a final-year requirement. Additionally, treatment of malabsorptive states (coeliac disease, tropical sprue) and functional disorders (IBS) is covered here.
Provided image
Ulcerative Colitis (UC) — pharmacological step-up:
Step 1 — Aminosalicylates (5-ASA, mesalamine): First-line for mild-to-moderate UC. These drugs reduce mucosal inflammation by inhibiting prostaglandin synthesis, lipoxygenase pathway, and NF-κB, and by reducing reactive oxygen species in the colonic mucosa. Formulations: sulfasalazine (5-ASA linked to sulfapyridine by an azo bond — the sulfapyridine moiety is responsible for most side effects: nausea, headache, oligospermia, haemolytic anaemia, skin rash); mesalamine (5-ASA alone — fewer systemic side effects; preferred). Route: oral + topical (rectal suppository for proctitis; enema for left-sided UC). Efficacy: induces and maintains remission in mild-moderate UC.
Step 2 — Corticosteroids: For moderate-to-severe flares not responding to aminosalicylates. Prednisolone 40–60 mg/day oral for active disease (taper over 8–12 weeks once remission achieved). IV hydrocortisone 100 mg every 6–8 hours or IV methylprednisolone 60 mg/day for severe UC requiring hospitalisation. Corticosteroids are not used for maintenance — they have unacceptable long-term side effects (adrenal suppression, osteoporosis, Cushing syndrome, diabetes, cataracts, infection susceptibility). Budesonide MMX (ileal/right-colon release formulation) for distal disease with lower systemic absorption.
Step 3 — Immunomodulators: For steroid-dependent or steroid-refractory UC. Azathioprine 2–2.5 mg/kg/day or 6-mercaptopurine (6-MP) 1–1.5 mg/kg/day — thiopurine drugs that inhibit purine synthesis and lymphocyte proliferation. Monitor CBC regularly (bone marrow suppression risk); check TPMT (thiopurine methyltransferase) enzyme activity before starting (TPMT-deficient patients metabolise azathioprine differently, risking severe myelosuppression). Latent TB screening mandatory before starting (India: Mantoux + IGRA + chest X-ray). Side effects: nausea (especially at initiation), hepatotoxicity, pancreatitis, lymphoma risk (with prolonged use).
Step 4 — Biological agents (immunotherapy — IM16.16): For moderate-to-severe UC refractory to corticosteroids and immunomodulators.
- Anti-TNF-α agents: Infliximab (chimeric IgG1 monoclonal antibody; given by IV infusion at 0, 2, 6 weeks induction then every 8 weeks maintenance; 5 mg/kg per dose) and Adalimumab (fully humanised; subcutaneous injection; 160 mg → 80 mg → 40 mg every other week). Mechanism: bind and neutralise tumour necrosis factor alpha (TNF-α), a pro-inflammatory cytokine central to both UC and Crohn's inflammation. Side effects: increased risk of serious infections (including TB reactivation — MANDATORY TB screening before starting), risk of lymphoma (HSTCL — hepatosplenic T-cell lymphoma with combination thiopurine use), infusion reactions (infliximab), injection site reactions (adalimumab), demyelinating disease (rare).
- Anti-integrin agents: Vedolizumab (gut-selective; blocks α4β7 integrin, preventing lymphocyte trafficking to the gut; less systemic immunosuppression; preferred in older patients or those with high infection risk)
- Anti-IL-12/23 agents: Ustekinumab (blocks p40 subunit common to IL-12 and IL-23; used in CD and UC refractory to anti-TNF)
- JAK inhibitors: Tofacitinib (oral; JAK 1/3 inhibitor; approved for moderate-severe UC; risk of herpes zoster reactivation, VTE)
Crohn's Disease (CD) — pharmacotherapy:
Similar step-up ladder but with some differences: aminosalicylates have limited efficacy in CD (especially small bowel CD). Corticosteroids for active flares (budesonide preferred for ileocaecal CD due to lower systemic effects). Azathioprine/6-MP for maintenance. Metronidazole and ciprofloxacin for perianal fistulae and perianal disease. Anti-TNF agents (infliximab, adalimumab) are particularly effective for fistulising Crohn's — infliximab has the strongest evidence for fistula closure. Vedolizumab and ustekinumab for anti-TNF failure.
Coeliac disease: Strict, lifelong gluten-free diet (GFD) — complete exclusion of wheat, barley, and rye. No pharmacological treatment is standard; the diet alone resolves villous atrophy and nutritional deficiencies within 6–12 months in most patients. Provide: dietary counselling, nutritional supplementation (iron, folate, B12, vitamin D, calcium) during the recovery phase, bone density monitoring.
Tropical sprue: Folic acid 5 mg/day (addresses the folate deficiency component) + tetracycline 250 mg four times daily × 3–6 months (eradicates the suspected bacterial overgrowth/trigger). Most patients respond to this regimen with mucosal healing and resolution of diarrhoea.
Irritable Bowel Syndrome (IBS): Lifestyle measures (fibre, dietary modification, stress management) are first-line. Pharmacological: antispasmodics (mebeverine, dicyclomine) for abdominal cramping; low-dose tricyclic antidepressants (amitriptyline 10–25 mg nocte) for diarrhoea-predominant IBS (reduce intestinal motility, pain modulation); loperamide for diarrhoea-predominant IBS (ONLY in functional IBS, NOT in IBD or infective causes).
Surgical Indications in Inflammatory Bowel Disease
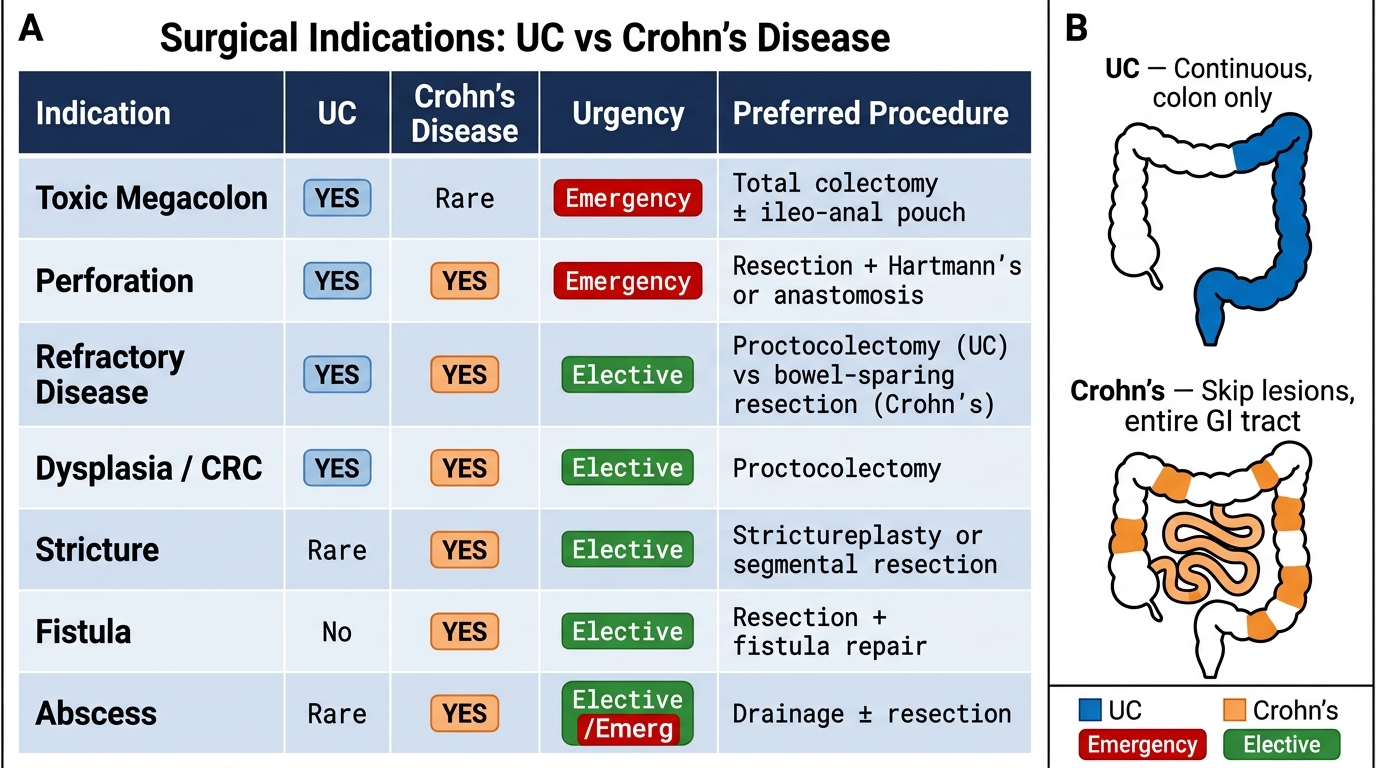
Surgery in inflammatory bowel disease is not a failure of medical therapy — it is a planned component of the therapeutic strategy for specific indications that cannot be managed medically. The crucial conceptual distinction is that surgery is potentially curative in UC (colectomy removes the diseased organ, eliminating the risk of colitis-related complications and colorectal carcinoma), while surgery in Crohn's disease is not curative (the disease can recur anywhere in the GI tract) and is therefore used only for complications, not to achieve remission. Understanding this distinction is the core of IM16.17. The conceptual clarity about what surgery achieves — cure in UC, complication management only in CD — is the foundation for every surgical timing decision. Crucially, in UC, the option of curative surgery should be proactively discussed with patients who have refractory disease, steroid dependence, or dysplasia — framing surgery as an empowering therapeutic option rather than a failure of medical care, and allowing the patient to make an informed decision about timing.
Surgical indications in Ulcerative Colitis:
Emergency surgical indications (require urgent surgical consultation — hours, not days):
- Toxic megacolon: acute dilatation of the colon (transverse colon diameter >6 cm on plain X-ray, accompanied by systemic toxicity — fever, tachycardia, leucocytosis, hypoalbuminaemia). Maximal medical therapy (IV corticosteroids, IV antibiotics, NG suction, IV fluids, bowel rest) is given for 48–72 hours; if no improvement, immediate colectomy is life-saving. Perforation risk with toxic megacolon is 20–30% and carries high mortality.
- Perforation: surgical emergency — peritoneal signs, sudden worsening after apparent improvement, free air under diaphragm on X-ray/CT. Immediate laparotomy.
- Massive haemorrhage: uncommon; if uncontrolled by endoscopic or interventional radiological means, emergency colectomy.
Elective surgical indications (planned, can be timed):
- Medically refractory UC: disease not controlled by optimal medical therapy including biologics; chronic unacceptable quality of life from ongoing symptoms despite maximal treatment
- Steroid dependence: patient cannot be weaned from corticosteroids without disease relapse; long-term steroid use carries unacceptable consequences
- High-grade dysplasia or colorectal carcinoma: UC increases the risk of colorectal carcinoma (relative risk 2× after 10 years, higher with pancolitis and young age of onset); high-grade dysplasia in surveillance colonoscopy biopsies is an indication for colectomy (prophylactic or therapeutic)
- Growth retardation in children with refractory UC
Procedure of choice: Total proctocolectomy with ileo-anal pouch anastomosis (IPAA / 'J-pouch procedure') — removes the entire colon and rectum (eliminates cancer risk and colitis) while restoring bowel continuity via an ileal J-pouch connected to the anal sphincter. Avoids a permanent ileostomy in most patients. Defunctioning ileostomy is often created initially and closed 2–3 months after the pouch heals. Proctocolectomy + permanent ileostomy (Brooke ileostomy) is an alternative for patients with poor sphincter function (poor candidates for the J-pouch) or those who prefer certainty.
Surgical indications in Crohn's Disease:
Crohn's surgery is for complications — NOT to achieve remission. The disease recurs post-operatively in most patients (clinical recurrence 20% per year; endoscopic recurrence 70–80% within 1 year).
Indications:
- Intestinal obstruction from stricture (fibrotic stricture unresponsive to dilation or balloon endoscopy)
- Internal and external fistulae (enteroenteric, enterovesical, enterocutaneous) that do not respond to medical therapy (metronidazole, ciprofloxacin, infliximab)
- Perianal fistulae and abscesses: examination under anaesthesia (EUA) + drainage + seton placement; occasionally proctectomy for severe perianal Crohn's
- Intra-abdominal abscess: percutaneous drainage + IV antibiotics followed by elective surgical resection of the diseased bowel segment after the sepsis has settled
- Free perforation: rare in CD (unlike UC); immediate laparotomy
- Short segment stricture: stricturoplasty (longitudinal incision + transverse closure — widens the lumen without resecting bowel, preserving intestinal length in patients already at risk of short bowel syndrome)
- Failure to respond to maximal medical therapy in a limited, symptomatic bowel segment: resection of that segment as a last resort
Post-operative prophylaxis in Crohn's: After resection, start azathioprine or 6-MP within 3 months (reduces post-operative recurrence rate). Anti-TNF (infliximab) post-operatively for high-risk patients (extensive prior resections, fistulising disease, young age at diagnosis).
Surgical Indications in IBD: UC vs Crohn's Disease
SELF-CHECK
A 28-year-old woman with a 5-year history of ulcerative colitis (pancolitis) is admitted with toxic megacolon — transverse colon diameter 7 cm on plain X-ray, fever 39.2°C, HR 118/min, and leucocyte count 18×10⁹/L. She has received 48 hours of maximal medical therapy (IV hydrocortisone, IV antibiotics, bowel rest, IV fluids) without improvement. What is the appropriate next step?
A. Add infliximab 5 mg/kg IV to 'rescue' the colon before considering surgery
B. Increase the IV hydrocortisone dose and continue medical management for a further 5 days
C. Urgent surgical consultation for colectomy
D. Perform an emergency colonoscopy to assess disease extent and activity
Reveal Answer
Answer: C. Urgent surgical consultation for colectomy
Toxic megacolon (colon diameter >6 cm + systemic toxicity) in UC that fails to respond to 48–72 hours of maximal medical therapy is an indication for urgent colectomy. Continuing medical therapy beyond this window significantly increases the risk of perforation (20–30% with toxic megacolon, carrying high mortality) without improving outcomes. Infliximab 'rescue therapy' can be attempted in some centres as an alternative to immediate colectomy in selected cases, but the standard of care after 48–72 hours of failed medical therapy is surgery. Emergency colonoscopy is contraindicated in toxic megacolon — it risks perforation. Total colectomy (often with a temporary ileostomy) is life-saving; reconstruction with an ileo-anal pouch can be planned as a staged procedure once the patient has recovered.