Page 14 of 21
IM18.15-16 | Stroke Rehabilitation and Counselling — SDL Guide (Part 2)
Communicating Prognosis — What to Tell the Patient and Family
Prognostic communication is one of the most complex clinical communication tasks in neurology and internal medicine. Stroke prognosis is variable, depends on multiple factors, and cannot be predicted with certainty for any individual — yet patients and families deserve an honest, specific, and humane account of what to expect. The physician who gives vague non-answers ('we'll see how things go') fails the patient; the one who gives falsely precise predictions damages trust when reality diverges. The skill lies in communicating genuine uncertainty while providing a meaningful framework for planning and hope.
Factors determining stroke recovery:
Prognosis is shaped by: the location and volume of the infarct (NIHSS and DWI lesion volume are the strongest early predictors); the patient's age and premorbid functional status; the presence and quality of rehabilitation; comorbidities (diabetes and pre-existing cognitive impairment worsen recovery); and the time to treatment (thrombolysis/thrombectomy improves the recovery trajectory). The NIHSS at 24–72 hours is a strong predictor: NIHSS <6 = 70–80% independence at 3 months; NIHSS 6–15 = 50% independence; NIHSS >15 = less than 30% independence with medical management alone.
Recovery timelines by deficit type (for counselling purposes):
- Motor function: maximum recovery occurs in the first 3–6 months; meaningful recovery continues to 12 months. A patient with full arm paralysis at 48 hours who has any wrist extension by week 2 has a significantly better motor prognosis. Patients who have no voluntary movement at 4 weeks are unlikely to regain functional use of the hand (but may still regain walking).
- Aphasia: language recovery is slower and more prolonged than motor recovery. Comprehension (Wernicke's) tends to recover better than expression (Broca's). Intensive, ongoing speech therapy drives recovery even beyond 1–2 years. Mild anomia and word-finding difficulty may persist indefinitely but do not prevent meaningful communication.
- Dysphagia: 65–70% of acute stroke patients have dysphagia; the majority (>60%) resolve within the first 2–4 weeks. Persistent dysphagia at 3 months indicates the need for long-term enteral feeding or dietary modification.
- Depression: post-stroke depression affects 30–35% of stroke survivors and is a major predictor of poor rehabilitation outcome. It should be actively screened for (PHQ-9 or the validated CSSD) at every post-stroke visit, not assumed to be inevitable or untreatable.
The communication framework — SPIKES for bad news in stroke:
The SPIKES protocol (Setting, Perception, Invitation, Knowledge, Empathy, Summary) provides structure:
- Setting: private space, family present if the patient wishes, adequate time (not a corridor conversation).
- Perception: 'Can you tell me what you understand about what has happened?' — establishes baseline and avoids information mismatch.
- Invitation: 'Would you like me to explain in detail what we expect for recovery?'
- Knowledge: deliver information in plain language, in steps, without jargon — 'The stroke caused damage to the part of the brain that controls your right arm and your speech. The damage cannot be reversed, but the brain can learn new ways to do things, especially with intensive therapy over the next few months.'
- Empathy: name and acknowledge the emotion — 'I can see this is very hard to hear. It is completely understandable to feel frightened and overwhelmed.'
- Summary: summarise the plan — what therapy will happen, who to call with questions, what the next review appointment is for.
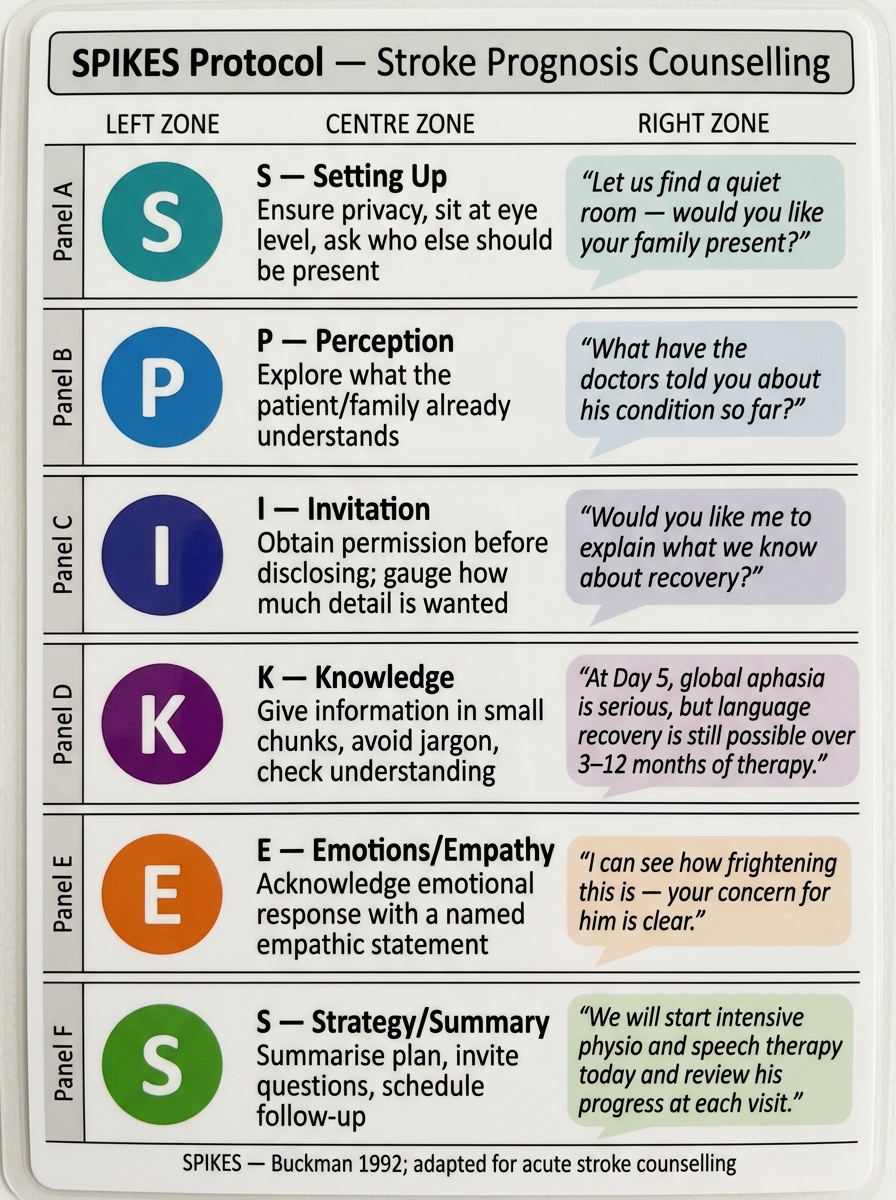
SPIKES Protocol — Pocket Reference Card for Stroke Prognosis Counselling
SELF-CHECK
A 60-year-old man with right MCA stroke has dense left hemiplegia and global aphasia. It is now Day 5. His wife asks: 'Will my husband ever speak and walk again?' Which response BEST reflects evidence-based, empathetic communication?
A. 'We cannot say anything about recovery until at least 6 months — it is too early to predict.'
B. 'The damage is permanent. He will not speak or walk again. You should plan for long-term care.'
C. 'Recovery from aphasia and hemiplegia is possible with intensive therapy over the next 3–12 months. Global aphasia at day 5 is a serious sign, but meaningful language can still return, especially comprehension. Starting intensive physiotherapy and speech therapy immediately gives the best chance. We will review progress at each visit.'
D. 'He will make a full recovery — strokes at his age usually recover well.'
Reveal Answer
Answer: C. 'Recovery from aphasia and hemiplegia is possible with intensive therapy over the next 3–12 months. Global aphasia at day 5 is a serious sign, but meaningful language can still return, especially comprehension. Starting intensive physiotherapy and speech therapy immediately gives the best chance. We will review progress at each visit.'
Option C is the correct answer because it is honest (acknowledges global aphasia is a serious sign), evidence-based (recovery continues over months with therapy), hopeful without false reassurance (does not promise full recovery), and action-oriented (frames the next steps — therapy, review visits). Option A is unhelpfully vague and delays realistic planning. Option B is falsely pessimistic — global aphasia at day 5 does not preclude meaningful language recovery, and motor recovery with physiotherapy is expected in most patients. Option D is falsely reassuring and inaccurate. The key principle: communicate genuine uncertainty with a recovery framework, not vague non-answers or false precision.
Counselling the Patient — Specific Post-Stroke Issues
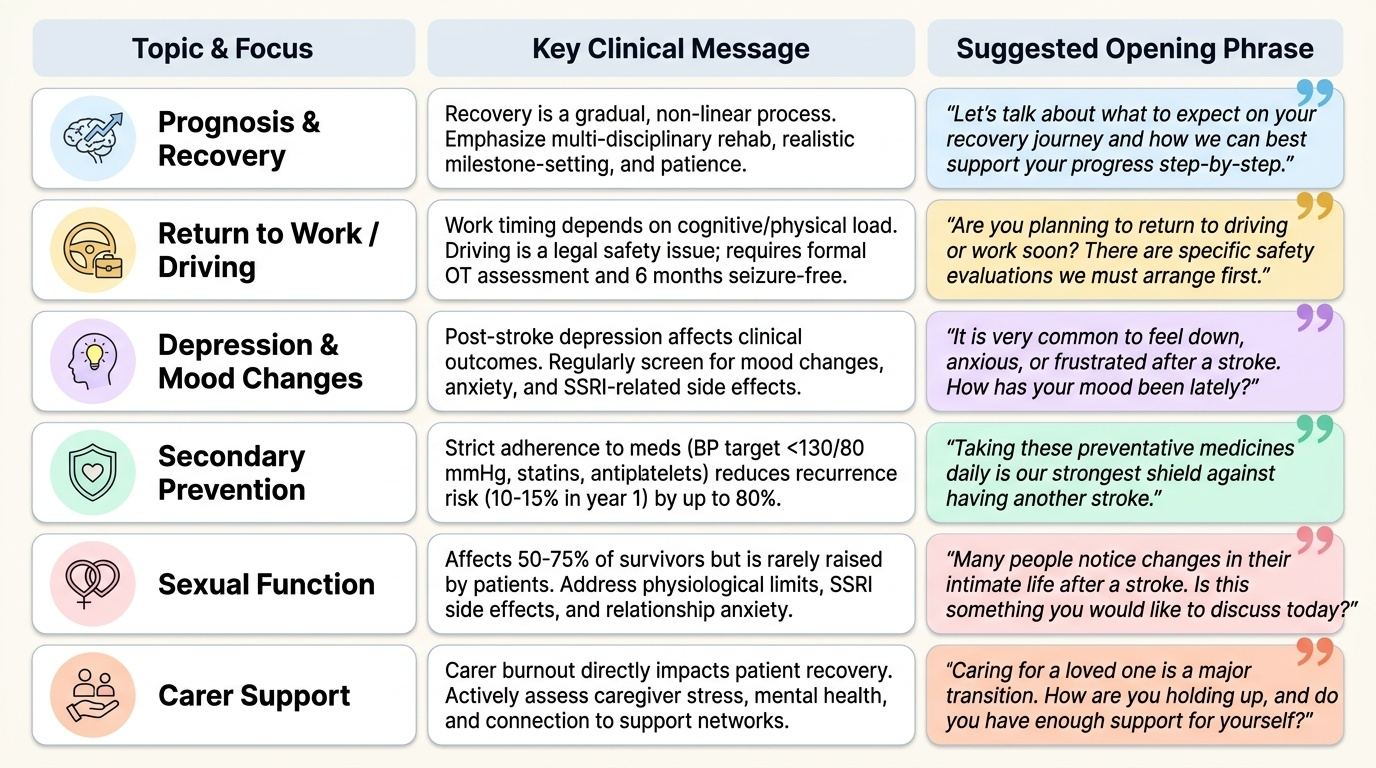
Beyond prognostic communication, several specific counselling conversations arise recurrently in post-stroke outpatient care and must be managed with accurate, practical, and empathetic information. The final-year student and intern will encounter all of these in the first year of clinical practice and must be prepared to address them directly without deflecting to a specialist.
Provided image
Return to work and driving:
Return-to-work timing depends on the nature of the work, the degree of residual deficit, and any cognitive impairment. Most patients with mild stroke and a desk-based job can return to work within 3–6 months; physical and cognitive work requires fuller assessment. Driving is a legal and safety issue — in most Indian states, patients who have had a stroke should not drive until medically cleared; this requires a formal driving assessment (usually by an OT, after a minimum 6-month seizure-free period if post-stroke seizure occurred). The physician must explicitly address driving with every post-stroke patient, not leave it to the patient to raise.
Sexual function and intimacy:
Post-stroke sexual dysfunction is common and is almost never discussed unless the physician initiates the conversation. Reduced libido, erectile dysfunction (in males), and impaired sensation affect 50–75% of stroke survivors. Antidepressants (SSRIs) prescribed for post-stroke depression can compound this. The conversation should be normalised: 'Many people after a stroke notice changes in their intimate life — is this something you would like to discuss or get advice about?'
Secondary prevention and risk factor management:
Counselling at every post-stroke visit must include reinforcement of secondary prevention: antiplatelet therapy compliance, anticoagulation for AF (CHA₂DS₂-VASc ≥2), statin therapy, blood pressure control (target <130/80 mmHg in most ischaemic stroke survivors), diabetes management, smoking cessation, and alcohol reduction. The risk of recurrent stroke is 10–15% in the first year and 5–8% per year thereafter — this risk is substantially reduced by secondary prevention measures. Communicating this risk concretely ('your risk of having another stroke in the next year is about 10–15% if you take all the medications and make lifestyle changes; it is higher if you stop') motivates adherence.
Carer support:
The caregiver — typically a spouse or adult child — bears an enormous burden after stroke. Carer burnout, depression, and physical strain are common and are independent predictors of poor stroke survivor outcomes. Every post-stroke consultation should include a brief assessment of carer wellbeing: 'How are you coping? Are you getting enough sleep? Is there anything you need help with?' Signposting to support groups (Indian Stroke Association caregiver resources), respite care, and home nursing services is part of the physician's role.
Post-stroke epilepsy:
Approximately 5–10% of stroke survivors develop epilepsy (early seizures within 7 days of stroke in 5%; late post-stroke epilepsy beyond 7 days in 3–5%). Patients should be counselled that seizures are a known complication, and to seek emergency care for any new seizure. Routine prophylactic antiepileptic drugs are NOT recommended after stroke in the absence of seizures — this should be explicitly communicated to avoid inappropriate prescription by non-specialists.
SELF-CHECK
A 55-year-old woman had a right parietal ischaemic stroke 4 months ago. Her residual deficits are mild — slight left hand weakness and left hemispatial neglect. She asks whether she can resume driving. What is the MOST APPROPRIATE advice?
A. She can resume driving immediately — her deficits are mild.
B. She should never drive again after a stroke.
C. She should not drive until she has had a formal driving assessment, typically after at least 3 months of stability and with confirmation that the neglect has resolved or is adequately compensated.
D. She can drive on local roads but not highways, as the risk is lower.
Reveal Answer
Answer: C. She should not drive until she has had a formal driving assessment, typically after at least 3 months of stability and with confirmation that the neglect has resolved or is adequately compensated.
Hemispatial neglect is a significant driving safety hazard — the patient does not attend to the left visual field, which directly impairs the ability to detect pedestrians, vehicles, and hazards. Even mild neglect is a contraindication to driving until formally assessed. The minimum period for reassessment is generally 3–6 months of stable neurological status; a formal driving assessment by an occupational therapist or designated driving assessment centre is required. Option A is unsafe — 'mild deficits' does not mean no driving risk; neglect is particularly hazardous. Option B is too absolute — many stroke survivors return to driving successfully after assessment. Option D has no evidence base and is clinically unsafe. The physician must raise driving explicitly at every post-stroke visit.
Applied Practice — Coordinating the Multidisciplinary Team from a General Medicine Setting
In Indian general hospitals, stroke rehabilitation is rarely delivered by a dedicated stroke unit team. The general physician, house surgeon, or medical officer is often the de facto coordinator of post-stroke care — writing referrals, monitoring rehabilitation progress, managing comorbidities, prescribing secondary prevention, and providing the face of continuity for the patient and family. Applied practice in this context means understanding what to do when the ideal system is unavailable, how to triage referral urgency, and how to document rehabilitation goals in the patient record in a way that enables any treating doctor to continue the care plan.
Writing an effective rehabilitation referral:
A good rehabilitation referral includes: the stroke date and type (ischaemic/haemorrhagic); the location and NIHSS at onset and current; the specific deficit being referred for (dysphagia, aphasia, right hemiplegia); the functional goal (safe oral intake, ambulation to bathroom, return to writing); and any specific precautions (seizure risk, cardiac precautions, fall risk). A vague referral ('for physiotherapy') without functional goals leads to low-intensity, non-targeted therapy.
Prescribing for spasticity:
When physiotherapy alone does not control spasticity limiting function or causing pain, the general physician may initiate oral agents: baclofen (GABA-B agonist; start 5 mg TDS, titrate to 20–80 mg/day) for generalised spasticity; tizanidine (alpha-2 agonist; start 2 mg nocte, maximum 36 mg/day) as an alternative. Botulinum toxin type A injections (prescribed by a neurologist or rehabilitation physician) are the gold standard for focal, function-limiting spasticity (e.g., equinovarus foot preventing gait training, flexed elbow/wrist preventing ADLs).
Post-stroke depression — when to prescribe:
Post-stroke depression should be treated with an SSRI when it is causing significant distress or interfering with rehabilitation participation. Escitalopram (10–20 mg/day) is well tolerated and widely used. Avoid tricyclic antidepressants (cardiac risk, high anticholinergic load). Counsel the patient that antidepressants take 2–4 weeks to show effect and should not be stopped abruptly. Psychological therapy (CBT-based) is effective and should be offered alongside pharmacotherapy where available.
The post-stroke review consultation structure:
Every post-stroke outpatient visit should systematically cover: (1) neurological examination — any change in NIHSS or mRS?; (2) rehabilitation progress — OT/PT/SLT reports, functional goals achieved?; (3) secondary prevention — compliance with antiplatelet/anticoagulant/statin/antihypertensive, BP measured today, HbA1c if diabetic, latest INR if on warfarin; (4) comorbidities and complications — depression screen (PHQ-2 minimum), seizure history, UTI/chest infection, pressure sores?; (5) psychosocial — carer wellbeing, home equipment, social support; (6) next steps — when is the next imaging review? When is the driving assessment?
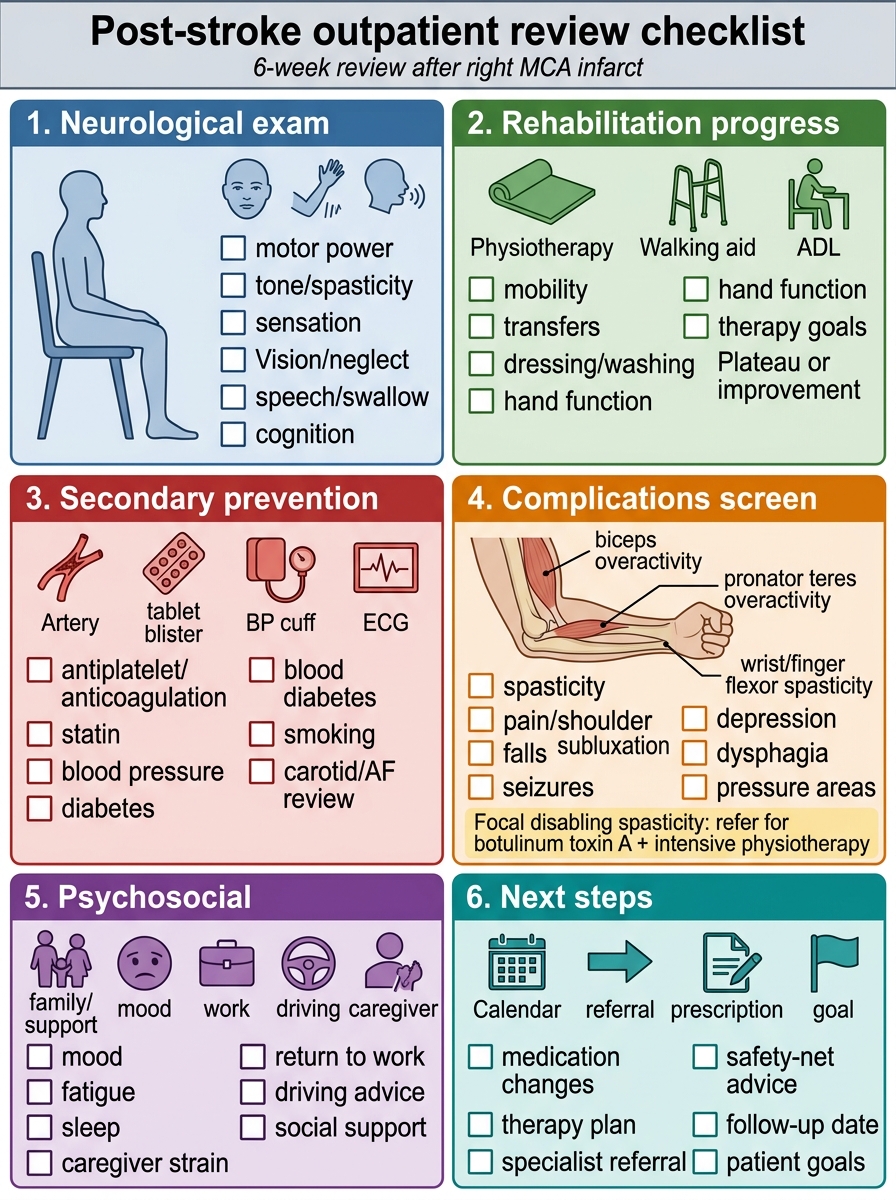
Post-Stroke Outpatient Review Checklist
SELF-CHECK
A 62-year-old man with a 6-week-old right MCA infarct has right arm spasticity limiting his ability to dress and wash. His physiotherapy has plateaued. He is on baclofen 20 mg TDS with incomplete effect. The next MOST APPROPRIATE management of his focal arm spasticity is:
A. Increase baclofen to maximum dose (80 mg/day) and continue physiotherapy
B. Add tizanidine 4 mg BD to his baclofen
C. Refer to a neurologist or rehabilitation physician for botulinum toxin type A injections to the affected upper limb muscles, combined with intensive physiotherapy
D. Discharge from physiotherapy — no further gains are expected after 6 weeks
Reveal Answer
Answer: C. Refer to a neurologist or rehabilitation physician for botulinum toxin type A injections to the affected upper limb muscles, combined with intensive physiotherapy
Focal arm spasticity limiting specific functions (dressing, washing) is the primary indication for botulinum toxin type A injections, which temporarily paralyse the overactive muscle groups (typically biceps, pronator teres, wrist/finger flexors) for 3–4 months, creating a therapeutic window for intensive physiotherapy to train new movement patterns. Escalating baclofen further risks dose-related sedation, weakness, and cognitive side effects without targeting the focal muscles causing the specific functional limitation. Combining two oral antispastic agents (baclofen + tizanidine) increases systemic side effect burden without the precision of focal injection. Discharging from physiotherapy at 6 weeks is premature — meaningful gains can continue to 12 months and beyond. The correct pathway is focal Botox by a specialist + continuation of task-specific physiotherapy.