Page 15 of 21
IM18.15-16 | Stroke Rehabilitation and Counselling — SDL Guide (Part 3)
Self-Assessment: Integrating Rehabilitation and Counselling
The rehabilitation and counselling competencies are assessed not through knowledge recall alone, but through the application of knowledge to simulated patient interactions and clinical scenarios that reflect real post-stroke consultations. The scenarios below require you to integrate the rehabilitation framework, prognostic information, and communication skills from this module.
Scenario A: Mrs Meenakshi Iyer, 68 years old, was admitted for a lacunar infarct affecting the posterior limb of the internal capsule 10 days ago. She has pure motor hemiplegia — moderate right arm and leg weakness, NIHSS = 6 now (was 10 on admission). She is walking with a frame. Her daughter wants to know: (i) whether she can return home next week; (ii) whether she needs a professional carer; (iii) when she can drive. How do you counsel the family?
Analysis: Lacunar infarct with improving motor deficit (NIHSS 10 → 6) — good recovery trajectory. Mobilising with a frame at 10 days = appropriate. Discharge home next week is reasonable if the home environment is safe (OT home assessment or checklist), family can provide supervision, physiotherapy can be arranged as outpatient or home-based, and there is no dysphagia. Professional carer: not necessarily — if family can supervise and assist with ADLs, a home physiotherapy programme may suffice; reassess at 6 weeks. Driving: advise clearly — she should not drive until neurologically stable at minimum 3–6 months, and a formal driving assessment is required before resuming.
Scenario B: Mr Arun Mehta, 50 years old, had a large left MCA ischaemic stroke 3 months ago. He has Broca's aphasia (telegraphic speech, preserved comprehension) and right hemiplegia with partial hand recovery. He is very frustrated and tearful during the consultation. His wife says he has been refusing physiotherapy because 'he says it's pointless'. PHQ-9 score = 16 (moderate depression). How do you manage this?
Analysis: Post-stroke depression is impairing rehabilitation participation — this is a recognised pattern. Acknowledge the frustration directly and empathetically ('I can understand why this feels overwhelming — your life has changed profoundly'). Explain that depression after stroke is a brain-based condition, not weakness, and is treatable. Prescribe escitalopram 10 mg daily (or equivalent SSRI); review at 4 weeks. Arrange psychological support if available. Discuss the frustration with the physiotherapy team — a brief break followed by re-engagement with modified short-term goals may help. Counsel the family: their role is supportive, not coercive — forced therapy participation is counterproductive. Set a specific review appointment (4 weeks) to assess mood and therapy re-engagement.
Scenario C: You are reviewing Mr Venkat Rao, 74 years old, at 6 months post-haemorrhagic stroke (right thalamic ICH). His mRS = 3 (moderate disability; requires assistance for some activities but independent for basic ADLs with aids). His daughter asks: 'Should we restart his aspirin? His cardiologist said he needs it for his coronary artery disease. But we are scared about another bleed.' How do you advise?
Analysis: This is a real and common clinical tension. The evidence (RESTART trial, 2019) shows that restarting antiplatelet therapy after ICH in patients with a separate compelling indication (CAD, previous ischaemic stroke) reduces the risk of recurrent vascular events without significantly increasing the risk of recurrent ICH — the risk of recurrent vascular events outweighs the risk of recurrent ICH in most patients. At 6 months post-ICH, the haematoma has resolved. The decision should be made jointly with neurology and cardiology input. The family's concern is valid and should be acknowledged. Explain the RESTART evidence in plain language: 'The research suggests that the risk of a second bleed from aspirin is small compared to the risk of a heart attack or ischaemic stroke if aspirin is withheld. We are recommending aspirin with close monitoring.'
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
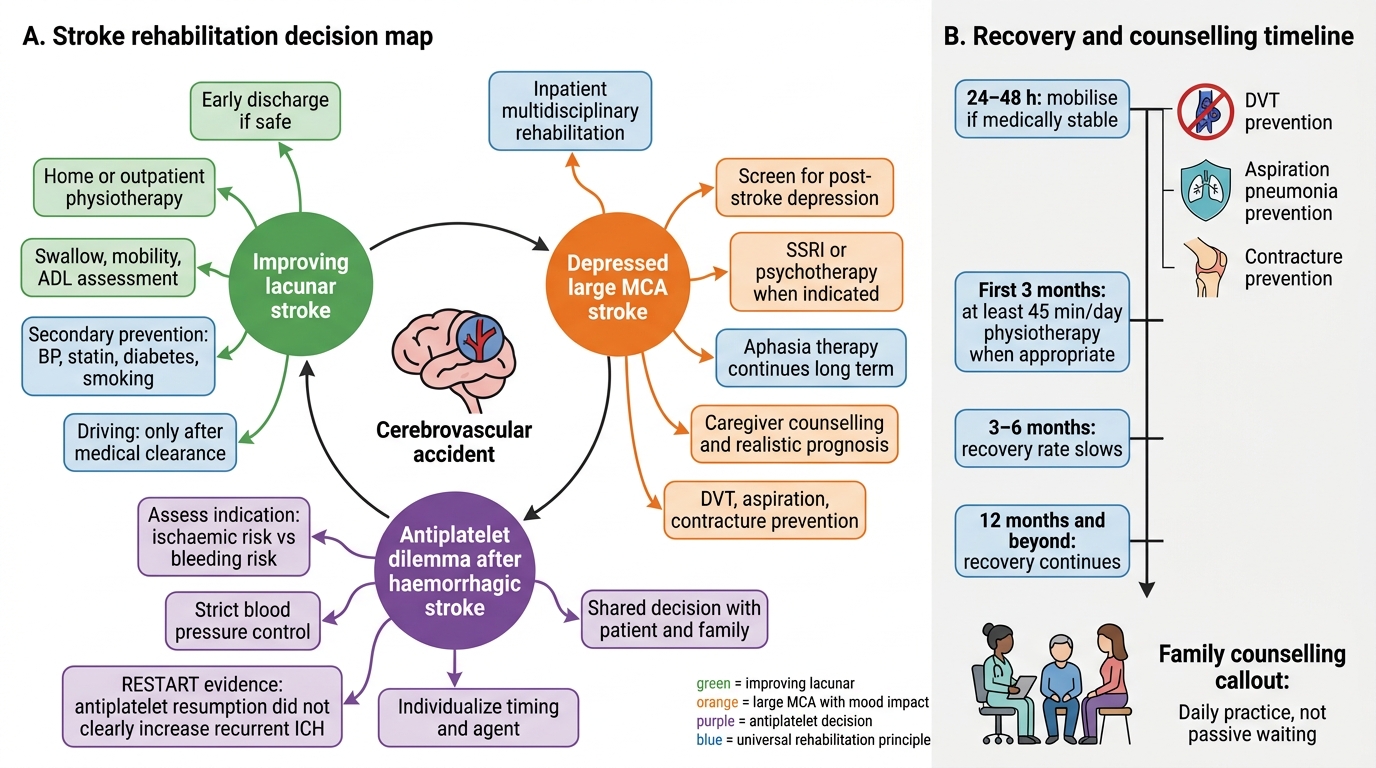
Stroke Rehabilitation and Counselling Decision Map
CLINICAL PEARL
The single most evidence-supported principle in stroke rehabilitation is early mobilisation — beginning within 24–48 hours of stroke if medically stable. Early sitting and standing prevent deep vein thrombosis, aspiration pneumonia, and joint contractures, and may improve long-term functional outcome. The earlier and more intensive the rehabilitation (minimum 45 minutes per day of physiotherapy in the first 3 months), the better the functional outcome.
For counselling, the most common error is either excessive pessimism ('there is nothing more to do after 3 months') or excessive optimism ('he will be back to normal'). The truth is evidence-based and honest: recovery continues with therapy for 12 months and beyond; the rate slows after 3–6 months but does not stop. Language recovery from aphasia is particularly prolonged and should never be abandoned. Teach families to frame rehabilitation as a daily practice, not a passive waiting exercise.