Page 13 of 21
IM18.15-16 | Stroke Rehabilitation and Counselling — SDL Guide
Learning Objectives
- Enumerate and describe the indications for multidisciplinary rehabilitation after stroke, mapped to specific neurological deficits — motor, language, swallowing, cognitive, psychosocial
- Describe the roles and key techniques of physiotherapy, speech and language therapy, occupational therapy, neuropsychology, and social work in post-stroke rehabilitation
- Outline the three phases of stroke rehabilitation — acute, sub-acute, and community — with the goals and intensity appropriate to each phase
- Communicate prognosis after stroke to patients and families using an evidence-based framework and empathetic language (SPIKES protocol)
- Counsel patients on specific post-stroke issues: return to driving, depression, secondary prevention, sexual function, post-stroke epilepsy, and carer support
INSTRUCTIONS
This module is the most interpersonally demanding in the stroke cluster — it requires you to practise both the clinical knowledge of rehabilitation modalities and the communication skills of prognostic counselling. Do not skip the scenarios: they are the best preparation for real post-stroke outpatient consultations. The SPIKES protocol is worth memorising as a scaffold for difficult conversations. The 'post-stroke review checklist' in arc step 5 is a practical tool you should be able to reproduce from memory for your internship year.
References
- AHA/ASA 2016 Guidelines for Adult Stroke Rehabilitation and Recovery (guideline)
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 427 — Cerebrovascular Diseases (rehabilitation section) (textbook)
- API Textbook of Medicine, 10th ed. — Stroke Rehabilitation (textbook)
- RESTART Collaboration 2019 — Restart or stop antithrombotics randomised trial after intracranial bleeding (Lancet) (guideline)
- Indian Stroke Association Clinical Practice Guidelines, 2020 — Rehabilitation and Secondary Prevention (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mr Rajan Pillai, a 58-year-old retired teacher, had an acute left MCA ischaemic stroke three weeks ago. He received thrombolysis and made a partial recovery. He is now sitting in your outpatient clinic in a wheelchair. His wife is next to him. His right arm hangs at his side — dense hemiplegia. His speech is slow and effortful, but he understands every word you say — Broca's aphasia. His wife says: 'Doctor, will he ever walk again? Will he speak properly? He used to be so active. He is depressed — he doesn't want to eat. Should we put him in a home? Is there anything you can do?' Mr Pillai is watching you. He can hear everything. He cannot easily express what he wants to say, but his eyes tell you he needs an honest, humane, and hopeful answer. Everything in this module prepares you to give it.
WHY THIS MATTERS
Stroke rehabilitation and patient counselling are competencies IM18.15 and IM18.16 — both at the KH and SH level respectively. The vast majority of stroke survivors have significant residual disability and require structured rehabilitation over months to years. In India, where formal inpatient rehabilitation units are available only in major centres, the general physician is often the primary coordinator of rehabilitation — prescribing and monitoring physiotherapy, occupational therapy, speech therapy, and psychological support from a general medical setting. Counselling is an equally critical skill: family members and patients routinely arrive at outpatient appointments with existential questions about prognosis, dependence, employment, and caregiving that must be addressed accurately, empathetically, and without false reassurance. The final-year student who understands the rehabilitation framework and can communicate prognosis sensitively is ready for internship responsibilities in neurology wards and post-stroke outpatient care.
RECALL
Before studying rehabilitation, recall the neurobiological basis of recovery after stroke. The brain has two mechanisms for recovery: resolution of diaschisis (swelling, oedema, and metabolic depression in connected but undamaged areas resolves over days to weeks, producing rapid early recovery) and neuroplasticity (reorganisation of cortical maps, synaptic sprouting, and recruitment of ipsilateral or contralateral pathways, occurring over months and enabling slower, sustained recovery). Neuroplasticity is use-dependent — it requires repetitive, task-specific practice to drive cortical reorganisation. This is the biological rationale for all stroke rehabilitation: repetition and task specificity. Recall also the major stroke deficits that rehabilitation targets: motor weakness (hemiplegia/hemiparesis), spasticity, aphasia (Broca's, Wernicke's, global), dysphagia, hemianopia, hemispatial neglect, and cognitive impairment. Each deficit requires a different rehabilitation approach and a different timeline of recovery expectations.
Indications for Stroke Rehabilitation
Virtually all stroke survivors with residual neurological deficits are candidates for stroke rehabilitation. The goal of rehabilitation is to maximise functional recovery, prevent complications of immobility and neurological disability, facilitate re-integration into the community, and support the caregiver. It is important to understand that 'indication for rehabilitation' does not require a threshold of disability severity — even mild stroke with subtle functional limitations (difficulty with fine motor tasks, mild word-finding difficulty, balance impairment) benefits from targeted rehabilitation. Conversely, patients with very severe deficits (dense hemiplegia with global aphasia and low GCS) still benefit from early passive rehabilitation to prevent joint contractures, pressure sores, and deep vein thrombosis, even when active motor recovery is not yet a realistic goal.
The specific indications mapped to deficit type are:
- Motor deficit (hemiplegia / hemiparesis): all patients with motor deficit are referred to physiotherapy for graduated mobilisation (sitting → standing → walking), strengthening, balance training, gait re-education, and spasticity management.
- Dysphagia: patients with impaired swallowing are referred to speech and language therapy (SLT) immediately — dysphagia is associated with aspiration pneumonia (the most common early post-stroke complication) and must be managed with safe swallowing strategies or enteral feeding until safe oral intake is possible.
- Aphasia (expressive, receptive, or global): referred to speech and language therapy for language rehabilitation — which requires intensive, repetitive communication practice targeting the specific aphasia type.
- Upper limb impairment and activities of daily living (ADL): referred to occupational therapy (OT) for retraining in ADLs (dressing, bathing, self-feeding, writing), provision of adaptive equipment, and assessment of home environment for modifications.
- Hemianopia / visual neglect: occupational therapy and orthoptic assessment for compensatory scanning strategies, prism glasses, and visual field training.
- Cognitive impairment (memory, attention, executive function): neuropsychological assessment and cognitive rehabilitation programmes — often in specialist stroke or rehabilitation units.
- Psychosocial — depression and adjustment disorder: psychological support, antidepressant therapy (SSRIs — fluoxetine has been studied specifically in post-stroke depression and improves both mood and motor recovery; the FOCUS trial, however, showed no functional benefit of routine fluoxetine prescription), social work assessment for home support and financial entitlements.
- Bladder and bowel dysfunction: pelvic floor physiotherapy, bladder training programme, intermittent catheterisation programme where needed.
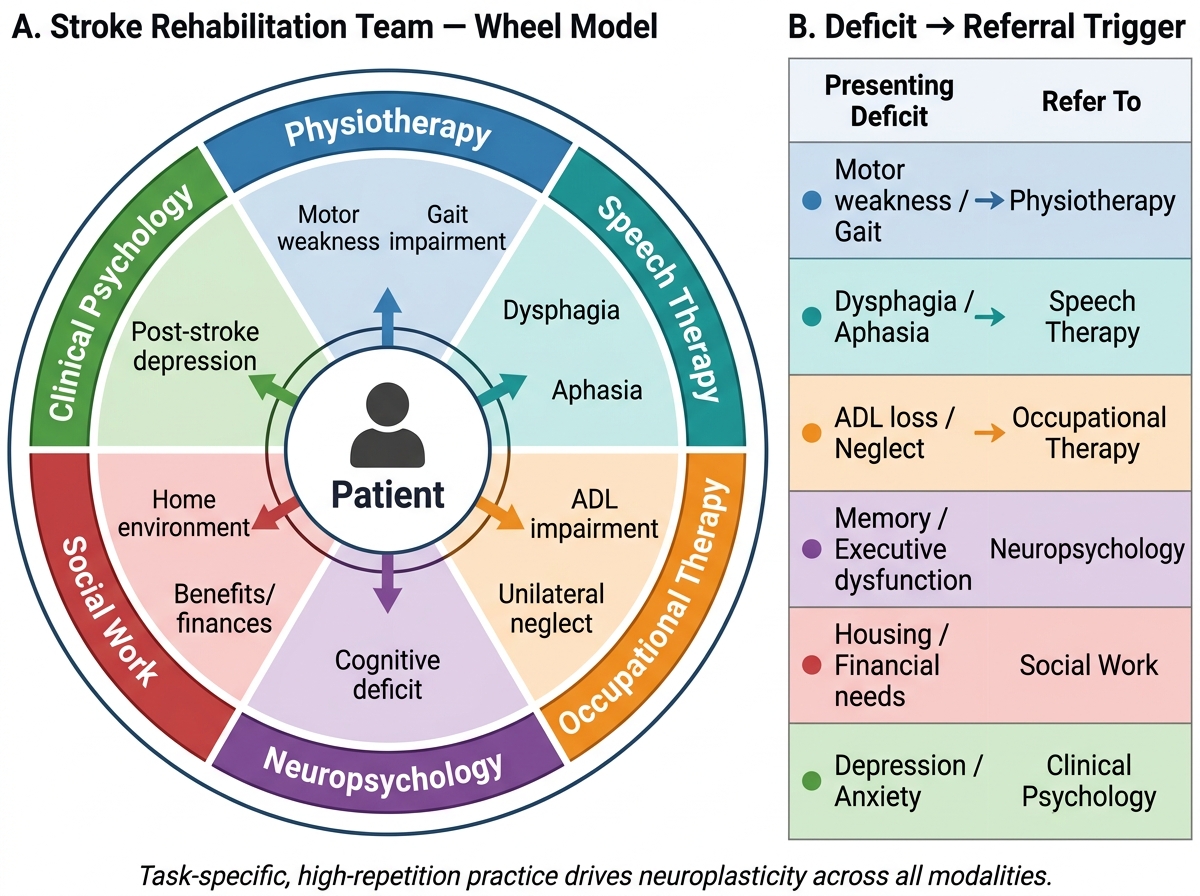
Multidisciplinary Stroke Rehabilitation Team: Deficit-Driven Referral Pathways
Modalities of Stroke Rehabilitation — What Each Discipline Does
Each rehabilitation discipline operates according to specific principles and techniques that are grounded in the neuroscience of motor learning and neuroplasticity. The general physician does not deliver these therapies directly but must understand what each discipline provides in order to write appropriate referrals, set realistic expectations, and interpret progress reports. The key principle unifying all rehabilitation modalities is task-specific, high-repetition practice — the intensity and ecological validity of practice determine the degree of cortical reorganisation achieved. A vague referral to 'physiotherapy' without specifying goals, the relevant deficit, and the target function produces generic, low-intensity sessions that do not drive neuroplasticity. The physician who understands each discipline's toolkit writes referrals that direct therapists to the most effective interventions for each patient's specific impairment profile.
Physiotherapy (PT) — motor rehabilitation:
Physiotherapy for stroke uses a progression of graduated tasks to restore postural control, balance, and functional ambulation. The major approaches include:
- Task-oriented training: practise the actual tasks the patient wants to perform (sit-to-stand, walking to the bathroom) rather than isolated muscle exercises — more effective than non-task-specific strengthening.
- Constraint-induced movement therapy (CIMT): the unaffected arm is constrained (with a mitt or sling) for most waking hours, forcing the affected arm to perform all tasks; proven to drive cortical reorganisation in the motor cortex contralateral to the affected arm; most effective when some wrist/finger extension is preserved (modified CIMT for patients with more severe paresis).
- Robotic assisted therapy: exoskeletal devices (e.g., Armeo, Lokomat) assist repetitive task practice with feedback; used in dedicated rehabilitation centres; growing evidence base for severe upper limb paresis.
- Neuromuscular electrical stimulation (NMES) / functional electrical stimulation (FES): electrical stimulation of paretic muscles to augment voluntary contraction and prevent disuse atrophy — used as adjunct to active PT.
- Gait training: treadmill training with body-weight support for patients who cannot walk independently; progressed to community ambulation training.
- Spasticity management: stretching programmes, splinting to maintain joint position, and coordination with the medical team regarding botulinum toxin injections (Botox) for focal spasticity (e.g., spastic equinovarus foot, flexed wrist/fingers).
Speech and Language Therapy (SLT) — aphasia and dysphagia:
For aphasia, SLT uses repetitive, cueing-based exercises tailored to the aphasia type: naming drills for anomic/Broca's aphasia; comprehension tasks for Wernicke's aphasia; augmentative and alternative communication (AAC) devices (tablets with symbol-based communication apps) for severe global aphasia. Constraint-induced language therapy (CILT) parallels CIMT — the patient must use spoken language even when it is difficult, rather than relying on gestures or writing.
For dysphagia, SLT assesses swallowing using bedside clinical examination and video-fluoroscopic swallowing study (VFSS — the gold standard for characterising pharyngeal aspiration) or FEES (fibre-optic endoscopic evaluation of swallowing). Interventions include: dietary texture modification (IDDSI framework — pureed to normal), postural techniques (chin tuck, head turn towards paretic side), and swallowing manoeuvres (Mendelsohn, supraglottic swallow).
Occupational Therapy (OT) — functional independence:
OT restores independence in activities of daily living through task practice (ADL retraining), adaptive equipment prescription (plate guards, sock aids, one-handed kitchen tools), and home environment assessment (stair rails, bathroom grab bars, ramp for wheelchair access). In India, home visits are often not feasible; OTs provide a practical home-modification checklist based on patient-reported barriers. Driving assessment is performed by OT after sufficient motor and cognitive recovery.
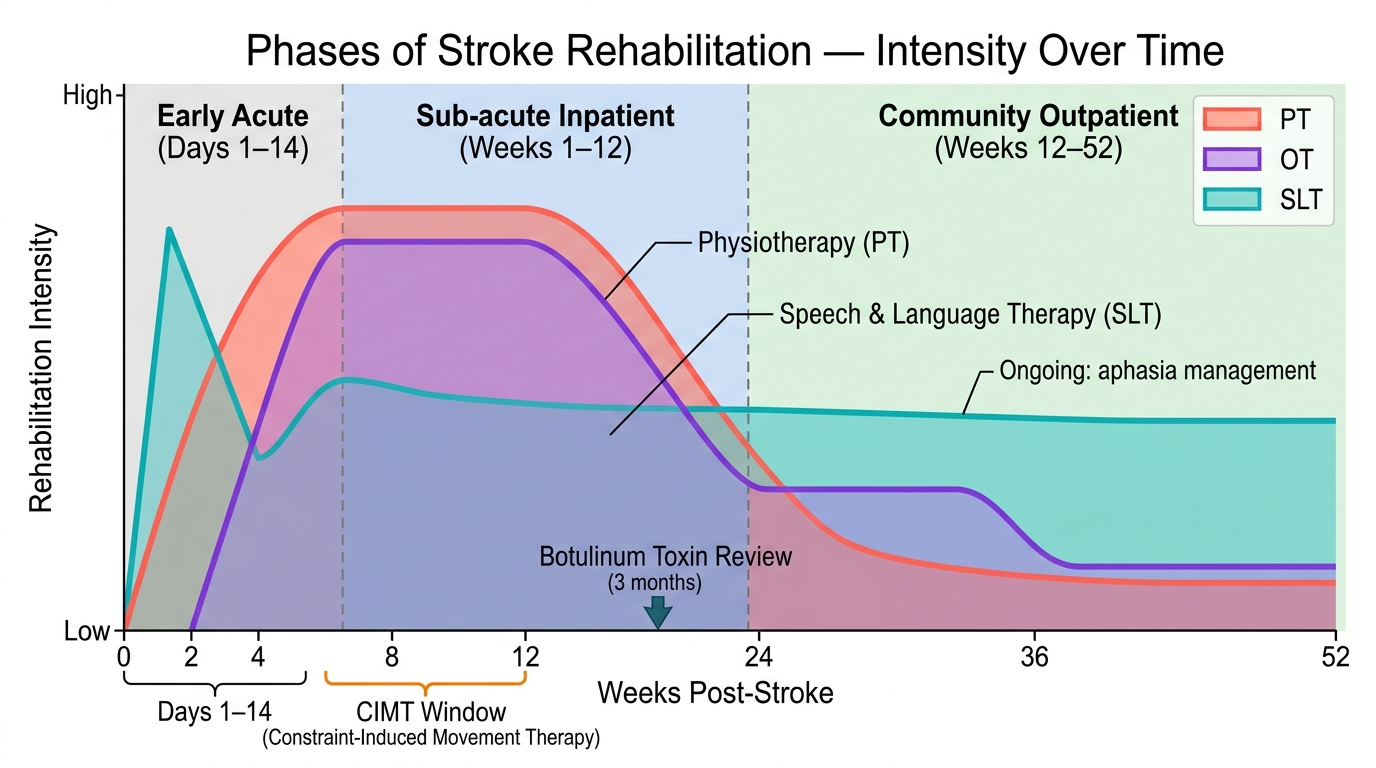
Temporal Intensity of Multidisciplinary Stroke Rehabilitation Across the Three Clinical Phases
Timing and Phases of Stroke Rehabilitation
Stroke rehabilitation is not a single event but a longitudinal process unfolding over three overlapping phases, each with different intensity, goals, and responsible care settings. Understanding the timeline of rehabilitation is clinically essential because it determines when to refer, what to expect at each stage, and when to escalate or step down care. The physician must be able to explain this trajectory to patients and families in a comprehensible way because unrealistic expectations — both over-optimism ('he will be back to normal in 3 months') and under-pessimism ('there is nothing more to do after the first year') — harm the rehabilitation process and damage the therapeutic relationship.
Phase 1 — Acute rehabilitation (Days 1–14, in hospital):
Rehabilitation begins within 24–48 hours of stroke if the patient is medically stable — this is the single most evidence-supported principle in stroke rehabilitation. Early mobilisation (sitting in bed, then chair, then standing) reduces deep vein thrombosis, pressure sore development, aspiration pneumonia, and joint contracture. Dysphagia assessment is a day-1 priority. The target in this phase is safe mobilisation and medical stability, not functional independence. The AVERT trial showed that very early intense mobilisation (within 24 hours, multiple daily sessions) was associated with worse outcomes in some patients — the current recommendation is early but not ultra-early aggressive mobilisation.
Phase 2 — Sub-acute rehabilitation (Weeks 2–12, inpatient rehabilitation unit or home-based with daily therapy):
This is the period of maximum neuroplasticity and the window for the most gains in motor and language function. The intensity of therapy in this phase determines long-term outcome — patients who receive ≥45 minutes of physiotherapy per day in the first 3 months have consistently better outcomes. In India, inpatient rehabilitation units exist in select centres (NIMHANS, AIIMS, PGI, KEM); most patients receive outpatient or home-based therapy. Goals: independent or supervised ambulation, upper limb function for ADLs, safe oral intake (or planned enteral feeding), family training in handling and positioning, psychological support.
Phase 3 — Community rehabilitation (3 months to 1 year and beyond):
After the initial intensive phase, outpatient or community therapy continues with reducing frequency but sustained goal-orientation. Evidence shows that motor and language recovery continues beyond 6 months and even beyond 1 year with continuing practice — the traditional teaching of 'no recovery after 6 months' is outdated. Goals in this phase include: return to preferred activities, vocational rehabilitation for working-age patients, carer support and respite services, driving assessment, and long-term secondary prevention. The modified Rankin Scale (mRS) is the standard outcome measure at 3 and 12 months: mRS 0 = no symptoms; mRS 2 = slight disability but independent; mRS 3 = moderate disability requiring some assistance; mRS 5 = severe disability, total dependence.
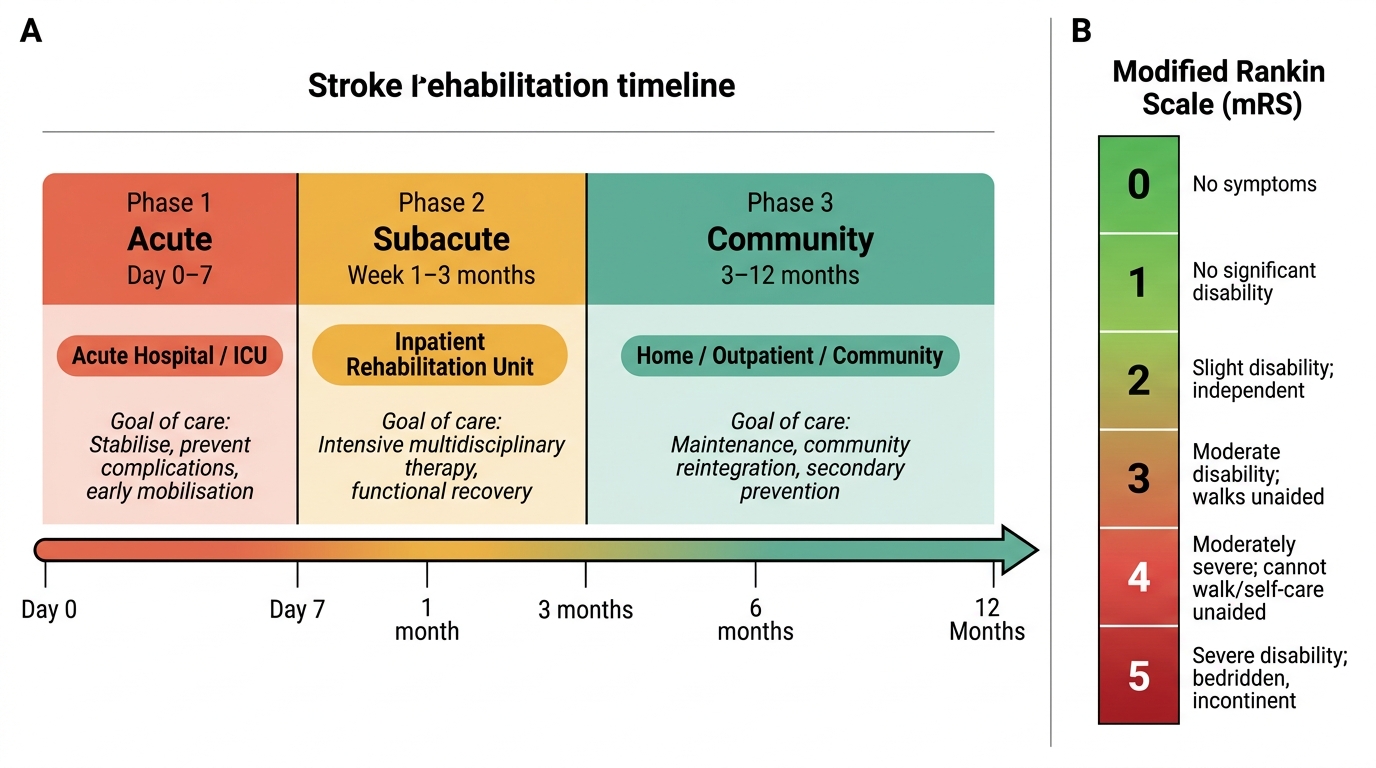
Stroke Rehabilitation Phases and Modified Rankin Scale (mRS)