Page 11 of 21
IM18.10-14 | Stroke Acute Management — SDL Guide (Part 2)
Confirming Treatment Eligibility — The Stroke Triage Checklist
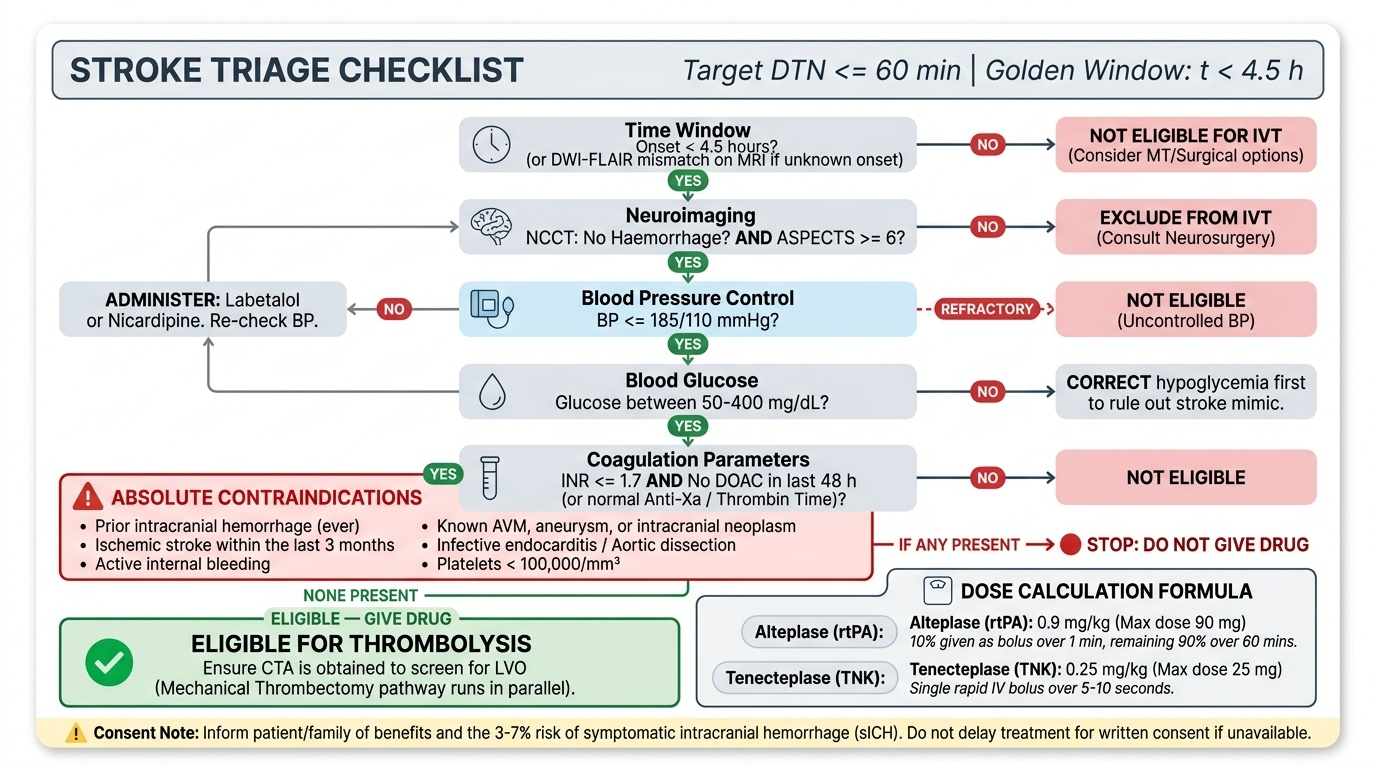
Before committing to any definitive stroke treatment — thrombolysis, mechanical thrombectomy, or surgical intervention — the clinician must confirm eligibility through a rapid but systematic triage checklist. This diagnostic triage step is distinct from the initial supportive management (arc step 1) and the pharmacological principles (arc step 2): it is the translation of those principles into a bedside decision for a specific patient. The entire process must be completed within the first 30–45 minutes of arrival for thrombolysis to be delivered within the golden window; in centres with direct transfer protocols, the target door-to-needle time is 60 minutes or less. A structured checklist prevents the most common errors — missed haemorrhage, uncontrolled BP at the time of drug administration, unrecognised anticoagulation — that lead to preventable harm.
Provided image
The pre-thrombolysis triage checklist (ischaemic stroke):
- Time: Is the patient within 4.5 hours of last known well? If wake-up stroke or unknown onset — is there a DWI-FLAIR mismatch on MRI (surrogate for onset ≤4.5 h)?
- Imaging: Has NCCT excluded haemorrhage? Is ASPECTS ≥6 (no large established infarct)? Has CTA been obtained to identify large vessel occlusion for thrombectomy decision?
- Blood pressure: Is BP <185/110 mmHg now? If not, has labetalol or nicardipine been given and is BP trending to target?
- Blood glucose: Is glucose between 50–400 mg/dL? Hypoglycaemia must be corrected before thrombolysis — it can mimic stroke and must be excluded as the cause.
- Coagulation: Has the INR been checked? Is it ≤1.7? Has the patient taken any DOAC in the last 48 hours? If yes — what is the anti-Xa or thrombin time result?
- Absolute contraindications: Run through the full list — prior ICH ever, stroke in last 3 months, active bleeding, AVM/aneurysm, endocarditis, aortic dissection, platelet count <100,000.
- Weight: Has the patient's weight been estimated for dose calculation? (0.9 mg/kg for alteplase; 0.25 mg/kg for tenecteplase)
- Consent: Has the patient or family been informed of the benefits and the 3–7% risk of symptomatic intracranial haemorrhage?
Large vessel occlusion triage (mechanical thrombectomy):
If CTA shows a proximal LVO (ICA, M1, basilar), the thrombectomy eligibility checklist runs in parallel:
- Time: Within 6 hours of onset? Or if beyond 6 hours, does the patient meet DAWN/DEFUSE-3 criteria — small infarct core on CT perfusion/DWI, large mismatch?
- Deficit severity: NIHSS ≥6 (minor strokes generally do not warrant procedural risk)?
- ASPECTS: ≥6 (large established infarct = less to save, more haemorrhagic risk)?
- Functional status: Was the patient functionally independent before the stroke (mRS 0–1)?
- Access: Is an interventional neuroradiology suite available? Has the on-call neurointerventional team been activated?
ICH triage — confirming the diagnosis and severity:
For haemorrhagic stroke, the triage is different — there is no drug to give, but there are decisions to make urgently:
- Is this hypertensive ICH, or is there a structural lesion (AVM, aneurysm, tumour) requiring specific treatment? CTA or DSA is needed if the patient is young, normotensive, or the haematoma is in an atypical location.
- Is there intraventricular extension? If yes — neurosurgery review for EVD.
- Is the patient on anticoagulants? Which agent? Reversal agent must be available and given within minutes.
- What is the haematoma volume (ABC/2)? This determines prognosis and guides surgical consultation.
- What is the GCS? Rapidly declining consciousness requires immediate anaesthesia and airway management.
SELF-CHECK
A 72-year-old man presents with acute ischaemic stroke. NIHSS = 14. He is 90 minutes from last known well, has no haemorrhage on CT, and receives IV alteplase successfully. No large vessel occlusion is seen on CTA. His ECG 2 hours later shows new AF. At 24 hours, repeat CT shows no haemorrhagic transformation. What antiplatelet and anticoagulation strategy should be initiated?
A. Start aspirin 300 mg immediately after confirming no haemorrhage on CT
B. Start aspirin 300 mg at 24 hours after repeat CT; delay anticoagulation for 6 days given moderate stroke (NIHSS 14), then start NOAC for AF
C. Start dual antiplatelet (aspirin + clopidogrel) for 21 days
D. Start unfractionated heparin at 24 hours to prevent early recurrence from AF
Reveal Answer
Answer: B. Start aspirin 300 mg at 24 hours after repeat CT; delay anticoagulation for 6 days given moderate stroke (NIHSS 14), then start NOAC for AF
After thrombolysis, antiplatelets are withheld for 24 hours. At 24 hours, repeat CT confirms no haemorrhagic transformation, so aspirin 300 mg can be started. The new AF is the cause of the cardioembolic stroke — long-term anticoagulation with a NOAC is mandatory for secondary prevention. However, immediate anticoagulation after a moderate stroke (NIHSS 14) risks haemorrhagic transformation. The '1-3-6-12 rule' based on stroke severity recommends: minor stroke (NIHSS <5) = 3 days; moderate stroke (NIHSS 5–15) = 6 days; large stroke (NIHSS >15) = 12 days. With NIHSS 14, anticoagulation is generally started at 6 days after confirming no haemorrhagic transformation on repeat imaging. DAPT is appropriate for minor stroke/TIA, not for a moderate stroke with a known AF source. Heparin is not routinely used for acute ischaemic stroke.
Management of Haemorrhagic Stroke
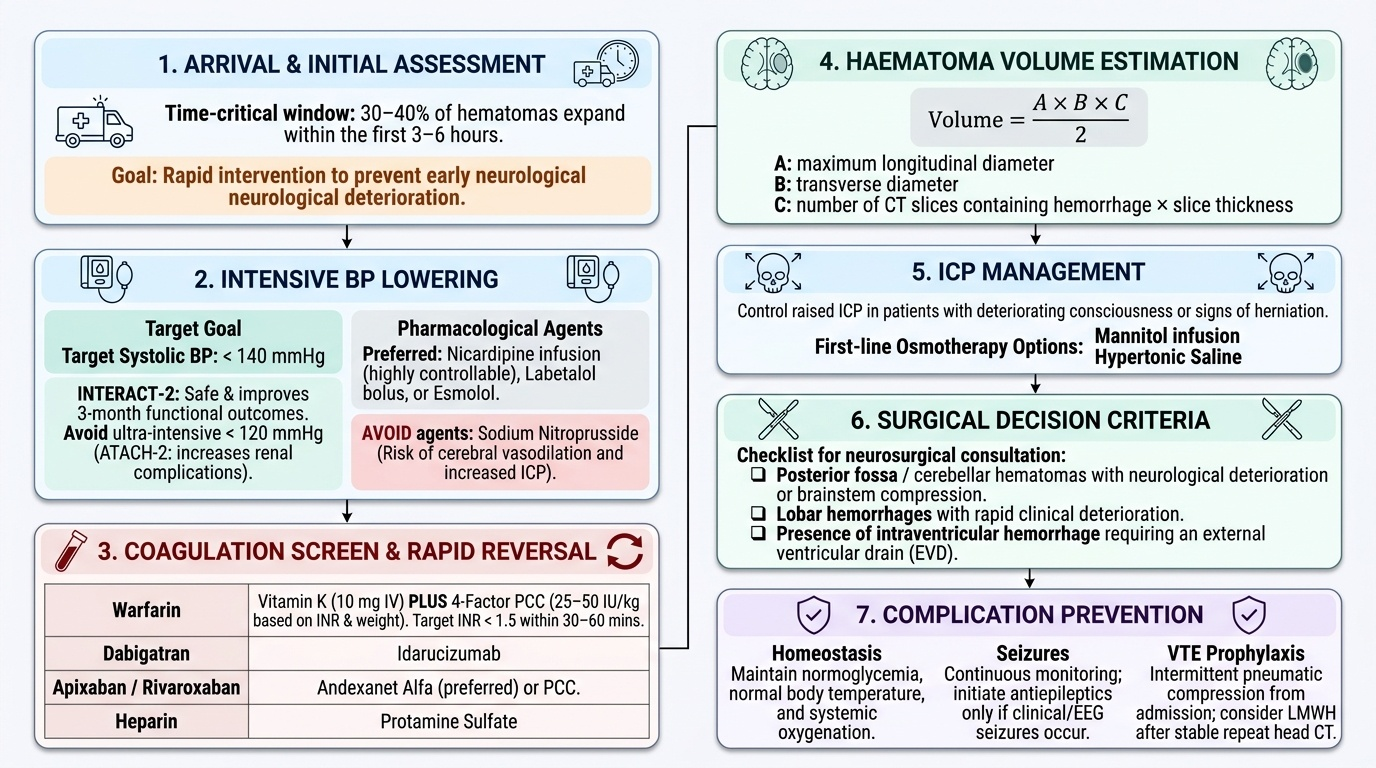
Haemorrhagic stroke — intracerebral haemorrhage (ICH) and subarachnoid haemorrhage (SAH) — carries a higher early mortality than ischaemic stroke and requires a fundamentally different management approach. There is no reperfusion therapy in ICH; the management goals are to stop haematoma expansion, control raised intracranial pressure, reverse any coagulopathy, maintain systemic homeostasis, and identify any underlying structural cause requiring surgical treatment. The first hour of ICH management is as time-critical as the first hour of ischaemic stroke treatment, for a different reason: approximately 30–40% of haematomas expand in the first 3–6 hours, and haematoma expansion is the most important driver of early neurological deterioration and 30-day mortality.
Provided image
Blood pressure management in ICH:
Acute severe hypertension in ICH drives haematoma expansion and must be treated promptly. The evidence from the INTERACT-2 (2013) and ATACH-2 (2016) trials establishes: target systolic BP <140 mmHg, achieved within 1 hour of presentation. The INTERACT-2 trial showed that intensive BP lowering (target <140 mmHg) was safe and associated with improved functional outcome at 3 months. The ATACH-2 trial showed that ultra-intensive lowering (target <120 mmHg) was not beneficial and may increase renal complications — so the target remains <140 mmHg, not lower. Agents used: nicardipine infusion (preferred for controllability), labetalol bolus, or esmolol. Avoid sodium nitroprusside (can increase ICP by cerebral vasodilation).
Reversal of anticoagulation:
For anticoagulant-related ICH, rapid reversal of anticoagulation is the highest priority. The specific reversal agent depends on the anticoagulant:
- Warfarin (INR elevated): vitamin K 10 mg IV (takes 12–24 hours to work — inadequate as sole agent in emergency) PLUS 4-factor prothrombin complex concentrate (4F-PCC) at a dose based on the INR and body weight (e.g., 25–50 IU/kg). Target: INR <1.5 within 30–60 minutes. PCC is preferred over fresh frozen plasma (FFP) because it achieves faster reversal and requires far less volume.
- Dabigatran (direct thrombin inhibitor): idarucizumab (Praxbind) — a specific humanised antibody that reverses dabigatran within minutes; dose 5 g IV in two 2.5 g boluses.
- Factor Xa inhibitors (apixaban, rivaroxaban, edoxaban): andexanet alfa (specific reversal agent, not universally available) or 4F-PCC as an off-label alternative (used where andexanet alfa is unavailable — common in India).
- Unfractionated heparin: protamine sulphate (1 mg per 100 units of heparin in last dose, max 50 mg IV over 10 minutes).
- LMWH: protamine sulphate (partially reverses LMWH — 1 mg per 1 mg enoxaparin given in last 8 hours; maximum reversal ~60–70%).
Haematoma volume and management intensity:
Haematoma volume is calculated by the ABC/2 formula on CT: A (greatest diameter on axial image) × B (greatest perpendicular diameter) × C (number of slices × slice thickness) ÷ 2. Haematoma volume correlates directly with 30-day mortality: volume >30 mL carries 70% 30-day mortality; >60 mL virtually universally fatal without surgery. The relationship between haematoma volume and neurological deficit allows prognosis to be communicated to the family.
Managing raised intracranial pressure (ICP):
In large ICH with signs of raised ICP (worsening consciousness, Cushing's triad — hypertension, bradycardia, irregular breathing) or herniation:
- Head of bed elevated 30°
- Hyperventilation (target pCO2 35 mmHg) — short-term, temporising measure
- Osmotherapy: mannitol 20% solution 0.5–1 g/kg IV over 15–20 minutes, or hypertonic saline (3%–23.4%) — both draw fluid from brain parenchyma by osmotic gradient; hypertonic saline is preferred if hypotension is present (mannitol is an osmotic diuretic and can reduce BP)
- Dexamethasone: NOT indicated in ICH (unlike brain tumour oedema) — no benefit and increases infection/hyperglycaemia risk
- CSF drainage via external ventricular drain (EVD): if intraventricular haemorrhage causing obstructive hydrocephalus — a neurosurgical emergency
Prevention of complications:
- Seizure prophylaxis: routine prophylaxis is NOT recommended; treat seizures if they occur with IV benzodiazepines followed by levetiracetam or valproate
- DVT prophylaxis: intermittent pneumatic compression from admission; LMWH can be started at 48–72 hours in ischaemic stroke after confirming no haemorrhagic transformation; in ICH, LMWH is generally started at 48 hours after haematoma stability confirmed on imaging
- Dysphagia: formal swallowing assessment before any oral intake; enteral nutrition via NGT if unable to swallow safely
SELF-CHECK
A 75-year-old woman on warfarin (INR 3.8) for a mechanical mitral valve presents with acute ICH. Haematoma volume is 18 mL in the right thalamus. Her GCS is 12/15. What is the MOST APPROPRIATE immediate management of her anticoagulation?
A. Vitamin K 10 mg IV alone — sufficient for emergency reversal
B. Withhold warfarin and observe; reversal is not needed unless INR >5
C. Vitamin K 10 mg IV PLUS 4-factor prothrombin complex concentrate (4F-PCC) to target INR <1.5 within 30–60 minutes
D. Fresh frozen plasma (FFP) alone — PCC is not indicated because she has a mechanical valve
Reveal Answer
Answer: C. Vitamin K 10 mg IV PLUS 4-factor prothrombin complex concentrate (4F-PCC) to target INR <1.5 within 30–60 minutes
Anticoagulant-related ICH (INR 3.8 on warfarin) requires urgent and complete reversal of anticoagulation to prevent haematoma expansion. Vitamin K alone is insufficient in the acute setting because its effect requires 12–24 hours (hepatic synthesis of clotting factors). 4F-PCC provides immediate restoration of clotting factors II, VII, IX, and X within 30–60 minutes and is the preferred agent for emergency warfarin reversal. Vitamin K is given concurrently to provide a sustained effect. The INR target is <1.5. Mechanical valve status does not change the need for reversal in an acute ICH — the life-threatening haemorrhage takes priority over thrombotic risk (which can be managed with careful anticoagulation resumption 4–8 weeks later). FFP achieves reversal but requires 10–15 mL/kg volume (risk of fluid overload and slower INR correction) — PCC is superior.
Surgical Indications in Haemorrhagic Stroke
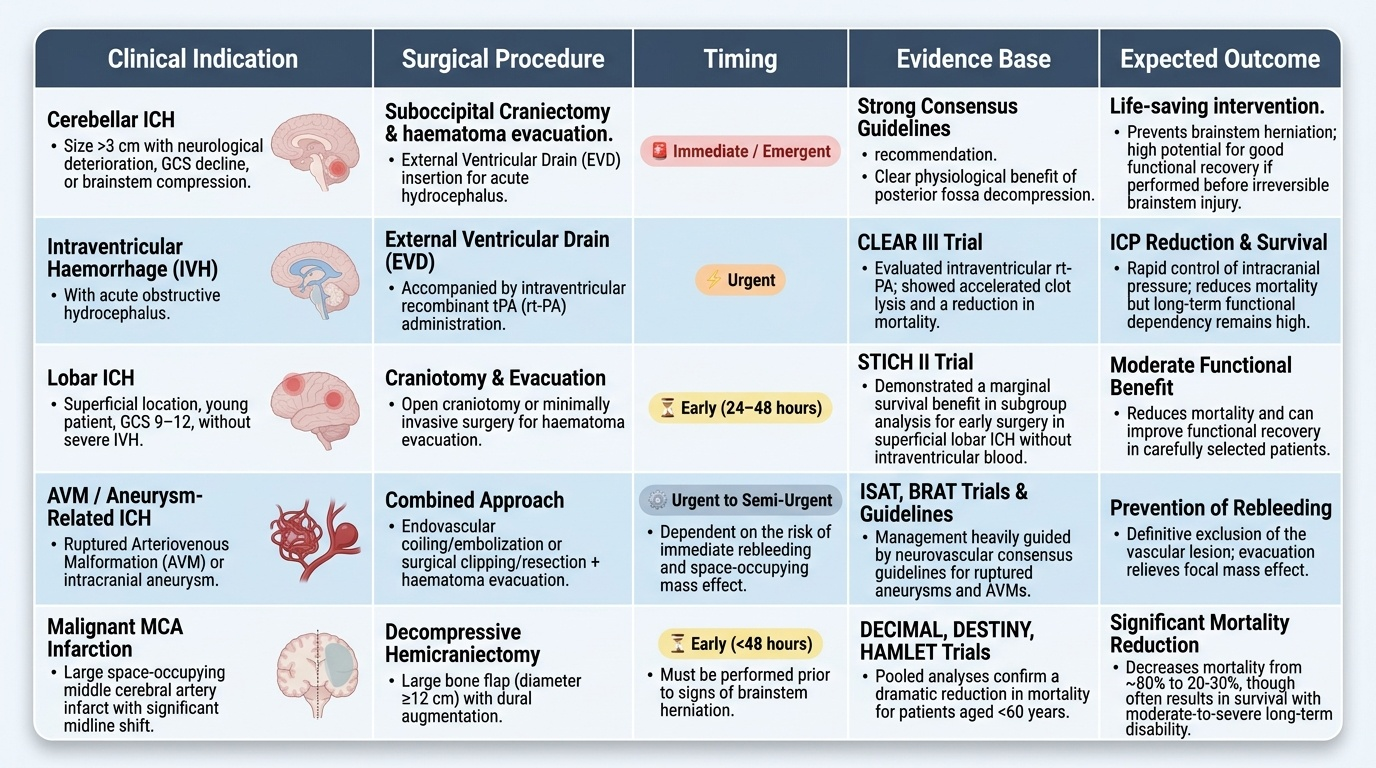
Surgical intervention in haemorrhagic stroke remains highly selective and is guided by a careful weighing of the haematoma's anatomical location, volume, the patient's neurological grade, age, and comorbidities. The landmark STICH-I and STICH-II trials of craniotomy for supratentorial ICH failed to show a clear benefit of early surgical haematoma evacuation over conservative management for most patients, limiting the role of surgery to specific indications where the risk-benefit ratio shifts decisively in favour of intervention. This means that the default posture for most supratentorial ICH — putaminal, thalamic, pontine — is careful medical management, not surgery. The clinician's task is to recognise the specific anatomical and clinical circumstances that represent exceptions to this rule and to escalate urgently when those conditions are met. Understanding these indications — and the reasoning behind them — is the knowledge required at the IM18.14 competency level (K — awareness level, not requiring clinical performance).
Provided image
Established indications for surgical intervention in ICH:
- Cerebellar ICH with neurological deterioration, brainstem compression, or haematoma >3 cm: cerebellar ICH is a clear exception to the general rule of medical management. The cerebellum lies in the posterior fossa, a confined space — even moderate-volume cerebellar haematomas can compress the fourth ventricle (causing obstructive hydrocephalus) and the brainstem (causing life-threatening cardiorespiratory compromise). Suboccipital craniectomy with evacuation of the cerebellar haematoma is life-saving. This is the most well-established surgical indication in ICH. Haematoma >3 cm and/or obstructive hydrocephalus are thresholds commonly used; deteriorating GCS is the clinical trigger. An external ventricular drain (EVD) may be placed as a temporising measure while surgical planning proceeds.
- Obstructive hydrocephalus from intraventricular haemorrhage (IVH): blood entering the ventricles (IVH) can obstruct CSF drainage at the third or fourth ventricle, causing acute obstructive hydrocephalus with rising ICP. An external ventricular drain (EVD) provides immediate drainage. Intraventricular recombinant tPA (rt-PA via the EVD — CLEAR III trial) can accelerate clot lysis within the ventricles and may reduce death and disability.
- Lobar ICH in young patients (age <45) with accessible haematoma and deteriorating consciousness (GCS 9–12): in selected young patients with a surgically accessible lobar haematoma (near the cortical surface, not deep thalamic or capsular where surgical access causes excessive damage), haematoma evacuation may be considered if the patient is deteriorating despite maximal medical treatment. The STICH-I post-hoc analysis showed a marginal benefit of surgery for superficial lobar haematoma within 1 cm of the cortical surface.
- Structural lesion causing ICH (AVM, aneurysm, tumour): if the ICH is caused by a ruptured AVM or aneurysm (identified on CTA or DSA), surgical or endovascular treatment of the underlying lesion is definitive — both to treat the haematoma and prevent rebleeding. Similarly, haemorrhage into a brain tumour may require surgical excision once the acute phase has stabilised.
- Decompressive craniectomy for malignant MCA infarction: although technically a procedure for ischaemic stroke, decompressive hemicraniectomy (removal of part of the skull to allow the oedematous brain to expand) is life-saving in malignant MCA infarction — a large MCA territory infarct (>145 cm³ on DWI, clinical signs of ICP) causing transtentorial herniation, occurring predominantly in patients under 60 years. The DESTINY, DECIMAL, and HAMLET trials showed that decompressive hemicraniectomy within 48 hours reduces mortality from ~80% to 22% in patients under 60; however, it increases the proportion surviving with severe disability, and informed consent regarding the expected level of disability is mandatory.
Where surgery is NOT indicated in ICH:
- Deep supratentorial ICH (putaminal, thalamic, pontine) in the absence of hydrocephalus or mass effect with herniation: STICH-I and STICH-II showed no benefit of early craniotomy for these locations.
- Patients with very large haematomas (>60 mL) and deep coma (GCS ≤5) where the prognosis is so poor that surgery will not meaningfully change outcome.
- Pontine haemorrhage: surgical access to the pons is not feasible; conservative management only.
CLINICAL PEARL
The most important BP threshold in stroke management is 185/110 mmHg — the ceiling for safe IV thrombolysis. Above this, the risk of haemorrhagic transformation from the thrombolytic agent on an unprotected hypertensive vessel wall is unacceptably high. The target after thrombolysis is <180/105 mmHg for 24 hours. Many students confuse this with the permissive hypertension threshold for ischaemic stroke without thrombolysis (≤220/120 mmHg, where BP is left alone) — these are different thresholds for different clinical situations.
A second pearl: cerebellar ICH is surgically different from all other ICH locations. While deep supratentorial ICH (putamen, thalamus, pons) is managed conservatively in most cases (STICH trials), cerebellar ICH >3 cm or with neurological deterioration is a neurosurgical emergency — suboccipital craniectomy. The posterior fossa is a confined space; a 3 cm cerebellar haematoma compresses the fourth ventricle and kills the patient from brainstem herniation far faster than a 3 cm putaminal haematoma. Never apply the general 'conserve' rule to cerebellar ICH.
Self-Assessment: Integrating Stroke Acute Management
The acute management of stroke requires integrating the clinical diagnosis (ischaemic vs haemorrhagic), the imaging results (NCCT, CTA, ASPECTS), the patient-specific eligibility assessment (blood pressure, INR, contraindications), and the treatment protocol (thrombolysis dose, BP target, antiplatelet timing, surgical decision) into a single rapid management plan. The scenarios below are at the level expected in your final MBBS examination and early internship clinical practice.
Scenario A: A 58-year-old hypertensive male presents with acute right hemiplegia at 11:20. Last known well 10:45. NIHSS = 16. NCCT: no haemorrhage, ASPECTS 9. CTA: left M1 MCA occlusion. BP 200/116 mmHg. Blood glucose 8.0 mmol/L. No anticoagulant use. INR 1.1. What is the management plan?
Analysis: Time from LKW = 35 minutes. Well within 4.5-hour thrombolysis window AND 6-hour mechanical thrombectomy window. Both are indicated. Immediate action: labetalol 10–20 mg IV to lower BP to <185/110 mmHg. Once BP controlled (<185/110): give tenecteplase 0.25 mg/kg IV bolus (max 25 mg) — or alteplase 0.9 mg/kg (max 90 mg; 10% bolus, 90% over 60 min). Simultaneously: activate thrombectomy team, transfer to angiography suite immediately after thrombolysis bolus. NIHSS = 16 (severe stroke), ASPECTS 9 (minimal established infarct), M1 occlusion — highly favourable thrombectomy candidate. Antiplatelet: do NOT give for 24 hours post-thrombolysis. After 24h repeat CT: start aspirin 300 mg if no haemorrhagic transformation. Cardiac monitoring (Holter 24h) for AF detection.
Scenario B: A 80-year-old man presents at 3 am with sudden-onset severe headache (worst of his life) and neck stiffness. He was found by his wife. GCS = 12. NCCT: hyperdensity in the basal cisterns and sylvian fissures. CT angiography: 7 mm aneurysm at the AComm–ACA junction. What is the diagnosis and immediate management?
Analysis: Subarachnoid haemorrhage (basal cisterns + sylvian fissures = blood in subarachnoid space) from ruptured AComm aneurysm. Immediate management: protect airway (GCS 12, at risk — anaesthesia review), BP target SBP <160 mmHg (to prevent rebleeding before definitive aneurysm treatment), nimodipine 60 mg oral every 4 hours (calcium channel blocker — reduces cerebral vasospasm), maintain euvolaemia, urgent neurosurgery/neurointerventional review for aneurysm securing (coiling preferred in most centres — ISAT trial; clipping if anatomy unfavourable). No thrombolysis. No antiplatelet. No anticoagulant.
Scenario C: A 55-year-old hypertensive male has sudden right-sided weakness and headache. NCCT: 40 mL ICH in the right putamen with intraventricular extension. GCS = 10. BP 198/112 mmHg. No anticoagulant use. Coagulation screen: normal. What is the management?
Analysis: Large hypertensive putaminal ICH with IVH. No anticoagulant reversal needed (coags normal). BP: target SBP <140 mmHg — nicardipine infusion. GCS 10 + intraventricular extension → neurosurgery review for external ventricular drain (obstructive hydrocephalus risk). Putaminal location — NOT a candidate for haematoma evacuation (deep supratentorial; STICH evidence). Medical management: manage ICP (mannitol if signs of herniation), prevent complications (VTE prophylaxis with pneumatic compression from admission, LMWH at 48 hours after haematoma stability confirmed, swallowing assessment, enteral nutrition). Prognosis: haematoma volume 40 mL = approximately 50% 30-day mortality; counsel family accordingly.
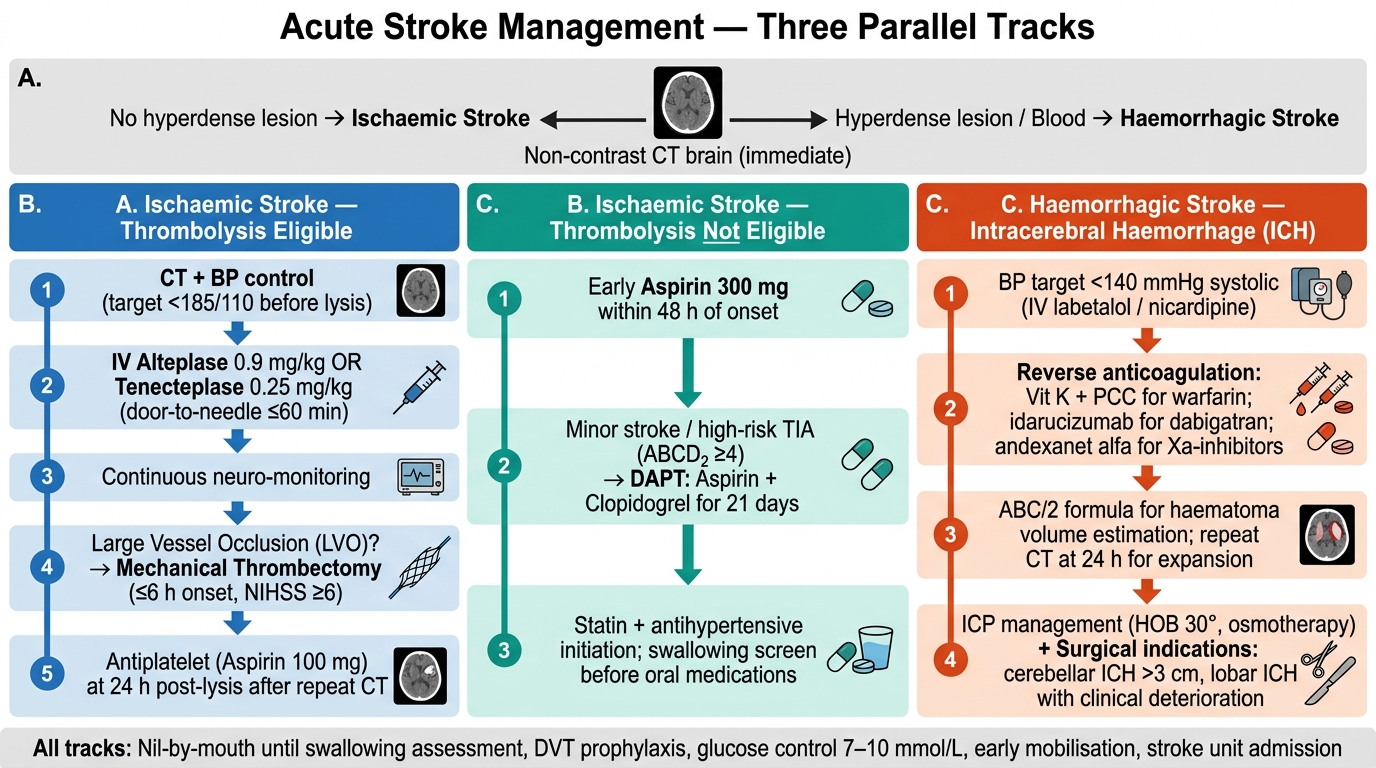
Acute Stroke Management — Three Parallel Treatment Tracks