Page 6 of 21
IM17.{2,4-5} | Headache Clinical Evaluation — SDL Guide (Part 2)
Neurological Examination in the Headache Patient
The physical examination in a headache patient serves to identify objective signs of intracranial disease that would be missed by history alone, to establish a baseline neurological status before any treatment is initiated, and to detect meningeal irritation or raised intracranial pressure — the two examination syndromes that most directly alter the urgency and direction of management. A complete neurological examination is mandatory in any new headache presentation; a focused examination re-checking relevant components is appropriate at follow-up visits.
The neurological examination in a headache patient is structured into six components, performed in the following order to ensure completeness.
1. General and vital signs: Blood pressure (malignant hypertension: diastolic >120–130 mmHg with headache, vomiting, and papilloedema), heart rate, temperature (fever suggests infection), and level of consciousness (GCS if altered). A hypertensive emergency can cause headache indistinguishable from migraine — blood pressure is therefore a mandatory measurement in every headache consultation.
2. Higher mental functions: Orientation to time, place, and person; attention and concentration; language (aphasia suggests cortical lesion); memory. Subtle encephalopathy may manifest as confusion, agitation, or unusual behaviour in meningitis or encephalitis before frank signs appear.
3. Cranial nerve examination: All 12 cranial nerves should be assessed. Key findings relevant to headache: (a) Pupillary reactions and extraocular movements — a unilaterally dilated, sluggishly reacting pupil with ipsilateral ptosis and downward/outward deviation of the eye = third nerve palsy, suggesting posterior communicating artery aneurysm as a cause of thunderclap headache; (b) Fundoscopy — papilloedema (blurred disc margins, disc hyperaemia, venous engorgement, haemorrhages, loss of spontaneous venous pulsations) indicates raised intracranial pressure; (c) Visual fields — bitemporal hemianopia suggests pituitary tumour; homonymous hemianopia suggests contralateral occipital or optic radiation pathology; (d) Facial sensation and motor function — trigeminal and facial nerve assessment for a pontine lesion.
4. Motor system: Power, tone, reflexes, and plantar responses in all four limbs. An extensor plantar response (Babinski sign) or asymmetric hyperreflexia localises upper motor neuron pathology — a space-occupying lesion must be excluded. Focal motor weakness alongside headache should always be treated as a secondary headache until proven otherwise, even if the history appears to fit migraine (consider hemiplegic migraine as a diagnosis of exclusion).
5. Cerebellar function and gait: Finger-nose test, heel-shin test, Romberg test, gait assessment. Ataxia alongside headache suggests a posterior fossa lesion or cerebellar haematoma.
6. Meningeal irritation signs: These are the most critical examination findings in a febrile headache patient and must be elicited systematically.
Neck stiffness (nuchal rigidity): With the patient supine and relaxed, gently flex the neck toward the chest. Resistance to passive neck flexion (the neck cannot be flexed so that the chin touches the chest) indicates meningismus — meningeal irritation from infection, blood, or malignant cells in the CSF. The test is positive when there is involuntary resistance; the examiner should not use force.
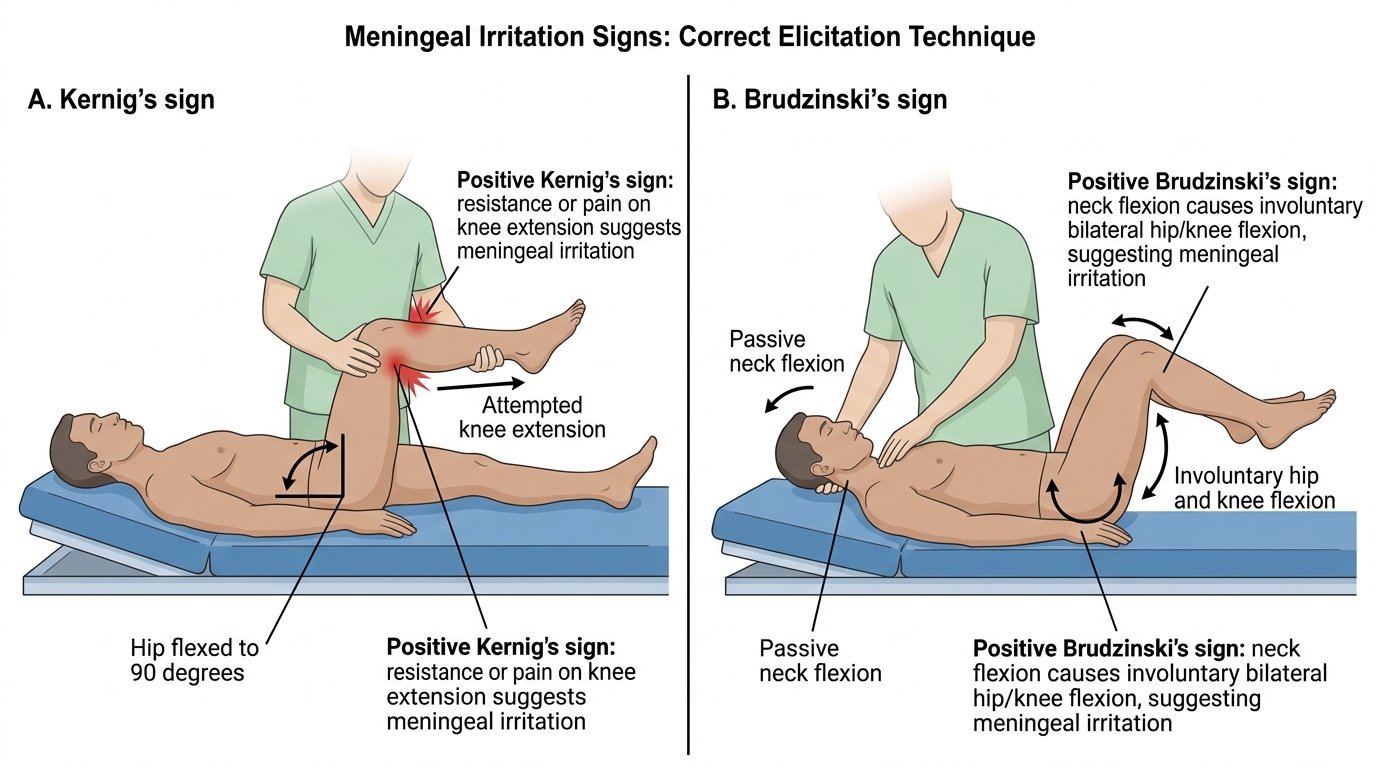
Kernig's sign: With the patient supine, flex the hip to 90° and then attempt to extend the knee. A positive sign is inability to fully extend the knee (beyond approximately 135°) due to pain — reflecting meningeal traction when the inflamed meninges are stretched by straightening the sciatic nerve.
Brudzinski's sign: With the patient supine, passively flex the neck. A positive sign is involuntary flexion of the hips and knees — the patient reflexively draws the legs up to reduce meningeal tension when the neck is flexed. A second Brudzinski sign: pressing on one knee with the hip flexed produces contralateral hip and knee flexion.
The sensitivity and specificity of these signs: Kernig's and Brudzinski's have sensitivity of only 5–30% for bacterial meningitis but high specificity (~95%). Their presence is highly significant; their absence does NOT exclude meningitis in an obtunded patient. Neck stiffness is more sensitive (~70%) but less specific. In clinical practice, the combination of fever, headache, and ANY degree of neck stiffness should prompt CSF examination.
Kernig's and Brudzinski's Signs
SELF-CHECK
While performing fundoscopy on a 40-year-old man with a 3-week history of progressively worsening morning headache and two episodes of effortless vomiting, you notice blurred disc margins and loss of the optic disc cup bilaterally. What is the most significant finding, and what does it indicate?
A. Arteriovenous nipping — indicates chronic hypertension
B. Papilloedema — indicates raised intracranial pressure and mandates urgent imaging
C. Cupping of the optic disc — indicates chronic open-angle glaucoma
D. Flame-shaped haemorrhages — indicates central retinal vein occlusion
Reveal Answer
Answer: B. Papilloedema — indicates raised intracranial pressure and mandates urgent imaging
Blurred disc margins and loss of the optic cup (disc hyperaemia, venous engorgement, elevation of the disc) constitute papilloedema — bilateral swelling of the optic disc due to raised intracranial pressure transmitted via the optic nerve sheath. In the context of progressively worsening morning headache (a SNNOOP10 positional red flag — worse on waking, relieved when upright, typical of raised ICP) and effortless vomiting (vomiting without preceding nausea, classic for raised ICP), papilloedema confirms the clinical suspicion of raised intracranial pressure from a space-occupying lesion and mandates urgent MRI brain with contrast. This is NOT a finding to monitor — it requires same-day imaging. A-V nipping is hypertensive retinopathy; cupping is glaucoma; flame haemorrhages indicate CRVO.
Signs of Raised Intracranial Pressure
Raised intracranial pressure (raised ICP) produces a recognisable clinical syndrome that the examining clinician must recognise and act upon urgently. The intracranial compartment is a closed rigid box — the Monro-Kellie doctrine states that the total volume of brain, CSF, and blood within the skull is constant, and any increase in one component requires a compensatory decrease in another. When compensation is exhausted, ICP rises and cerebral perfusion pressure falls, ultimately leading to brainstem herniation and death if untreated. Recognising raised ICP at the clinical examination stage allows urgent intervention before this irreversible stage is reached.
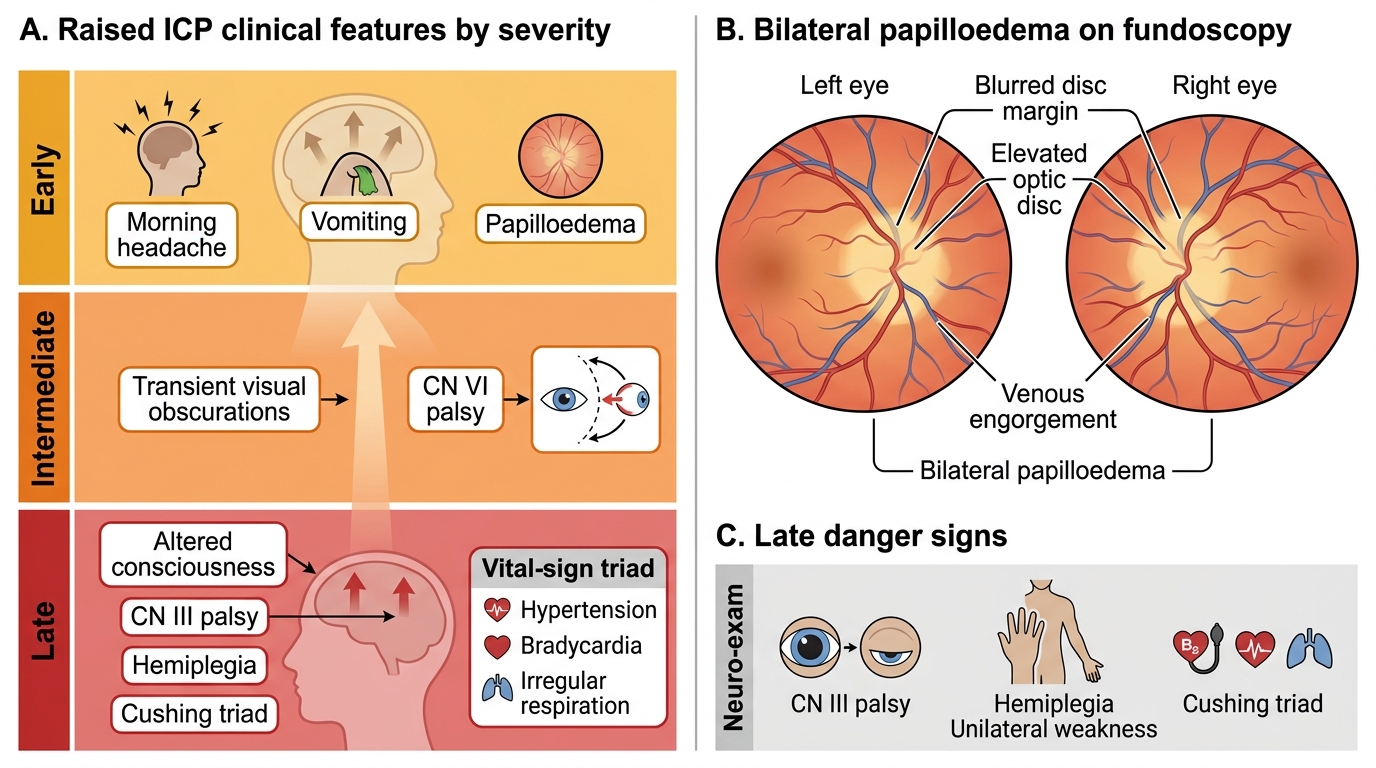
The classic Cushing's triad — hypertension + bradycardia + irregular breathing — is a late and ominous sign indicating impending brainstem herniation from massively elevated ICP. It must not be awaited before acting; management must begin at the first clinical suspicion of raised ICP, long before the Cushing triad appears.
The clinical features of raised ICP in order of typical progression are as follows. Early features: headache that is worse on waking (highest ICP occurs during recumbency due to increased venous return and reduced CSF resorption), worse with Valsalva manoeuvre (coughing, straining, bending forward), and relieved by sitting upright. Vomiting without preceding nausea — 'effortless' or 'projectile' vomiting — due to direct stimulation of the vomiting centre in the medullary floor of the fourth ventricle. Papilloedema on fundoscopy — a critical sign that confirms raised ICP and excludes migraine or tension-type headache as the explanation. The absence of papilloedema does NOT exclude raised ICP, especially in acute presentations (papilloedema takes 24–48 hours to develop after acute ICP elevation). Visual obscurations — brief greying or blackening of vision lasting seconds, typically on standing, due to transient reduction in optic nerve perfusion.
Late features (indicating herniation syndromes): altered consciousness, unilateral third nerve palsy (ipsilateral fixed dilated pupil — 'blown pupil') from uncal herniation compressing CN III against the tentorium; contralateral hemiplegia from cerebral peduncle compression; Cheyne-Stokes breathing; and finally, the Cushing triad. The sixth nerve (abducens) is a non-localising sign of raised ICP — a unilateral or bilateral CN VI palsy (convergent squint, diplopia on lateral gaze) can occur in raised ICP from any cause because CN VI has the longest intracranial course and is vulnerable to stretching.
In the Indian clinical context, important causes of raised ICP include: space-occupying lesion (primary or metastatic brain tumour, brain abscess — tuberculoma is an important cause in India), hydrocephalus (obstructive from tumour or cysticercosis; communicating from post-meningitic scarring), cerebral venous sinus thrombosis (CVT — important cause in young women in India, associated with dehydration, puerperium, oral contraceptive use, thrombophilia), idiopathic intracranial hypertension (IIH — raised ICP without a structural cause, seen in obese young women, presents with daily headache and papilloedema, diagnosis requires opening CSF pressure >25 cmH₂O on LP), and subdural haematoma (history of trauma — sometimes trivial — in elderly or anticoagulated patients).
Raised Intracranial Pressure: Clinical Severity and Papilloedema
Generating a Differential Diagnosis
Generating a structured differential diagnosis for a patient presenting with headache requires synthesising the history findings and examination results into a probabilistic clinical reasoning framework. The process is not a list-recall exercise — it requires active reasoning about which diagnostic category is most consistent with the clinical picture, which alternative diagnoses must be excluded, and which findings would be expected if each diagnosis were correct. At the SH competency level, you are expected to produce, document, and present a differential diagnosis that is reasoned, prioritised, and linked to the clinical evidence.
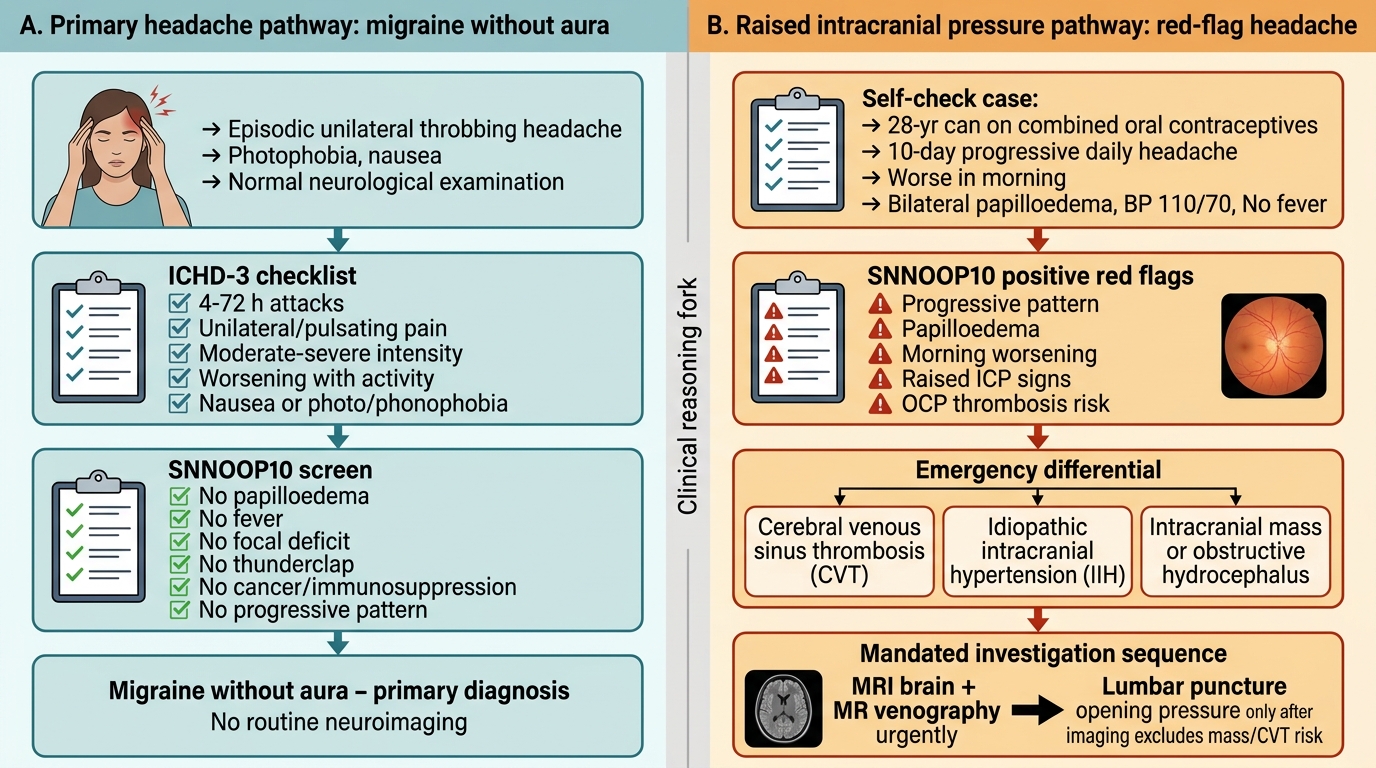
The differential diagnosis generation process for headache follows a three-step framework. Step 1: Probability ranking by pattern recognition. Apply ICHD-3 criteria to the headache characteristics. If the headache fits a primary syndrome (migraine, TTH, cluster) without any red flags, the primary diagnosis is at the top of the differential. If SNNOOP10 red flags are present, shift the primary diagnoses downward and raise the urgency of the secondary causes.
Step 2: Exclude dangerous diagnoses. Regardless of how typical the primary headache phenotype appears, the following diagnoses must be considered and either excluded clinically or by investigation in specific circumstances: subarachnoid haemorrhage (thunderclap onset, any new severe headache), bacterial meningitis (fever + neck stiffness ± rash), cerebral venous thrombosis (subacute progressive headache in young women, puerperium, OCP use), hypertensive emergency (BP >180/120 with headache), space-occupying lesion (progressive headache, focal deficit, papilloedema), temporal arteritis (age >50, scalp tenderness, elevated ESR).
Step 3: Document the differential with clinical justification. Each diagnosis in the differential should be supported by a clinical reason: 'Migraine without aura — supported by pulsating unilateral headache, nausea, photophobia, aggravation by activity, 5-year history of similar attacks, family history of migraine; no red flags on SNNOOP10 screen.' 'Medication-overuse headache — supported by NSAID use 15 days/month for >3 months; pattern change toward more frequent headaches over the past year.' 'Secondary headache from SOL — excluded by: no morning predominance, no vomiting without nausea, no focal deficits, no papilloedema on fundoscopy, normal neurological examination.'
A worked example integrating both cases from the opening hook:
Case 1 (32-year-old woman, throbbing unilateral headache, nausea, photophobia, activity aggravation): Primary differential: (1) Migraine without aura — fits all ICHD-3 criteria; (2) Migraine with aura — to be confirmed by asking specifically about preceding neurological symptoms; (3) MOH if analgesic overuse confirmed. Excluded by examination: no papilloedema, no meningism, no focal deficit, BP normal. SNNOOP10 negative.
Case 2 (55-year-old man, progressive morning headache 3 weeks, vomiting without nausea): Primary differential: (1) Space-occupying lesion — progressive course, morning predominance, vomiting without nausea = raised ICP pattern; (2) Subdural haematoma — check for recent head trauma; (3) CVT — consider if risk factors present; (4) Hypertensive emergency — measure BP immediately. Investigation mandated: MRI brain with contrast urgently. Do not label as primary headache until imaging excludes SOL.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Headache Differential: Migraine vs Raised Intracranial Pressure
SELF-CHECK
A 28-year-old woman on combined oral contraceptives presents with a 10-day history of progressively worsening daily headache, worse in the morning. She has no fever. Neurological examination reveals bilateral papilloedema. Blood pressure is 110/70 mmHg. What is the most important diagnosis to consider at the top of the differential, and what investigation is most urgently required?
A. Migraine without aura — reassure and prescribe a triptan
B. Idiopathic intracranial hypertension — LP for opening pressure after MRI/MRV
C. Tension-type headache — prescribe NSAIDs and reassure
D. Bacterial meningitis — LP immediately for CSF analysis
Reveal Answer
Answer: B. Idiopathic intracranial hypertension — LP for opening pressure after MRI/MRV
Progressive daily headache with bilateral papilloedema in a young woman on OCP raises two primary concerns: (1) cerebral venous sinus thrombosis (CVT) — OCP is a major risk factor; (2) idiopathic intracranial hypertension (IIH) — young obese women, daily headache, papilloedema, raised opening pressure >25 cmH₂O on LP. The critical first investigation is MRI brain with MR venography (MRV) to exclude CVT (a venous sinus thrombus can cause raised ICP with papilloedema and no fever). If MRV is negative, LP with opening pressure measurement confirms IIH. Migraine and TTH do NOT cause papilloedema — their presence mandates investigation. Bacterial meningitis is possible without fever but this presentation is more consistent with IIH/CVT.