Page 7 of 21
IM17.{2,4-5} | Headache Clinical Evaluation — SDL Guide (Part 3)
Self-Assessment: Applied Clinical Evaluation
The IM17.2, IM17.4, and IM17.5 competencies are assessed at the SH level — meaning the examiner expects you to demonstrate the skill of taking, documenting, and presenting a headache history, performing the relevant neurological examination, and generating a justified differential diagnosis. This section consolidates the skills covered in this module through integrative self-assessment scenarios.
Provided image
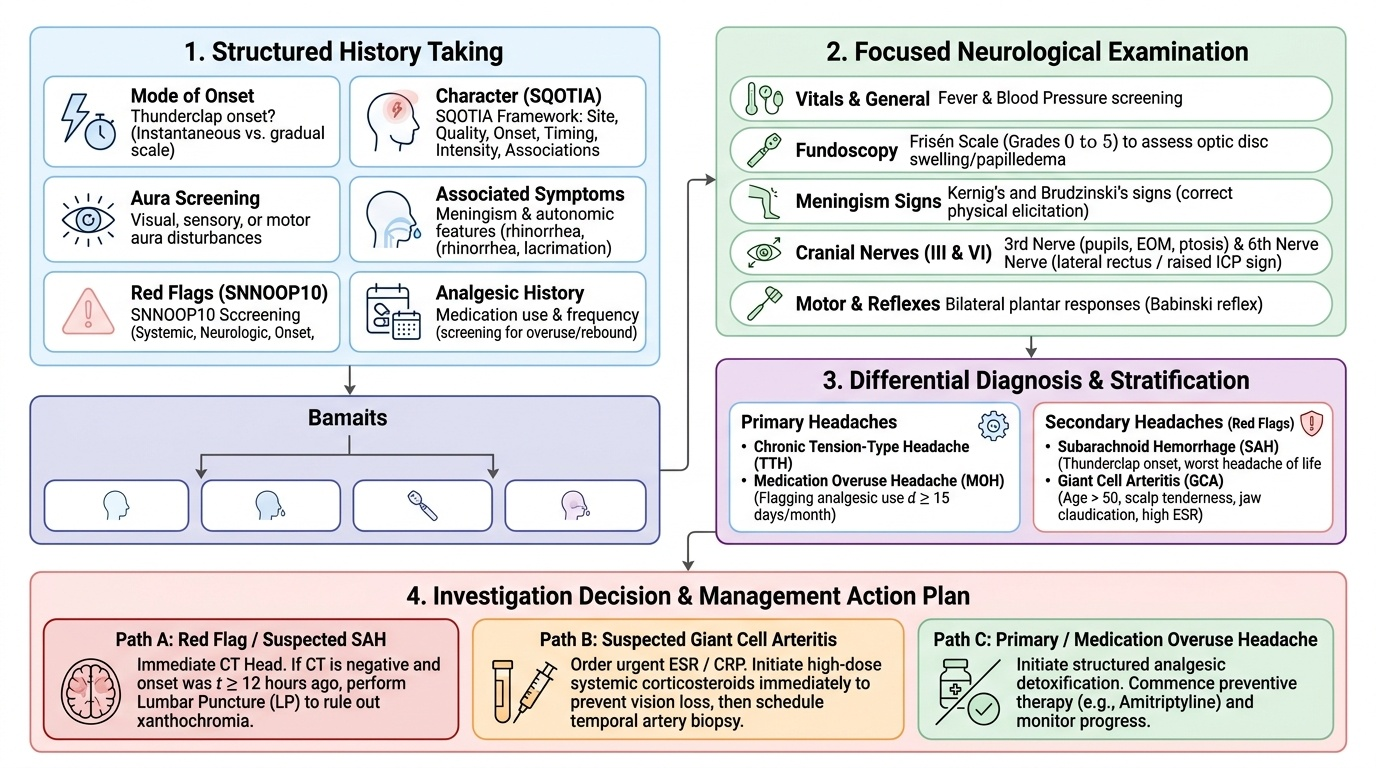
Self-assessment Task 1: Structured history-taking from a standardised patient. A 45-year-old man presents with headache. Apply the structured history framework: (a) ask the mode of onset first — is it thunderclap? (b) characterise the headache (SQOTIA), (c) screen for aura, (d) elicit associated symptoms (autonomic features, meningism symptoms), (e) screen for SNNOOP10 red flags, (f) ask about analgesic use and frequency. Document each domain explicitly. Generate a primary and secondary differential based on the history alone.
Self-assessment Task 2: Neurological examination checklist for headache. Before proceeding to examination, ensure you can perform without prompting: (a) fundoscopy looking for papilloedema — can you grade disc swelling on a scale from 0 to 5 (Frisén scale)? (b) eliciting Kernig's sign with correct technique, (c) eliciting Brudzinski's sign, (d) testing for third nerve palsy — the pupils, extraocular movements, and upper eyelid elevation, (e) checking for the sixth nerve palsy as a non-localising sign of raised ICP, (f) testing plantar responses bilaterally.
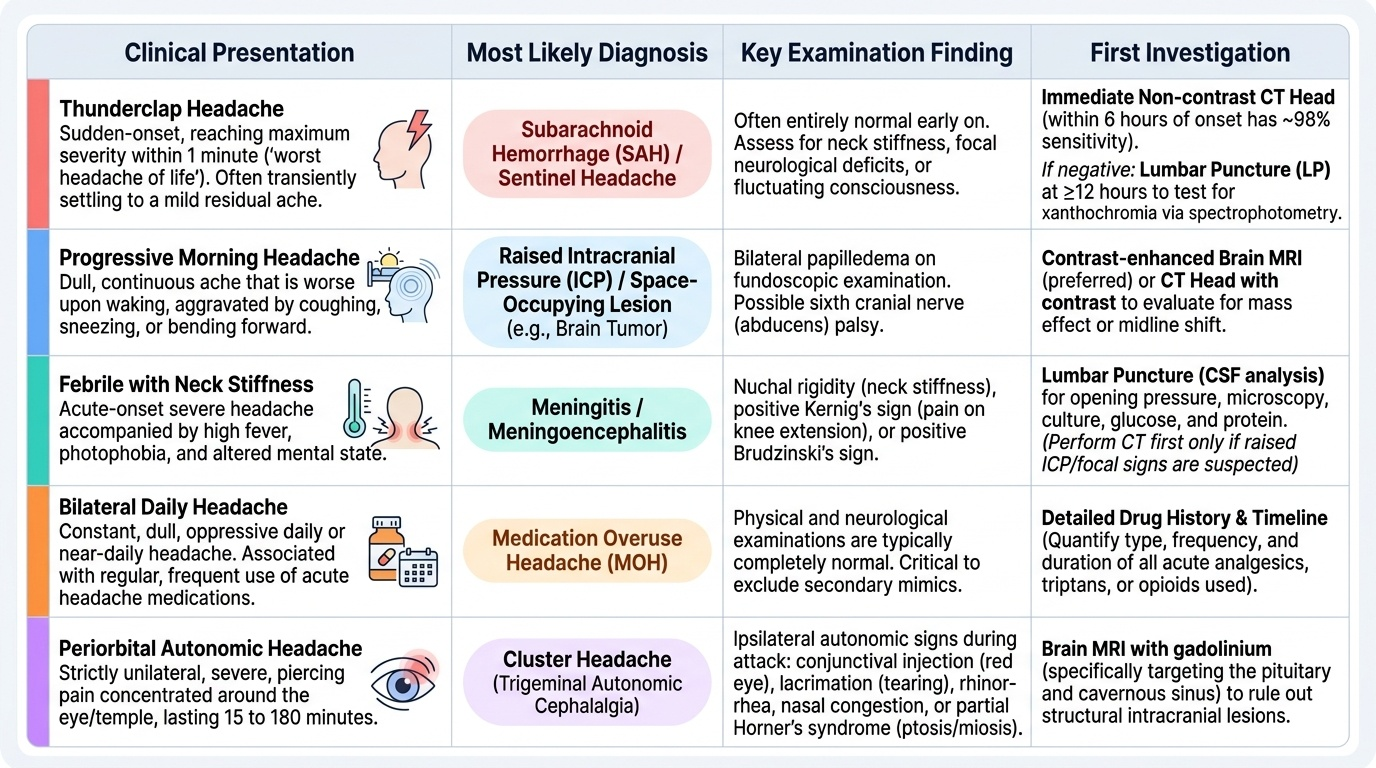
Self-assessment Task 3: Differential diagnosis exercise. For each of the following three brief histories, generate a differential diagnosis list (at minimum 3 diagnoses) with clinical justification:
- A: 19-year-old male student, sudden onset worst headache of his life, maximum intensity in 20 seconds, now largely resolved, no fever, normal examination.
- B: 35-year-old female, bilateral pressing headache daily for 6 months, no nausea, mild photophobia, takes paracetamol 16–18 days per month.
- C: 62-year-old male with new onset right-sided headache, scalp tenderness on brushing hair, jaw pain on eating, ESR 78 mm/hr.
Answers: (A) SAH until proven otherwise — CT head then LP ≥12 hours, even though largely resolved (sentinel headache); (B) Chronic TTH + MOH (paracetamol ≥15 days/month) — treatment: analgesic detoxification + amitriptyline; (C) Giant cell arteritis — high-dose prednisolone immediately (before biopsy) to prevent blindness; ESR >50 + age >50 + jaw claudication = classic triad.
Applying the Differential in Practice: Applied Scenarios
Integrating history, examination, and differential diagnosis into a coherent clinical narrative is the final skill that IM17.5 tests. In practice, this means being able to explain your reasoning to a patient, a senior colleague, and in a clinical case record — and to update the differential as new information emerges. The following scenarios provide self-testing material for applied practice at the KH-SH interface.
Provided image
Applied scenario A — Sentinel headache: A 42-year-old woman presents to the casualty department at 9 pm with a headache that came on while she was watching television, reached maximum severity 'within a minute or so,' and she describes it as 'the worst headache I've ever had.' The pain has now settled to a mild residual ache. She has no fever, no neck stiffness, and the neurological examination is entirely normal. Her GP had diagnosed her with migraine 3 years ago. The casualty officer is considering discharging her with a stronger triptan.
Assessment: This is a sentinel headache pattern — a thunderclap headache that precedes a major SAH bleed. The prior migraine history is irrelevant to this acute presentation: a sudden-onset worst-ever headache in a known migraineur still mandates the full SAH workup, because the history of migraine does NOT protect against aneurysmal rupture. The appropriate management is: non-contrast CT head immediately (she is within 6 hours of onset — CT sensitivity is ~98%); if CT is negative, LP at ≥12 hours to test for xanthochromia by spectrophotometry. Discharging without LP after a normal CT would be negligent if she re-bleeds.
Applied scenario B — Cervicogenic headache differentiation: A 48-year-old man presents with unilateral right-sided headache of 4 months' duration, radiating from the right occipital region over the vertex to the right frontal area. The pain is aggravated by sustained neck postures during office work and relieved by lying flat. There is tenderness on palpation of the right suboccipital muscles and right C2–3 facet joints. Cervical range of motion is restricted. Neurological examination is normal. SNNOOP10: positive for 'referred from cervical structures.'
Assessment: Cervicogenic headache — referred pain from upper cervical spine structures (C1–3) activating the trigeminocervical complex (overlap between trigeminal and upper cervical afferents at the trigeminal nucleus caudalis). Distinguishing features from migraine: onset from neck movement, pressure on cervical structures reproduces the headache, no nausea/photophobia, restricted cervical ROM. Management: physiotherapy (cervical joint mobilisation, postural training), cervical nerve blocks for refractory cases. This is a secondary headache (ICHD-3 Part 2: headache attributed to disorder of the cervical spine) — treated by managing the underlying cervical pathology, not with triptans.
CLINICAL PEARL
The most dangerous clinical error in headache evaluation is anchoring bias — once a patient has been labelled with migraine or tension-type headache, subsequent presentations tend to be attributed to the same diagnosis without reassessment. The rule is: any significant change in headache pattern — sudden increase in frequency, change in character, onset of new neurological symptoms, or a new headache that the patient themselves describes as different from their usual — must be evaluated as a potential new diagnosis, not assumed to be the established diagnosis worsening. This is particularly true for the 'first or worst' headache: even in a patient with a 10-year history of migraine, a headache that is genuinely different from their usual attacks must be taken seriously.
A practical tip for eliciting Kernig's sign: be gentle. The test requires the patient to be relaxed — tensing the hamstrings voluntarily (as may occur with an anxious patient) produces a false positive. Ask the patient to consciously relax the leg, and re-test if the first attempt is equivocal. In meningitis, the resistance is involuntary, painful, and reproducible.