Page 14 of 21
IM17.10-14 | Headache Emergency Care and Treatment — SDL Guide (Part 2)
Drug Regimens for Bacterial Meningitis
Bacterial meningitis is a neurological emergency that requires immediate, empirical antibiotic therapy before causative organism identification. Every hour of delay in starting antibiotics is associated with measurable increases in mortality and neurological morbidity — this is one of the clearest dose-response relationships between time-to-treatment and outcome in clinical medicine. The principles of antimicrobial selection in bacterial meningitis are: (1) adequate CSF penetration of the antibiotic — only certain agents achieve bactericidal concentrations in the CSF, primarily because of the blood-brain barrier; (2) broad spectrum empirical coverage of the most likely pathogens pending culture; and (3) dose adjustment for CNS pharmacokinetics (higher doses required for CSF penetration than for systemic infections).
Provided image
The commonest causative organisms of community-acquired bacterial meningitis vary by age:
- Neonates: Group B Streptococcus, E. coli, Listeria monocytogenes
- Infants and children: Streptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae
- Adults and young adults: Streptococcus pneumoniae (most common), Neisseria meningitidis
- Older adults (>60 years) and immunocompromised: Streptococcus pneumoniae, Listeria monocytogenes (add ampicillin to cover Listeria)
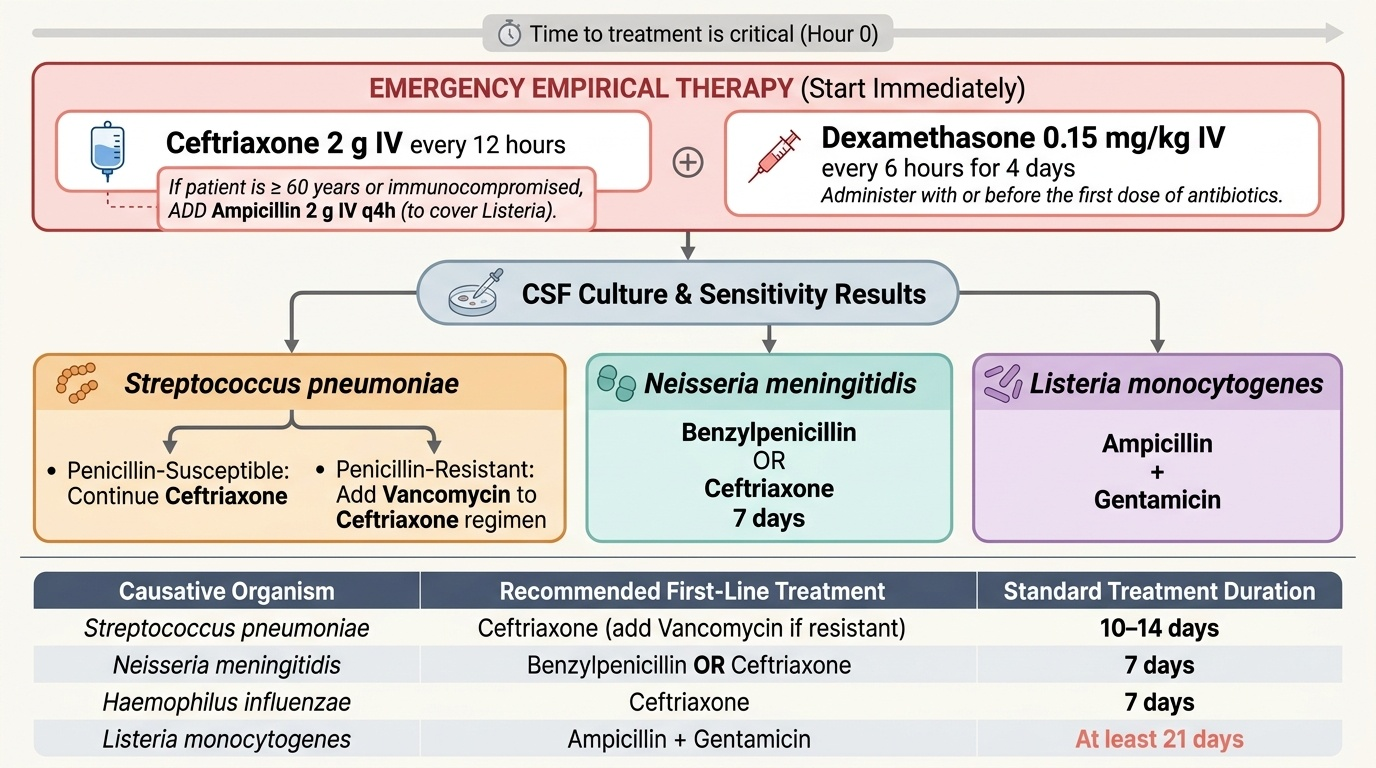
Empirical antibiotic regimen for adults with community-acquired bacterial meningitis:
First-line: Ceftriaxone 2 g IV every 12 hours (total 4 g/day). Ceftriaxone is a third-generation cephalosporin with excellent CSF penetration (CSF:serum ratio ~20–30% at inflamed meninges), broad-spectrum coverage of S. pneumoniae, N. meningitidis, and H. influenzae, long half-life allowing twice-daily dosing, and bactericidal mechanism (inhibition of cell wall synthesis via PBP binding). In penicillin-allergic patients: chloramphenicol 25 mg/kg IV every 6 hours (excellent CSF penetration, bacteriostatic against most bacteria but bactericidal for N. meningitidis and H. influenzae).
For patients ≥60 years or immunocompromised: add ampicillin 2 g IV every 4 hours to cover Listeria (ceftriaxone does not cover Listeria).
Adjunctive dexamethasone: Dexamethasone 0.15 mg/kg IV every 6 hours for 4 days, started with or before the first antibiotic dose. The mechanism: bacterial lysis by antibiotics releases cell wall fragments (lipopolysaccharide, peptidoglycan) that trigger a massive cytokine-mediated inflammatory response in the subarachnoid space, causing cerebral oedema, vasculitis, and neuronal damage. Dexamethasone suppresses this inflammatory cascade. Evidence: reduces mortality in pneumococcal meningitis; reduces hearing loss (the most common neurological sequel of bacterial meningitis, particularly S. pneumoniae) in both adults and children. Dose rationale: 0.15 mg/kg × 6 hourly = 10 mg q6h in a 70 kg adult.
Duration of treatment: Pneumococcal meningitis: 10–14 days; meningococcal: 5–7 days; Listeria: 21 days; Gram-negative bacillary (E. coli): 21 days.
Meningococcal prophylaxis for close contacts: Rifampicin 600 mg twice daily for 2 days (adults); single-dose ciprofloxacin 500 mg (oral, preferred in adults — simpler, equally effective); ceftriaxone 250 mg IM single dose (used in pregnancy — rifampicin and ciprofloxacin avoided in pregnancy). Meningococcal disease is a notifiable condition — public health notification mandatory.
Drug Regimens for Tuberculous and Viral Meningitis
Tuberculous meningitis (TBM) and viral meningitis (particularly herpes simplex encephalitis) represent the two other major infective headache-associated emergencies that require specific drug regimens beyond the bacterial meningitis protocol. Both require immediate recognition and treatment because delayed therapy significantly worsens outcome — and both have characteristic features that should trigger the specific drug without waiting for full microbiological confirmation.
Provided image
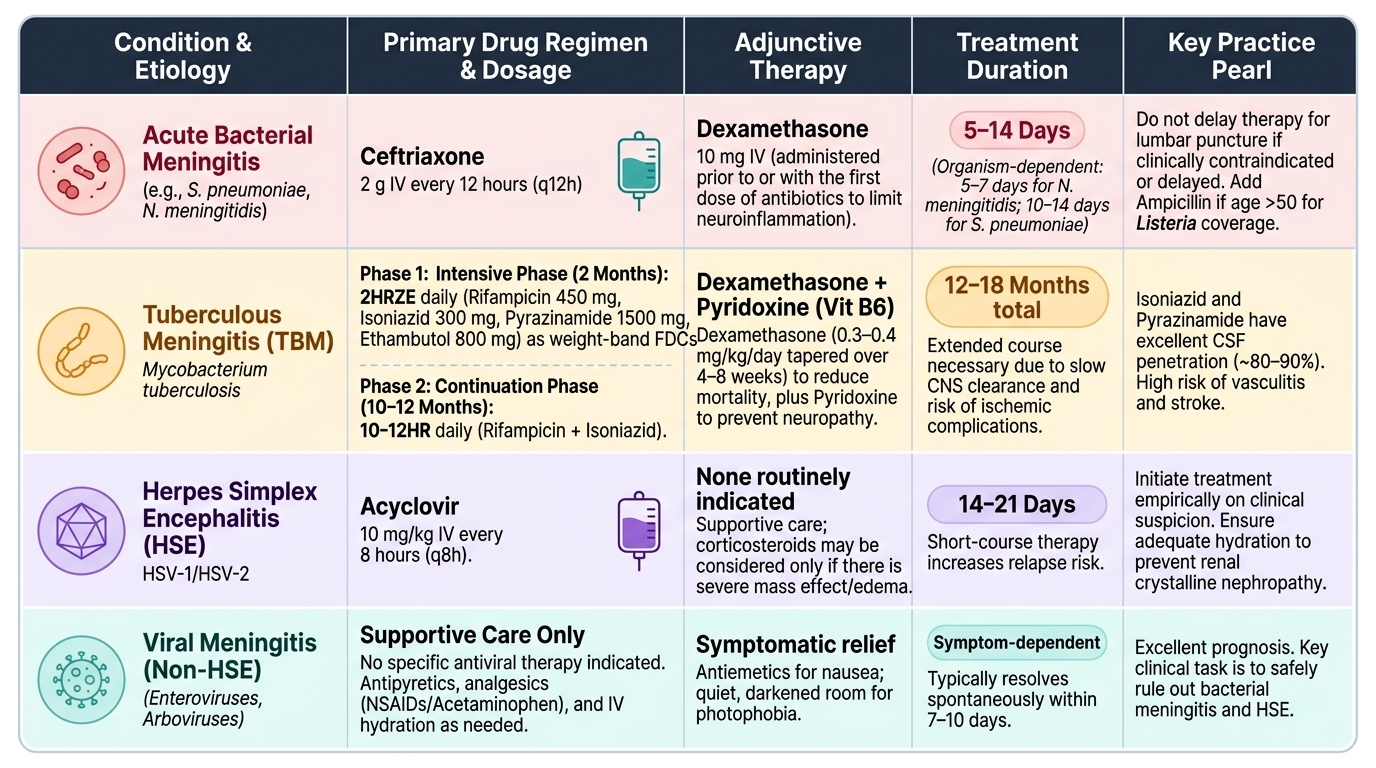
Tuberculous Meningitis (TBM) Drug Regimen:
The anti-TB treatment of TBM follows the NTEP (National TB Elimination Programme) guidelines — the same four drugs as pulmonary TB but with an extended duration because penetration into the CSF is variable across agents and the compartment is pharmacologically challenging. The regimen:
Intensive phase: 2HRZE — 2 months of Rifampicin (R) + Isoniazid (H) + Pyrazinamide (Z) + Ethambutol (E), all daily, as weight-band fixed-dose combinations (FDC) per NTEP dosing tables. Doses (for adult 50–69 kg): rifampicin 450 mg/day, isoniazid 300 mg/day, pyrazinamide 1500 mg/day, ethambutol 800 mg/day.
Continuation phase: 10–12HR — extended to 10–12 months of Rifampicin + Isoniazid daily (compared to 4 months for pulmonary TB). The extended duration is essential for TBM because: (1) mycobacteria are slower to be eliminated from the CNS; (2) the risk of relapse and drug resistance is higher in TBM; (3) the inflammatory phase with potential vasculitis and ischaemic complications persists for months. Total TBM duration: 12–18 months.
CSF penetration of individual TB drugs: Isoniazid penetrates CSF excellently (CSF:serum ratio ~80–90%); Pyrazinamide penetrates well (~90%); Rifampicin has moderate CSF penetration (~10–20%) but is bactericidal and essential; Ethambutol penetrates poorly into normal CSF (<10%) but better in inflamed meninges — included in the intensive phase for additive effect and to protect against resistance. This pharmacokinetic profile explains why isoniazid and pyrazinamide are the backbone of TBM treatment.
Adjunctive dexamethasone for TBM: Dexamethasone or prednisolone reduces mortality and severe disability in TBM — this is one of the most important evidence-based interventions in TBM management. Dexamethasone 0.3–0.4 mg/kg/day for 2–4 weeks, then tapered over 2–4 weeks (or a standard prednisolone 60 mg/day tapering schedule). Mechanism: reduces meningeal inflammation, cerebral oedema, vasculitis, and CSF outflow obstruction. Must be given to ALL patients with TBM regardless of severity.
Pyridoxine (vitamin B6): co-prescribed with isoniazid (10–25 mg/day) to prevent isoniazid-induced peripheral neuropathy, which occurs due to inhibition of pyridoxal phosphate synthesis by isoniazid competing with pyridoxal kinase.
Viral Meningitis and Herpes Simplex Encephalitis (HSE):
Most viral meningitis (enterovirus, HSV-2 — the most common cause of viral meningitis in adults) is self-limiting and does not require specific antiviral therapy. Management is supportive: analgesia, anti-emetics, adequate hydration, rest. Duration typically 5–10 days.
The critical exception is herpes simplex encephalitis (HSE) — caused predominantly by HSV-1, occasionally HSV-2. HSE is a neurological emergency with >70% mortality if untreated and significant neurological morbidity even with treatment. Clinical features: fever + headache + altered consciousness + focal neurological signs (particularly temporal lobe involvement — behavioural change, olfactory/gustatory hallucinations, amnesia, dysphasia, focal seizures). MRI: characteristic temporal lobe FLAIR/T2 signal change (unilateral or bilateral medial temporal, insular, and cingulate cortex involvement). CSF: lymphocytic pleocytosis, elevated protein, normal glucose; HSV PCR on CSF is diagnostic (sensitivity >95%).
Treatment: Acyclovir (aciclovir) 10 mg/kg IV every 8 hours (i.e., 30 mg/kg/day) for 14–21 days. Must be started empirically in any patient with features suggesting encephalitis while awaiting CSF HSV PCR — do not wait for PCR confirmation to start acyclovir if the clinical picture is consistent, because the neurological damage from delayed treatment is irreversible. Mechanism: acyclovir is phosphorylated by viral thymidine kinase to acyclovir triphosphate, which inhibits HSV DNA polymerase (chain termination). Adverse effects: nephrotoxicity (crystalline nephropathy at high doses — ensure adequate hydration, monitor renal function daily), neurotoxicity (delirium, encephalopathy — paradoxically rare), phlebitis at IV site.
SELF-CHECK
A 40-year-old immunocompetent man with fever, severe headache, confusion, and new-onset temporal lobe seizures is admitted. MRI shows bilateral temporal FLAIR signal change. CSF: lymphocytic pleocytosis, protein 110 mg/dL, glucose normal. HSV PCR is pending (result in 24 hours). What is the most appropriate immediate treatment?
A. Await HSV PCR result before starting any antiviral to avoid unnecessary drug exposure
B. Start oral acyclovir 400 mg five times daily — IV is not required for mild viral meningitis
C. Start IV acyclovir 10 mg/kg every 8 hours empirically while awaiting HSV PCR result
D. Start IV ceftriaxone + dexamethasone for presumed bacterial meningitis
Reveal Answer
Answer: C. Start IV acyclovir 10 mg/kg every 8 hours empirically while awaiting HSV PCR result
This is herpes simplex encephalitis (HSE) until proven otherwise: fever, confusion, temporal lobe seizures, bilateral temporal MRI signal change, lymphocytic pleocytosis with normal glucose in CSF — classic presentation. HSE has >70% mortality if untreated. IV acyclovir 10 mg/kg every 8 hours must be started empirically IMMEDIATELY, without waiting for HSV PCR confirmation. Every hour of delay in a conscious encephalitis patient risks irreversible neuronal death. Oral acyclovir does not achieve adequate CSF levels for HSE. Bacterial meningitis produces neutrophilic pleocytosis and low glucose — this pattern (lymphocytes, normal glucose) is viral. Starting ceftriaxone may be reasonable to cover bacterial meningitis empirically alongside acyclovir, but the primary intervention here is acyclovir.
Patient Counselling for Migraine and Tension-Type Headache
Patient counselling (IM17.14) is the competency that bridges pharmacological knowledge and clinical communication. A technically correct prescription that the patient does not understand, does not adhere to, or uses incorrectly is clinically ineffective. Counselling for migraine and tension-type headache covers four domains: lifestyle and trigger management, appropriate use of acute medications, education about preventive therapy, and recognition of red flags that require immediate medical attention.
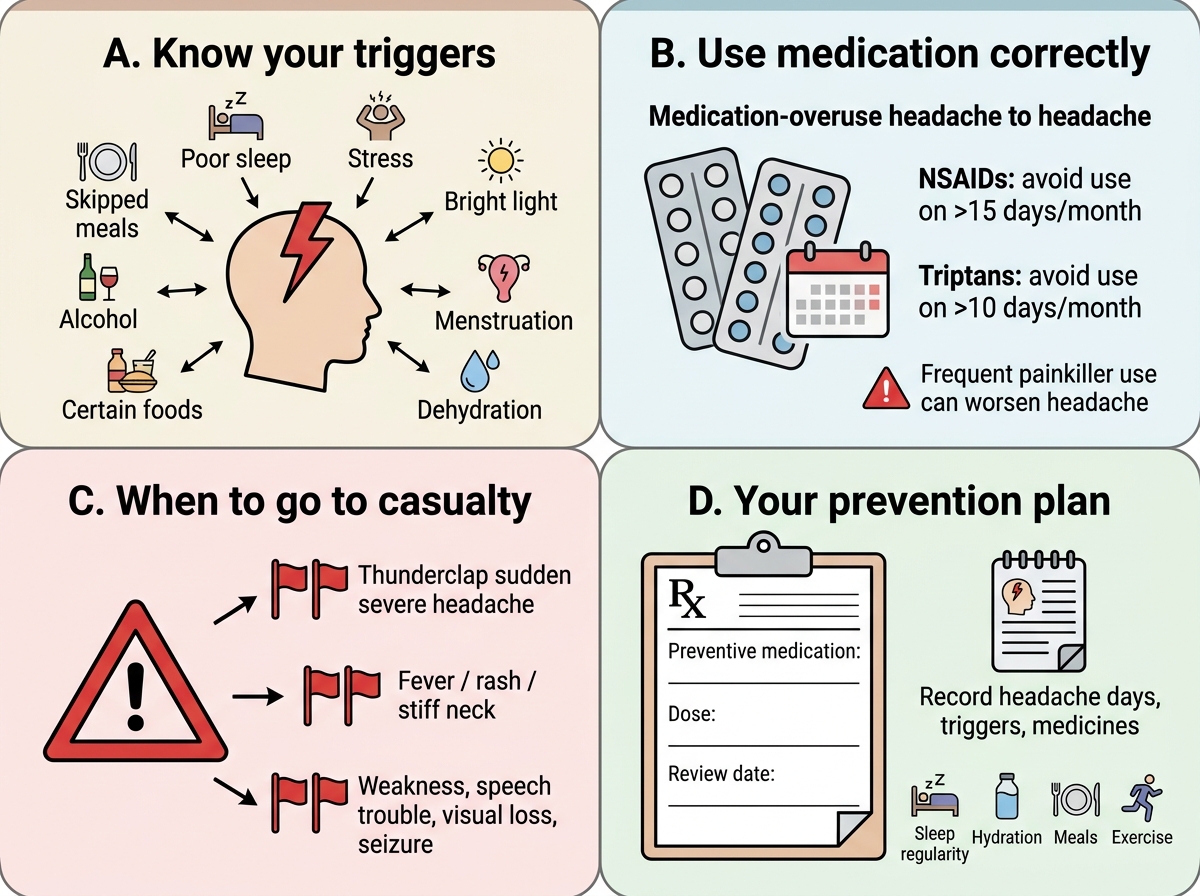
Counselling domain 1 — Migraine triggers and lifestyle modification: The single most cost-effective migraine intervention in resource-limited settings is trigger identification and avoidance. Key modifiable triggers include sleep disruption (both sleep deprivation and excessive sleep on weekends — 'weekend migraine'), skipping meals (hypoglycaemia), dehydration (particularly in hot weather), alcohol (especially red wine and beer — tyramine and histamine content), caffeine excess or withdrawal, physical or emotional stress, bright lights, strong smells, hormonal fluctuations (perimenstrual migraine), and certain foods (chocolate, aged cheese, processed meats — though evidence for specific food triggers is inconsistent). Counsel the patient to keep a headache diary (paper or app) recording: date and time of each attack, potential triggers, duration, severity, menstrual cycle, medications taken and their effect. A 2–3 month diary establishes patterns, identifies consistent triggers, and provides baseline attack frequency data for assessing preventive therapy efficacy.
Regular sleep, regular meals, regular exercise are the lifestyle pillars of migraine management. The 'regularity principle' — maintaining a consistent daily routine — is particularly important because migraine brains are sensitive to physiological perturbations. Aerobic exercise (30 minutes, 3–5 days per week) has evidence for reducing migraine frequency equivalent to topiramate in some studies, and does not have the adverse effect profile of medications.
Counselling domain 2 — Correct use of acute medications: The most important counselling message about acute medications is the risk of medication-overuse headache (MOH). Explain in plain language: 'When you take painkillers for headache more than 10–15 days per month, your brain adapts and actually starts producing more headaches to keep the painkiller level up. This is why taking more painkillers for more frequent headaches actually makes things worse over time — it is a trap, and the only way out is to reduce the painkiller use even though that is painful for 1–2 weeks.' The specific MOH thresholds to communicate: NSAIDs/paracetamol ≥15 days/month; triptans ≥10 days/month for >3 months. Counsel: treat attacks early (within 30 minutes of headache onset — late treatment when pain is severe is less effective and more likely to fail); use the most effective medication first (do not 'save the good medication' for really bad attacks — this strategy leads to escalating attacks); do not use acute medications more than 2 days per week.
Counselling domain 3 — Preventive therapy adherence: Preventive therapy fails most often due to: (a) patient discontinuation because of adverse effects in the first weeks before benefit is apparent; (b) inadequate dose titration (starting doses are sub-therapeutic); (c) lack of realistic expectations (50% reduction in attack frequency is success — elimination of all attacks is not the typical outcome). Counsel: 'This medicine will take 6–8 weeks to work. It may cause [specific side effects] at first, which usually improve. Please keep a headache diary so we can assess whether it is reducing your attacks after 3 months. Do not stop it without calling us — we may be able to adjust the dose.'
Counselling domain 4 — When to seek emergency care: Patients with established migraine are at risk of anchoring — attributing any new severe headache to migraine. Counsel about red flags that require immediate emergency attendance regardless of prior migraine history: 'If your headache comes on suddenly and reaches maximum pain within a minute — like being hit on the head — go to casualty immediately, even if it then improves. If your headache is accompanied by fever, stiff neck, a new rash, or confusion, go to casualty. If you have a new neurological symptom — weakness in a limb, speech difficulty, vision loss — that is new for you, go to casualty.'
Tension-type headache counselling specifics: TTH management emphasises non-pharmacological approaches more than migraine does. Physiotherapy for cervical muscle tension, biofeedback training, relaxation techniques (progressive muscle relaxation, diaphragmatic breathing), regular aerobic exercise, ergonomic assessment (workstation, posture, screen habits), and stress management are all evidence-based. Analgesic use should be limited to ≤14 days/month to avoid MOH. For chronic TTH, amitriptyline is the preventive of choice — counsel that it is being used for headache prevention at a low dose, not for depression, to avoid stigma-related non-adherence.
Migraine Patient Counselling Summary Card