Page 10 of 21
IM18.10-14 | Stroke Acute Management — SDL Guide
Learning Objectives
- Describe the initial supportive management of acute stroke — airway, oxygen, blood pressure targets (permissive hypertension vs pre-thrombolysis threshold vs ICH target), blood glucose, temperature, and swallowing assessment
- Describe IV thrombolysis for ischaemic stroke — alteplase and tenecteplase doses, the 4.5-hour window, the BP threshold of 185/110 mmHg, and absolute contraindications
- Explain the indications, eligibility criteria, and timing for mechanical thrombectomy, and the tandem thrombolysis-plus-thrombectomy strategy
- Describe the role of antiplatelet agents (aspirin monotherapy and DAPT) and anticoagulation timing in ischaemic stroke secondary prevention
- Describe the management of haemorrhagic stroke — BP target, anticoagulation reversal agents, ICP management, and the surgical indications for cerebellar ICH, IVH, and malignant MCA infarction
INSTRUCTIONS
This module is the most procedurally dense in the stroke cluster — it requires memorisation of specific doses (alteplase 0.9 mg/kg max 90 mg; tenecteplase 0.25 mg/kg max 25 mg), BP thresholds (185/110 pre-thrombolysis; 180/105 post-thrombolysis; 140 for ICH), and timing rules (4.5-hour thrombolysis window; 21-day DAPT for minor stroke; 1-3-6-12 rule for anticoagulation in AF). Use the summary table at the end as a revision card. The clinical cases are designed to test the integration of all these parameters simultaneously.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 427–428 — Treatment of Ischaemic and Haemorrhagic Stroke (textbook)
- AHA/ASA 2019 Guidelines for the Early Management of Patients with Acute Ischaemic Stroke (updated 2023 for tenecteplase) (guideline)
- AHA/ASA Guidelines for the Management of Spontaneous Intracerebral Haemorrhage, 2022 (guideline)
- API Textbook of Medicine, 10th ed. — Cerebrovascular Diseases (textbook)
- Indian Stroke Association Clinical Practice Guidelines, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 09:58 am. A 65-year-old hypertensive male arrived at your emergency department at 09:43 with left hemiplegia, left facial droop, and slurred speech. Last known well: 08:10 am. NIHSS = 14. NCCT brain was obtained at 09:52 and reported normal — no haemorrhage. CT angiography shows a hypodense (non-opacified) right M1 MCA. His blood pressure is 188/108 mmHg. Blood glucose is 9.2 mmol/L (166 mg/dL). His wife confirms he takes amlodipine 5 mg daily; no anticoagulants. It is now 09:58. You have 3.5 hours left in the thrombolysis window. The CT tech is still finishing the report. Your consultant is on the phone asking: 'Is he eligible? What's the blood pressure? Have you given the bolus?' The treatment decisions — thrombolysis eligibility, BP target, dose calculation, thrombectomy activation — must happen right now. Everything you have studied about stroke leads to this moment. This module gives you the complete management framework to act correctly under that pressure.
WHY THIS MATTERS
Acute stroke management is one of the most time-critical and consequential clinical skills in internal medicine. The NMC competencies IM18.10–IM18.14 require you to describe the initial supportive management of stroke, the use of thrombolytics with their indications and contraindications, the role of antiplatelets, and the management of haemorrhagic stroke including surgical indications — all at the KH level (Knowledge and clinical application). For the final-year student, this module bridges the pathophysiology and diagnostic knowledge from the earlier modules to real clinical decision-making. In India, where 85–90% of hospitals lack stroke units and many patients present to general medicine wards, the house surgeon and junior resident are often the first to make these decisions. Knowing precisely which patients get thrombolysis, which get thrombectomy, and how to manage blood pressure and complications in the acute phase is not theoretical knowledge — it is the difference between a patient who walks home and one who is permanently disabled.
RECALL
Before proceeding, activate the foundational knowledge from the earlier stroke modules. Recall that ischaemic stroke is caused by focal cerebral ischaemia; the penumbra (CBF 15–25 mL/100 g/min) is salvageable tissue surrounding the irreversible infarct core; the therapeutic goal is to restore flow to the penumbra before it dies. Recall the IV thrombolysis window: ≤4.5 hours from last known well for alteplase or tenecteplase. Recall that NCCT must be performed before thrombolysis to exclude haemorrhage — ICH on CT is an absolute contraindication. Recall that the blood pressure threshold for thrombolysis is <185/110 mmHg at the time of administration and must be maintained below 180/105 mmHg for 24 hours thereafter. Recall that haemorrhagic stroke requires a completely different approach — there is no reperfusion therapy; the goals are to halt haematoma expansion, control raised intracranial pressure, and reverse any coagulopathy. These foundational concepts are the skeleton onto which this management module adds the clinical detail.
Initial Supportive Management of Acute Stroke
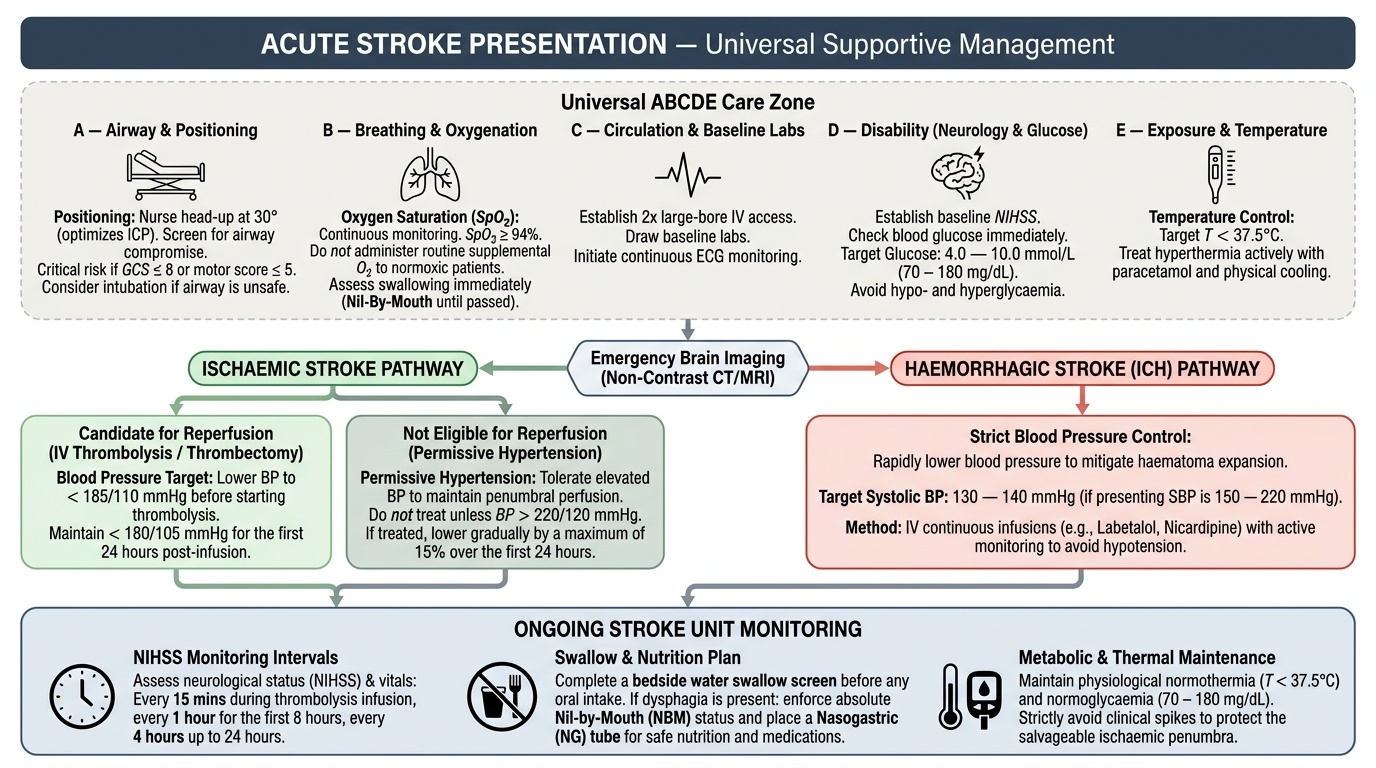
The initial supportive management of acute stroke applies universally to all stroke types — ischaemic and haemorrhagic — and runs in parallel with specific reperfusion or haemostatic therapies. It follows the ABCDE framework of emergency medicine and addresses the immediate physiological threats to brain viability: hypoxia, hypoglycaemia, hyperthermia, and extreme hypertension or hypotension. In a well-resourced stroke unit, these are managed systematically on arrival; in a general medical ward, the first-responding doctor must ensure each element is addressed before definitive treatment begins.
Provided image
A — Airway:
Maintain airway patency. Patients with a severely reduced conscious level (GCS ≤8 or GCS motor ≤5), those with bulbar palsy causing aspiration, and those with very large MCA infarcts at risk of cerebral oedema are at risk of airway compromise. Positioning: nurse in 30° head-up position (reduces ICP without reducing cerebral perfusion pressure excessively). Consider intubation and mechanical ventilation if GCS ≤8, airway is at risk, or SpO2 cannot be maintained ≥94% with supplemental oxygen. Supplemental oxygen is NOT routinely indicated for all stroke patients — the IST-3 trial and AHA guidelines do not support routine oxygen administration in normoxic patients. Give supplemental O2 only if SpO2 <94%.
B — Breathing and oxygenation:
Monitor SpO2 continuously. Treat hypoxia (SpO2 <94%) with supplemental oxygen by mask or nasal prongs. Aspiration pneumonia is a common early complication of stroke, particularly when there is bulbar palsy, dysarthria, or reduced consciousness. All stroke patients must have a swallowing assessment before any oral intake — a bedside water swallow test or formal speech therapy assessment; if dysphagia is identified, nil-by-mouth status, nasogastric tube for nutrition and medications.
C — Circulation and blood pressure:
Blood pressure management in acute stroke is one of the most nuanced aspects of initial management and differs between ischaemic and haemorrhagic stroke.
For ischaemic stroke without thrombolysis: the concept of permissive hypertension applies. In the acute phase, elevated blood pressure is a physiological response to maintain perfusion pressure to the ischaemic penumbra — the penumbra is a pressure-dependent zone, and lowering BP too aggressively reduces flow to this already-vulnerable tissue and expands the infarct. The AHA/ASA guidelines recommend NOT lowering blood pressure in the first 24–48 hours of acute ischaemic stroke unless it exceeds 220/120 mmHg (in which case a cautious 15% reduction is appropriate). There is no proven benefit to aggressive BP lowering in this phase.
For ischaemic stroke prior to thrombolysis: the BP must be lowered to <185/110 mmHg before alteplase or tenecteplase can be given. Agents used for this purpose include labetalol (10–20 mg IV, repeat after 10 minutes if needed; maximum 300 mg), nicardipine infusion (5 mg/hr, titrate upward), or clevidipine. Avoid sublingual nifedipine (unpredictable rapid drop). After thrombolysis, maintain BP <180/105 mmHg for 24 hours.
For haemorrhagic stroke (ICH): the target is systolic BP <140 mmHg, achieved within 1 hour of presentation, based on the INTERACT-2 and ATACH-2 trials. More aggressive reduction (SBP <120 mmHg) is harmful and should be avoided.
D — Disability (neurological status):
Document the NIHSS score on arrival and at regular intervals (1 hour, 6 hours, 24 hours). Monitor for neurological deterioration — worsening NIHSS or declining consciousness suggests haematoma expansion (ICH), cerebral oedema with herniation (large MCA infarct), recurrent stroke, or haemorrhagic transformation.
E — Blood glucose, temperature, and electrolytes:
Hyperglycaemia (blood glucose >10 mmol/L / 180 mg/dL) in the acute phase worsens infarct size and outcome — the mechanism is that high glucose fuels anaerobic metabolism in the penumbra, producing lactic acidosis and accelerating neuronal death. Target blood glucose 7.8–10 mmol/L (140–180 mg/dL) using insulin infusion if needed. Hypoglycaemia (glucose <3.5 mmol/L / 63 mg/dL) is a stroke mimic but also worsens outcome in actual stroke — correct with IV dextrose immediately. Hyperthermia (temperature >37.5°C) increases cerebral metabolic rate and worsens infarct — treat fever aggressively with paracetamol. Electrolytes: correct hyponatraemia and hypokalaemia which increase seizure risk.
Intravenous Thrombolysis — Indications, Contraindications, and Protocol
Intravenous thrombolysis with a tissue plasminogen activator (tPA) is the cornerstone of acute ischaemic stroke treatment and the most time-sensitive pharmacological intervention in internal medicine. The principle is straightforward: the thrombus occluding the cerebral artery is dissolved by activating plasminogen to plasmin, which degrades fibrin. The clinical impact is substantial — IV alteplase given within 3 hours improves functional outcomes by approximately 30% compared to placebo (NINDS trial, 1995); the benefit extends to 4.5 hours for selected patients (ECASS-3 trial, 2008). Every 15-minute reduction in door-to-needle time is associated with improved 3-month outcomes. The slogan 'time is brain' derives directly from this dose-response relationship between time to treatment and outcome. In India, tenecteplase has largely replaced alteplase in centres that routinely perform mechanical thrombectomy because its single-bolus dosing allows seamless transfer to the angiography suite without pausing an infusion — understanding both agents is therefore clinically relevant to the modern Indian physician.
Provided image
Thrombolytic agents currently used:
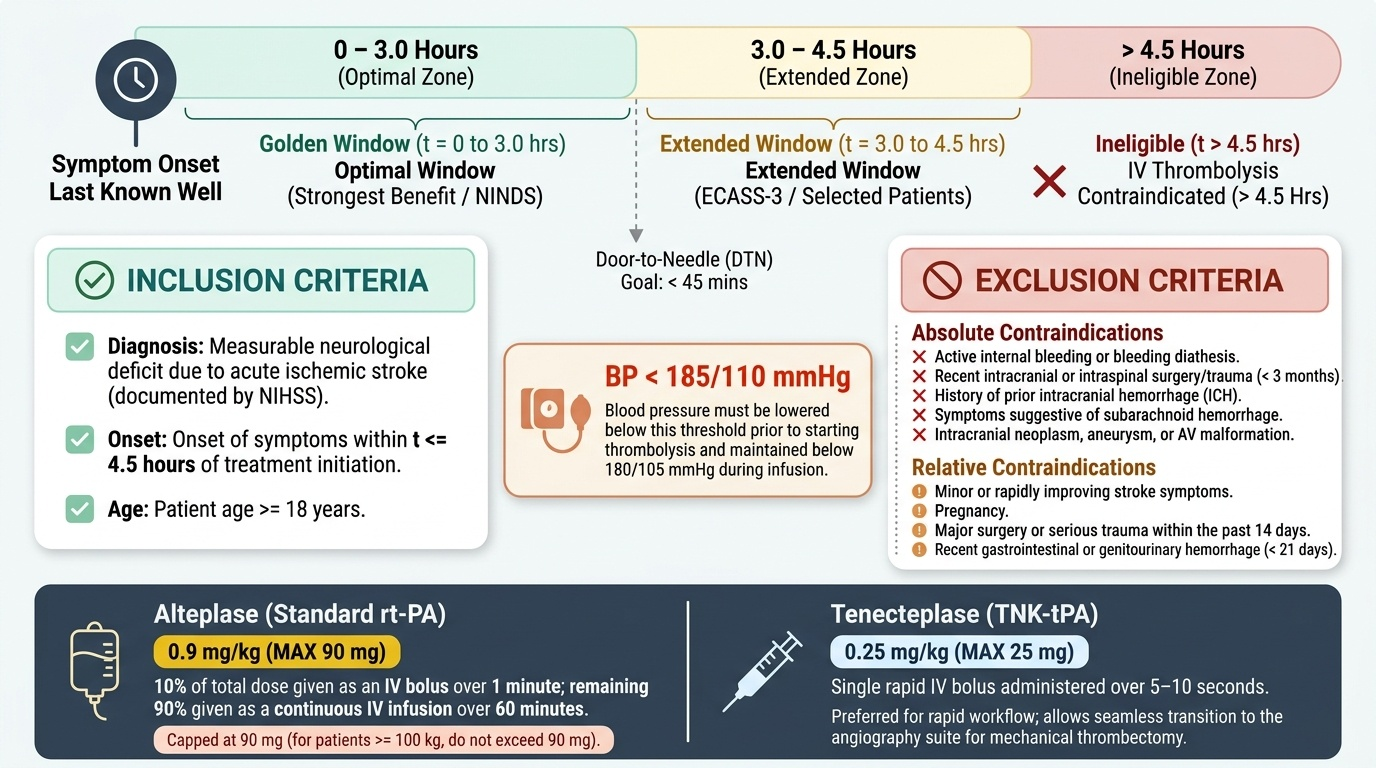
- Alteplase (rt-PA, recombinant tissue plasminogen activator): the original and most extensively studied agent. Dose: 0.9 mg/kg IV (maximum 90 mg); give 10% of the total dose as a bolus over 1 minute, then the remaining 90% as an infusion over 60 minutes. This is the standard dose — students and junior doctors must know this precisely. The maximum of 90 mg means a 100 kg patient receives 90 mg (not 0.9 × 100 = 90 mg by weight alone — the cap applies at 90 mg regardless of body weight above 100 kg).
- Tenecteplase (TNK-tPA): a genetically engineered variant of alteplase with a longer half-life (single IV bolus, not infusion), greater fibrin specificity, and resistance to plasminogen activator inhibitor. Dose: 0.25 mg/kg IV bolus (maximum 25 mg). Increasingly preferred in centres that offer mechanical thrombectomy because the single-bolus administration allows immediate transfer to the angiography suite. The AHA/ASA 2023 updated guidelines consider tenecteplase reasonable (class IIa) as an alternative to alteplase. It is simpler to administer and avoids 60-minute infusion monitoring.
Indications for IV thrombolysis:
- Ischaemic stroke with measurable neurological deficit (NIHSS ≥1 — but very minor isolated deficits may not be worth the haemorrhagic risk; clinical judgement required)
- Symptom onset (or last known well) within 4.5 hours
- NCCT brain: no haemorrhage, no established large infarct (ASPECTS ≥6)
- Blood pressure: <185/110 mmHg at the time of drug administration
- Blood glucose: >50 mg/dL and <400 mg/dL
- No absolute contraindication (see below)
Absolute contraindications to IV thrombolysis:
- Haemorrhage on NCCT brain
- Prior intracranial haemorrhage at any time
- Ischaemic stroke within the previous 3 months
- Major head trauma or intracranial surgery within 3 months
- Active internal bleeding (excluding menstruation)
- Arteriovenous malformation or known intracranial aneurysm
- Infective endocarditis (risk of mycotic aneurysm rupture)
- Aortic arch dissection (thrombolysis would extend the dissection)
- Blood glucose <50 or >400 mg/dL (check and correct first)
- INR >1.7 (warfarin); current therapeutic anticoagulation with heparin (APTT above normal); any DOAC taken within the last 48 hours (or positive anti-Xa or thrombin time)
- Platelet count <100,000/mm³
- NIHSS >25 (very large stroke — risk of haemorrhage high, benefit uncertain; relative contraindication)
Relative contraindications (risk-benefit discussion with senior):
- Minor, rapidly improving symptoms
- Seizure at onset with postictal neurological deficit (Todd's paresis — must be distinguished from stroke)
- Recent surgery (within 14 days) or serious trauma
- Pregnancy (thrombolysis has been used in life-threatening stroke in pregnancy; case-by-case)
- Recent MI within 3 months (potential cardiac tamponade risk with pericarditis)
Monitoring after thrombolysis:
After infusion, the patient requires intensive monitoring for 24 hours: neurological checks every 15 minutes for 2 hours, then hourly for 6 hours, then 2-hourly. BP monitoring: every 15 minutes during infusion, every 30 minutes for 6 hours post-infusion, then hourly. Stop the infusion and obtain urgent NCCT if any of: neurological deterioration, severe headache, acute hypertension (systolic >180 mmHg despite treatment), nausea/vomiting — these are warning signs of symptomatic intracranial haemorrhage (sICH), the most serious complication of thrombolysis, occurring in approximately 3–7% of treated patients.
SELF-CHECK
A 68-year-old woman has a left MCA ischaemic stroke. NIHSS = 10. Last known well 2.5 hours ago. NCCT: no haemorrhage, ASPECTS 8. Blood glucose 7.8 mmol/L (140 mg/dL). Her current BP is 192/106 mmHg. She takes warfarin for atrial fibrillation; her INR today is 1.4. Is she eligible for IV thrombolysis, and what is the immediate BP management?
A. Not eligible — INR 1.4 is an absolute contraindication to thrombolysis
B. Not eligible — she is in AF and therefore at too high a risk of haemorrhagic transformation
C. Eligible — lower BP to <185/110 mmHg with labetalol, then give alteplase 0.9 mg/kg (max 90 mg)
D. Eligible — thrombolysis can proceed immediately without BP treatment as she is within the window
Reveal Answer
Answer: C. Eligible — lower BP to <185/110 mmHg with labetalol, then give alteplase 0.9 mg/kg (max 90 mg)
INR 1.4 is below the threshold of 1.7 — it does not constitute a contraindication to thrombolysis (INR >1.7 is the cutoff). AF is not a contraindication to thrombolysis for ischaemic stroke — in fact, AF-related cardioembolic strokes are the target of thrombolysis in appropriate cases. The BP is 192/106 — this is above the 185/110 threshold required before alteplase can be given. The correct action is to lower BP to <185/110 with labetalol (10–20 mg IV) and then administer alteplase 0.9 mg/kg (max 90 mg; 10% as bolus, 90% over 60 minutes), provided BP remains below 185/110. Proceeding without BP treatment risks haemorrhagic transformation from uncontrolled hypertension during the thrombolytic state.
Mechanical Thrombectomy and Antiplatelet Therapy in Ischaemic Stroke
Beyond intravenous thrombolysis, two additional pillars of ischaemic stroke management must be understood: mechanical thrombectomy for proximal large vessel occlusion, and antiplatelet therapy for secondary prevention beginning in the acute phase. Together, these three treatments — IV thrombolysis, mechanical thrombectomy, and antiplatelet therapy — constitute the evidence-based pharmacological and interventional armamentarium for ischaemic stroke.
Mechanical thrombectomy (endovascular therapy):
Mechanical thrombectomy (MT) is the direct mechanical removal of the occluding thrombus from a proximal cerebral artery using a stent retriever or aspiration catheter, performed under fluoroscopic guidance in a neurointerventional suite. It has transformed outcomes for patients with large vessel occlusion: six landmark trials (MR CLEAN, ESCAPE, EXTEND-IA, SWIFT PRIME, THRACE, and others) demonstrated that MT + standard medical care achieves better functional outcomes at 3 months than standard medical care alone, with NNT of approximately 3–4 for an independent functional outcome. Eligibility criteria:
- Proximal large vessel occlusion: ICA terminus, M1 MCA (or selected M2), basilar artery — confirmed on CTA or MRA
- Time window: up to 6 hours from symptom onset (standard window); up to 24 hours with favourable penumbra-core mismatch on CT or MRI perfusion (DAWN and DEFUSE-3 trials — these select patients based on imaging, not just time)
- NIHSS ≥6 (modest or severe deficit — minor strokes generally do not benefit from the procedural risk)
- ASPECTS ≥6 (no large established infarct) — lower ASPECTS (≤5) is associated with higher haemorrhagic risk and lower benefit
- No absolute contraindications to arterial access or contrast
IV thrombolysis is NOT withheld if the patient is also a thrombectomy candidate — both are given (tandem strategy): thrombolysis first (immediately), then transfer for thrombectomy. Thrombolysis partially dissolves the thrombus, may rescue M2/M3 branches not accessible to the catheter, and does not delay thrombectomy preparation meaningfully.
Antiplatelet therapy in ischaemic stroke:
Aspirin (acetylsalicylic acid) is the cornerstone antiplatelet agent for ischaemic stroke. Its mechanism is irreversible inhibition of cyclooxygenase (COX-1), blocking thromboxane A2 synthesis and thereby inhibiting platelet aggregation. In acute ischaemic stroke:
- If thrombolysis was NOT given: aspirin 300 mg orally loading dose should be given within 48 hours of stroke onset — not immediately but after a repeat NCCT at 24 hours confirms no haemorrhagic transformation. The IST and CAST trials together (>40,000 patients) demonstrated that aspirin reduces early recurrent stroke risk and modestly improves functional outcome when started within 48 hours.
- If thrombolysis WAS given: do NOT give antiplatelets or anticoagulants for 24 hours after thrombolysis — risk of haemorrhagic transformation. Start antiplatelet at 24 hours after a repeat NCCT confirms no haemorrhagic transformation.
Dual antiplatelet therapy (DAPT) — aspirin + clopidogrel — is indicated for a 21-day course in two specific settings:
- Minor ischaemic stroke (NIHSS ≤3) or high-risk TIA (ABCD2 ≥4): the POINT and CHANCE trials demonstrated that DAPT (aspirin 75–300 mg + clopidogrel 300 mg loading dose, then 75 mg daily) started within 24 hours of minor stroke/TIA reduces 90-day recurrent stroke risk by approximately 25% compared to aspirin alone, without a significant increase in major bleeding. DAPT is continued for 21 days, then aspirin alone for long-term secondary prevention.
- After mechanical thrombectomy with stent placement (intracranial stenting): DAPT to prevent in-stent thrombosis.
Anticoagulation in ischaemic stroke:
Routine early anticoagulation (unfractionated heparin, LMWH, or DOACs) is NOT recommended for most acute ischaemic stroke patients due to the risk of haemorrhagic transformation outweighing the benefit of preventing early recurrence. The exception is AF-related cardioembolic stroke: anticoagulation is started after a delay based on infarct size — the '1-3-6-12 rule' (TIA = 1 day; minor stroke = 3 days; moderate stroke = 6 days; large stroke = 12 days before starting NOAC/warfarin) — after confirming on repeat NCCT that there is no haemorrhagic transformation. NOACs (apixaban, rivaroxaban, dabigatran) are preferred over warfarin for non-valvular AF. Warfarin with INR 2–3 remains the standard for valvular AF (rheumatic mitral stenosis, mechanical heart valve — for mechanical mitral valve, INR target 2.5–3.5).
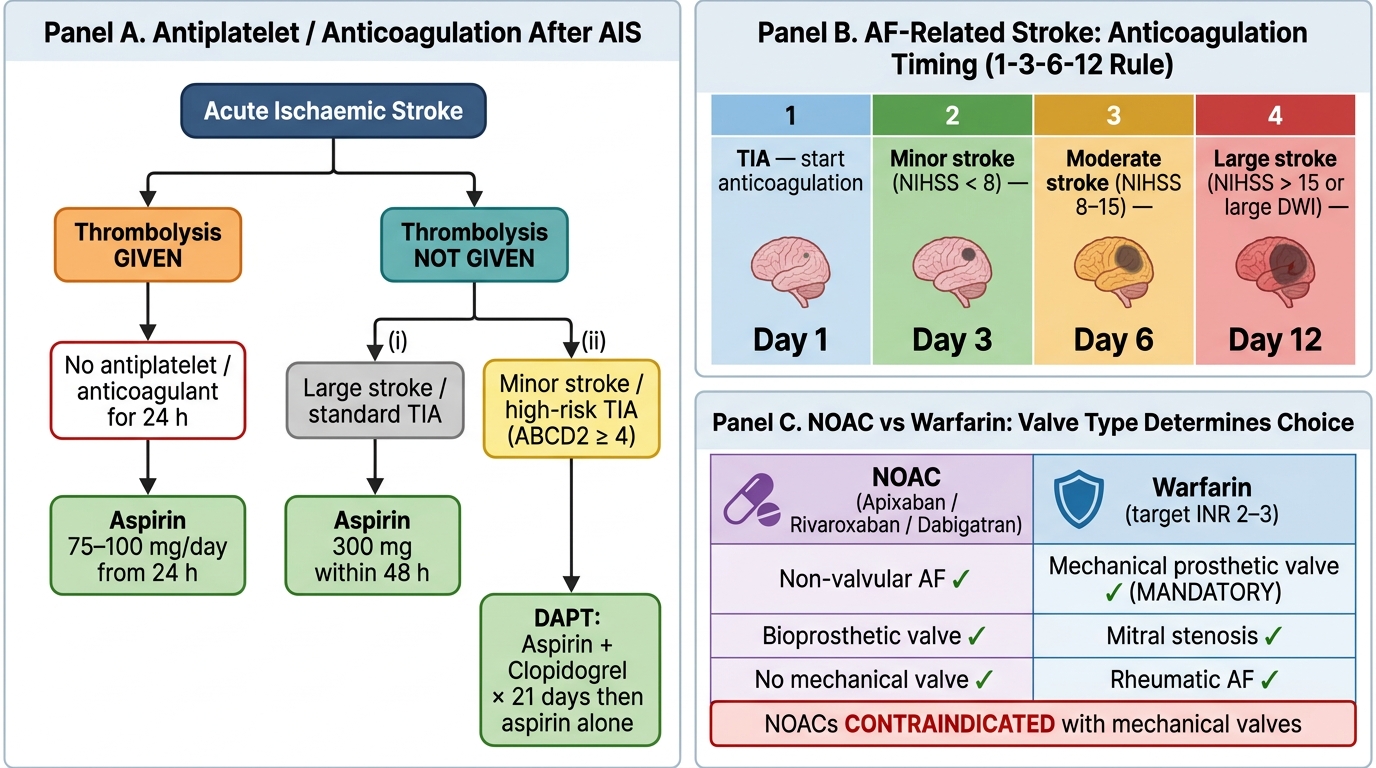
Antiplatelet & Anticoagulation Decision Tree in Acute Ischaemic Stroke