Page 5 of 21
IM17.{2,4-5} | Headache Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit and document a structured headache history covering onset, temporal pattern, characteristics, aura, associated symptoms, precipitants, analgesic use, and impact on function
- Apply the SNNOOP10 red-flag screen systematically during history-taking
- Demonstrate a complete neurological examination in a headache patient including fundoscopy, meningeal signs, and cranial nerve assessment
- Identify and elicit signs of raised intracranial pressure and meningeal irritation (papilloedema, Kernig's, Brudzinski's, nuchal rigidity)
- Generate, document, and present a structured differential diagnosis for headache presentations with clinical justification
INSTRUCTIONS
This module develops the clinical skills of headache history-taking, neurological examination, and differential diagnosis generation. These are SH-level competencies that require demonstration in clinical settings. Work through the structured framework systematically in every headache consultation until it becomes automatic.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 17 — Headache (textbook)
- API Textbook of Medicine, 10th ed. — Headache and Neurological Examination (textbook)
- British Association for the Study of Headache (BASH) Guidelines for All Healthcare Professionals in the Diagnosis and Management of Migraine, Tension-type, Cluster and Medication-overuse Headache, 4th edition (guideline)
- DeMyer's The Neurologic Examination, 6th ed. — Meningeal Signs and Raised ICP (textbook)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients present to your outpatient clinic within the same hour, each with a chief complaint of headache. The first is a 32-year-old woman who describes throbbing pain on the left side of her head for the past two days, accompanied by nausea, sensitivity to light, and aggravated by climbing stairs. The second is a 55-year-old man who says he has had a dull headache for the past three weeks that is gradually getting worse — it is worst when he wakes up in the morning, and twice last week he vomited without any nausea. Both patients use the word 'headache.' Your job is to generate, from these two histories alone, a differential diagnosis that is completely different for each patient — and to know which physical examination findings to look for to confirm or refute each hypothesis. The history you take in the next 10 minutes will determine whether you reassure and treat, or send this patient urgently for imaging. The clinical evaluation of headache is not a routine task — it is a high-stakes diagnostic skill.
WHY THIS MATTERS
The history and physical examination are the primary diagnostic instruments in headache medicine. Unlike most other organ systems where investigations frequently confirm or modify the clinical impression, in headache the diagnosis is made at the bedside — imaging and laboratory tests serve only to exclude secondary causes, not to establish a positive diagnosis of migraine or tension-type headache. The NMC competencies IM17.2 (elicit, document, and present a headache history), IM17.4 (demonstrate a detailed neurological examination including signs of raised ICP and meningitis), and IM17.5 (generate, document, and present a differential diagnosis) are assessed at the SH level — meaning you must demonstrate the skill, not merely describe it. In clinical examinations and postings, a systematic structured headache history with targeted neurological examination and a reasoned differential is the expected competency.
RECALL
Before proceeding, consolidate your prior learning. From your headache foundations module, recall the ICHD-3 primary headache types: migraine (pulsating, unilateral, 4–72h, nausea/photophobia, aggravated by activity), tension-type headache (bilateral, pressing, mild-moderate, no nausea, not aggravated), and cluster headache (severe, unilateral periorbital, 15–180 min, ipsilateral autonomic features). Recall the SNNOOP10 red flags that mandate investigation. From your neuroanatomy, recall that the meninges are pain-sensitive and that meningeal irritation produces neck stiffness (nuchal rigidity), Kernig's sign (inability to extend knee with hip flexed), and Brudzinski's sign (neck flexion induces hip and knee flexion). Recall that raised intracranial pressure classically produces morning headache (CSF pressure highest in recumbency), vomiting, and papilloedema on fundoscopy. These findings from the examination will direct your differential.
The Structured Headache History: Indication and Framework
The headache history is the single most important diagnostic tool available to the clinician. In primary headache disorders — which account for over 90% of headache presentations — the diagnosis rests entirely on the pattern of symptoms over time, and no biomarker, blood test, or imaging modality can substitute for a well-taken history. In secondary headache disorders, the history identifies the red-flag features that direct investigation. The clinical indication for taking a structured headache history is therefore universal: every patient presenting with headache, regardless of apparent severity or prior diagnosis, requires a systematic assessment.
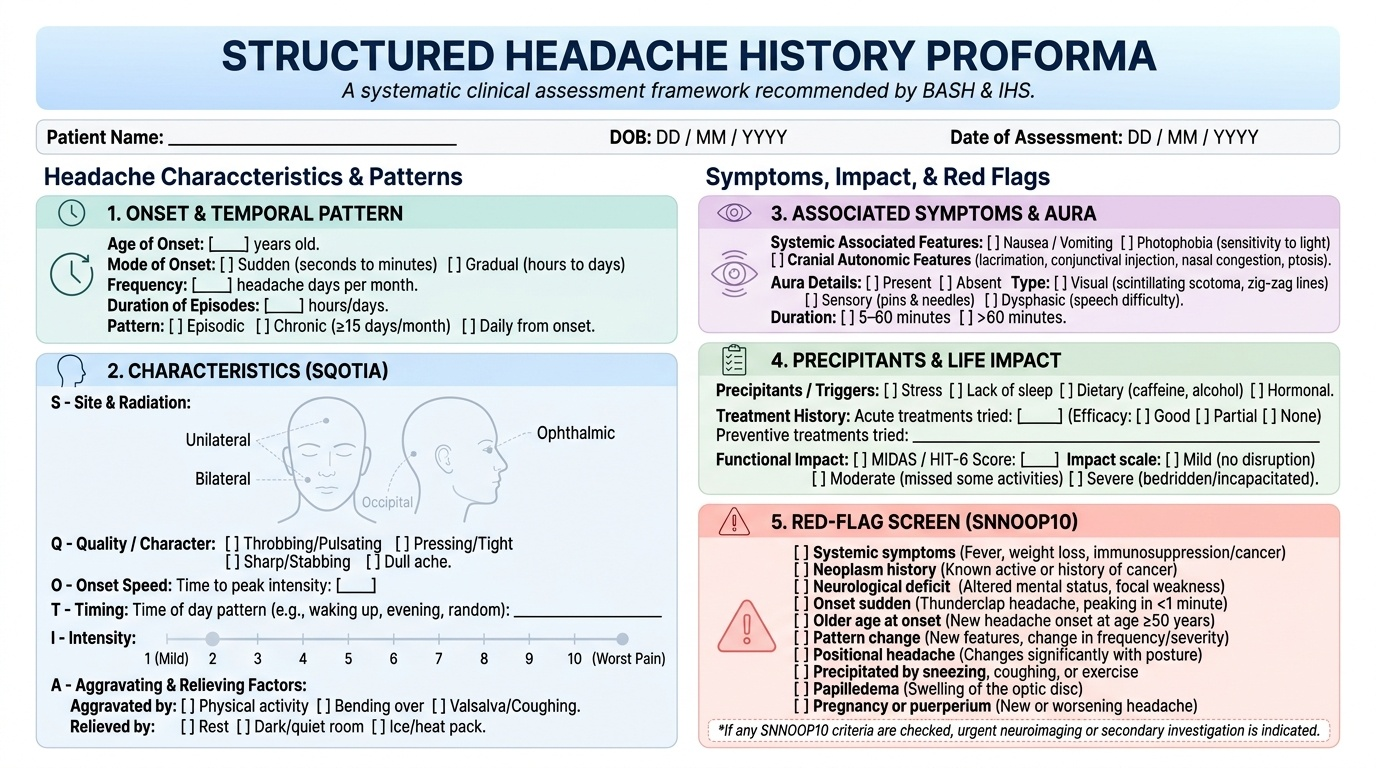
Provided image
The purpose of the headache history is threefold: first, to characterise the headache phenotype precisely enough to match it against ICHD-3 diagnostic criteria for a specific primary headache syndrome; second, to identify any SNNOOP10 red-flag features that mandate investigation for a secondary cause; and third, to assess the impact of headache on the patient's daily functioning and quality of life, which informs decisions about preventive therapy and disability management. Achieving all three goals requires a structured approach — not a free-form conversation — because patients vary enormously in how they volunteer information, and an unstructured approach consistently misses key discriminating features.
A validated framework widely used in clinical practice and recommended by the British Association for the Study of Headache (BASH) and the Indian Headache Society organises the headache history into the following domains: headache onset (age at first attack, mode of onset — sudden/gradual), headache frequency and temporal pattern (episodic vs daily, number of days/month, duration of episodes, time of day), headache characteristics (site, radiation, quality/character, severity), associated symptoms (nausea, vomiting, photophobia, phonophobia, aura, autonomic features, neurological symptoms, systemic symptoms), precipitating and aggravating factors (activity, posture, menstrual cycle, alcohol, stress, sleep deprivation, weather), relieving factors (analgesics — type, frequency, response), prior treatment history (what has been tried, at what dose, with what result), family history (migraine is highly heritable), and impact on function (work, school, social activities). Each domain maps onto one or more aspects of the diagnostic classification or red-flag screen.
Eliciting the Headache History: Key Questions and Discriminating Features
The technical skill of history-taking lies in asking the right questions in the right order and recognising which answers are diagnostically decisive. The following key questions and their clinical interpretation are essential for competent headache evaluation at the SH level.
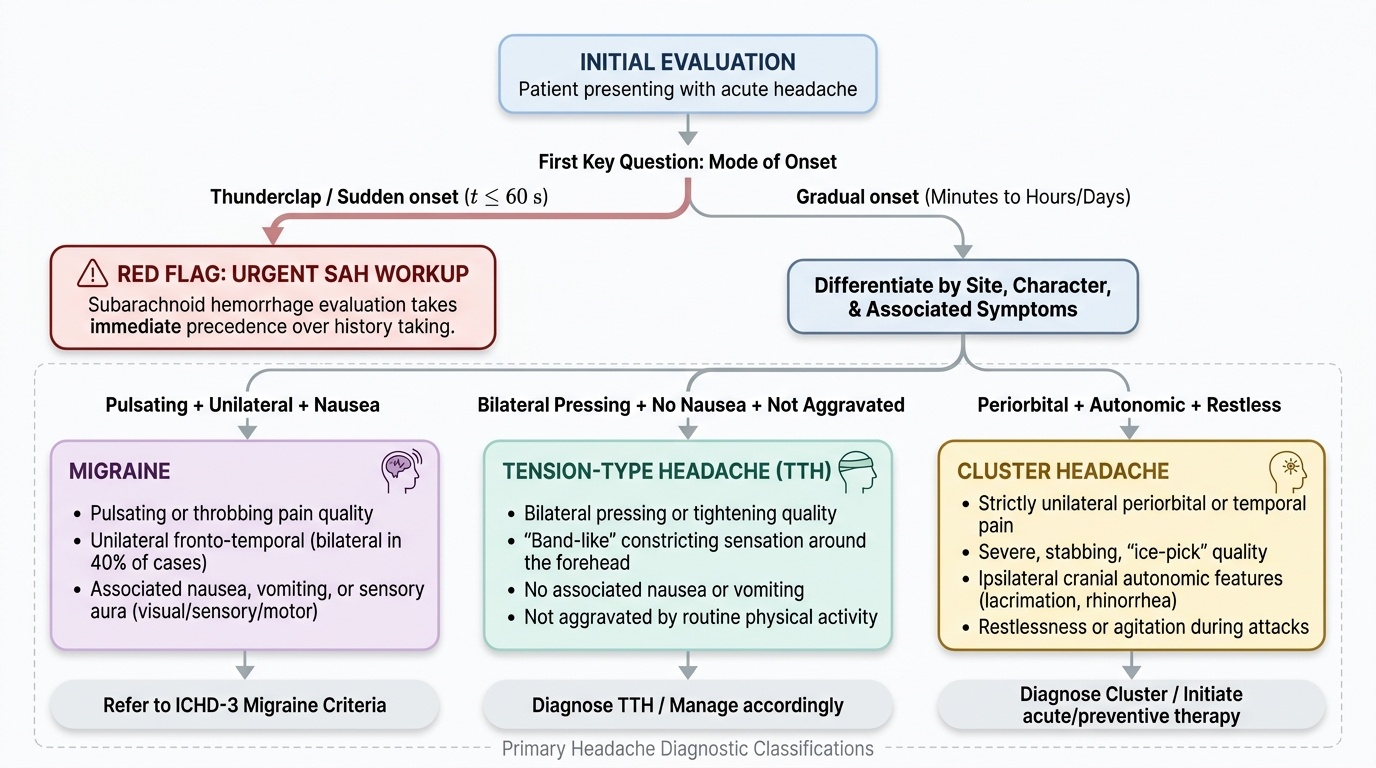
Provided image
Mode of onset is the single most important discriminating question. 'Did the pain come on suddenly, reaching maximum intensity within a minute or so, or did it build up gradually over minutes to hours?' A thunderclap onset — maximum intensity within 60 seconds — mandates the SAH workup before any further history is taken; it is a red flag that takes precedence over the full structured history. Gradual onset over 20–60 minutes is typical of migraine; gradual onset over hours to days suggests tension-type headache or raised ICP.
Site and radiation: 'Where exactly is the pain? Does it stay in one place or spread?' Unilateral fronto-temporal pain is typical of migraine but is not invariable — migraine can be bilateral in up to 40% of adults. Bilateral pressing pain favours tension-type. Strictly unilateral periorbital pain with ipsilateral eye tearing is cluster headache. Occipital pain radiating up and over the head in a 'band' pattern suggests cervicogenic headache. Vertex pain or bifrontal pain associated with morning worsening and vomiting suggests raised ICP.
Character of the pain: 'How would you describe the pain — throbbing/pulsating, pressing/squeezing, stabbing, burning, or something else?' Pulsating/throbbing quality is a positive ICHD-3 criterion for migraine. Pressing or tightening ('like a band around the head') is characteristic of tension-type. Severe, stabbing, 'ice-pick' quality periorbital pain is cluster headache.
Aura: 'Before the headache starts, do you get any warning symptoms — visual disturbances like zigzag lines or blind spots, tingling, weakness, or difficulty speaking?' Eliciting aura requires specific prompting because many patients do not volunteer these symptoms and may not associate them with the headache. Ask separately about each aura type: visual, sensory, motor, speech. If aura is present, establish its onset-to-peak time (must be ≥5 minutes for ICHD-3 migraine with aura), duration (5–60 minutes), and temporal relationship to the headache (occurs before, during, or rarely after). Ask about aura WITHOUT subsequent headache — a common pattern that leads patients to seek ophthalmological rather than neurological help.
Associated symptoms: 'During the headache, are you bothered by bright light? By noise? Do you feel sick or vomit? Do you have any eye watering, nasal stuffiness, or drooping of an eyelid?' Photophobia and phonophobia are associated features of migraine; their ABSENCE is a positive feature distinguishing tension-type from migraine. Ipsilateral lacrimation, nasal congestion, and ptosis are autonomic features of cluster headache. Fever, neck stiffness, or rash suggests meningitis.
Precipitating factors: Common migraine triggers include stress, sleep disruption, skipping meals, alcohol (especially red wine and beer), hormonal changes (perimenstrual), bright lights, and strong smells. Identify these proactively, as trigger avoidance is a first-line non-pharmacological management tool.
Analgesic use: 'How many days per month do you take painkillers for your headache, and which ones?' This question directly screens for medication-overuse headache (MOH) — a major cause of chronic daily headache. Regular use of simple analgesics or NSAIDs on ≥15 days/month, or triptans on ≥10 days/month, for >3 months is the ICHD-3 threshold for MOH.
SELF-CHECK
A 38-year-old woman presents with recurrent headaches. You ask about associated symptoms and she mentions that during attacks she has right-sided eye watering and a runny right nostril, and that she cannot sit still — she paces the room. She describes the pain as a 'drilling sensation' behind the right eye, lasting 45–60 minutes. Which diagnosis does this history most strongly support, and which history question has the highest discriminating value?
A. Migraine with aura; the most discriminating question is about visual disturbances before headache
B. Tension-type headache; the most discriminating question is about bilateral pressing quality
C. Cluster headache; the most discriminating question is about ipsilateral autonomic symptoms and restlessness
D. Subarachnoid haemorrhage; the most discriminating question is about thunderclap onset
Reveal Answer
Answer: C. Cluster headache; the most discriminating question is about ipsilateral autonomic symptoms and restlessness
Unilateral periorbital severe pain (45–60 minutes duration), ipsilateral lacrimation and rhinorrhoea (cranial autonomic features), and restlessness (inability to stay still, pacing) are the hallmark triad of cluster headache. The most discriminating history question is specifically about ipsilateral autonomic symptoms (eye watering, nasal discharge, conjunctival injection, ptosis) and behaviour during attacks (restlessness vs preference for lying still). Migraine patients typically prefer rest in a dark quiet room — the restlessness of cluster headache directly contrasts with this. Aura questions are key for migraine subtyping, not cluster headache diagnosis.
Documenting and Presenting the Headache History
Clinical documentation of a headache history serves three distinct purposes: it creates a medicolegally defensible record of the consultation, it enables continuity of care by communicating the headache phenotype precisely to other clinicians, and it provides the structured dataset required to apply ICHD-3 diagnostic criteria systematically. Poor documentation — vague entries like 'complains of headache, prescribed analgesics' — is a common quality-of-care failure that prevents accurate diagnosis and appropriate management. Final-year MBBS students are expected to produce structured, complete headache documentation that any other clinician can use to verify the diagnosis.
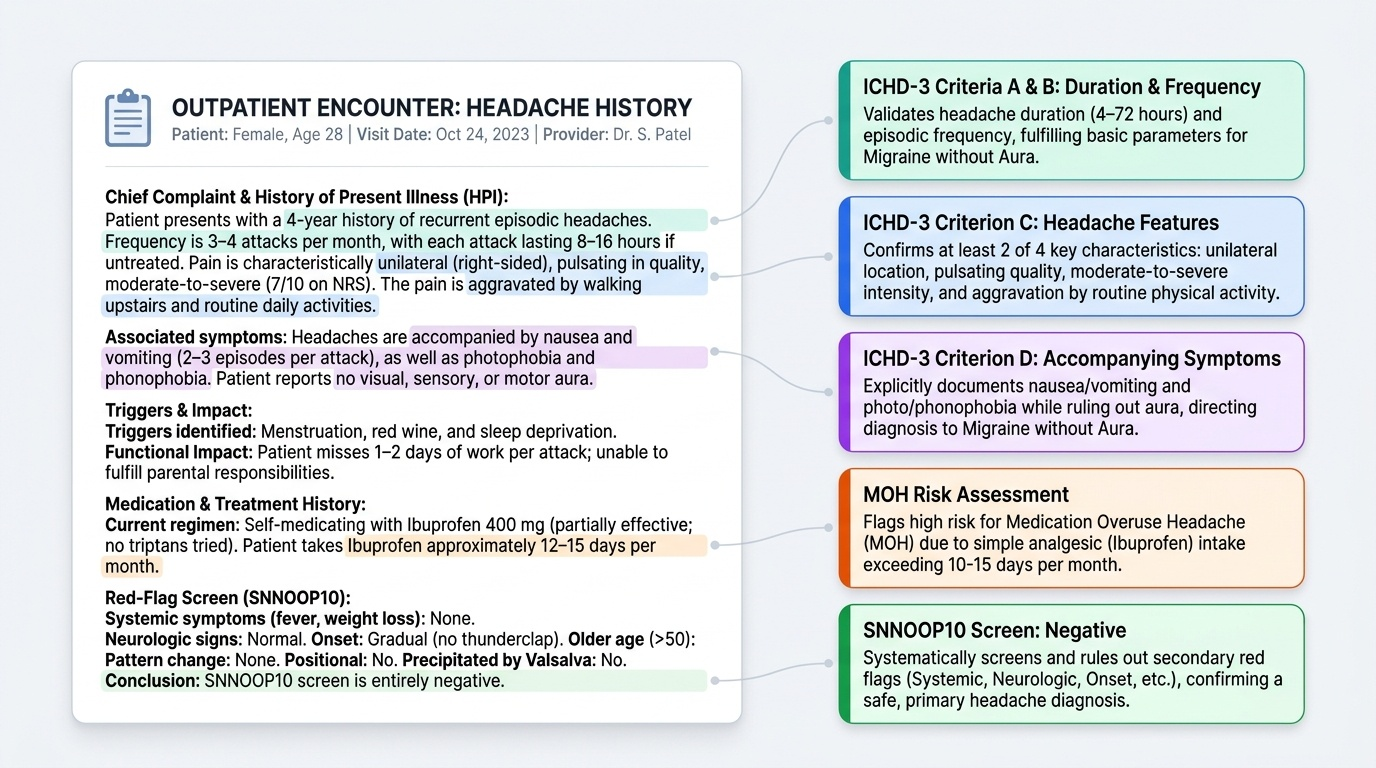
Provided image
A complete headache history documentation should include: (1) Chief complaint with temporal framing: 'Recurrent episodic headache for 4 years, 3–4 attacks per month, each lasting 8–16 hours.' (2) Headache characterisation: 'Unilateral (right-sided > left), pulsating quality, moderate-to-severe intensity (7/10 NRS), aggravated by walking upstairs or routine activity.' (3) Associated features enumerated explicitly: 'Accompanied by nausea, vomiting (2–3 episodes per attack), photophobia, phonophobia. No aura reported.' (4) Triggers identified: 'Triggered by menstruation, red wine, and sleep deprivation.' (5) Treatment history with response: 'Self-medicating with ibuprofen 400 mg, partially effective; no triptan tried. Takes ibuprofen approximately 12–15 days per month — screen positive for MOH risk.' (6) Impact on function: 'Misses work 1–2 days per attack; unable to fulfil parental responsibilities during attacks.' (7) Red-flag screen: 'No thunderclap onset. No neurological deficit. No fever. No vomiting without nausea. No morning worst headache. No weight loss. No visual loss. No recent change in pattern.' (8) Family history: 'Mother has diagnosed migraine.'
When presenting the history to a senior clinician or at a case presentation, the structured summary follows: 'This is a 32-year-old woman with a 4-year history of episodic migraine without aura, 3–4 attacks per month, consistent with ICHD-3 criteria: unilateral, pulsating, severe, aggravated by activity, with nausea and photophobia. No aura documented. SNNOOP10 screen negative. Currently at risk of MOH given ibuprofen use on 12–15 days/month. Family history of migraine. No prior preventive therapy. Assessment: episodic migraine without aura, approaching MOH threshold. Plan: triptan trial, headache diary, counselling regarding analgesic overuse.'