Page 5 of 14
IM19.3-6 | Movement Disorder Clinical Evaluation — SDL Guide (Part 2)
Interpretation of Findings: Rating Scales and Clinical Synthesis
Clinical findings from the history and examination must be integrated and interpreted systematically to generate a differential diagnosis and an anatomical formulation. This requires familiarity with validated rating scales and a framework for synthesising the individual findings into a coherent clinical picture.
Provided image
The value of systematic rating is not merely academic. A baseline MDS-UPDRS Part 3 score before treatment initiation, combined with a score 3 months after levodopa is started, objectively demonstrates the magnitude of the therapeutic response. This levodopa challenge response has diagnostic weight: a reduction in MDS-UPDRS Part 3 score of 30% or more is considered a clinically significant and supportive response for idiopathic PD. Conversely, a minimal response to adequate levodopa doses raises suspicion of Parkinson-plus syndrome or drug-induced parkinsonism, shifting the differential. Beyond PD, different movement disorders require different validated instruments — a single scale cannot serve all conditions, and choosing the correct instrument for the clinical question at hand is itself a competency tested in the IM19 curriculum.
The MDS-UPDRS (Movement Disorder Society Unified Parkinson's Disease Rating Scale) is the standard instrument for assessing all aspects of PD comprehensively. It has four parts:
- Part I: Non-motor experiences of daily living (cognitive impairment, hallucinations, depression, anxiety, apathy, autonomic symptoms — 13 items)
- Part II: Motor experiences of daily living (patient-reported impact on ADLs — speech, swallowing, handwriting, hobbies, gait, freezing — 13 items)
- Part III: Motor examination (clinician-rated — 18 items covering speech, facial expression, rigidity at 5 sites, finger tapping, hand movements, pronation-supination, toe tapping, leg agility, arising from chair, gait, freezing, postural stability, posture, body bradykinesia, postural tremor of hands, kinetic tremor of hands, rest tremor of limbs, constancy of rest tremor)
- Part IV: Motor complications (dyskinesias — duration and disability; OFF state — duration and predictability; painful OFF dystonia)
Each item is scored 0 (normal) to 4 (severe). A total Part III score is used to gauge overall motor severity; the individual item scores allow tracking of specific features over time and document the response to therapy.
Other rating scales relevant to movement disorders:
- Hoehn and Yahr Scale (modified): a staging scale for PD severity from 1 (unilateral disease only) to 5 (wheelchair-bound or bedridden). Simple and widely used but less sensitive to change than the MDS-UPDRS.
- Abnormal Involuntary Movements Scale (AIMS): a 12-item scale for rating orofacial, trunk, and limb dyskinesias (particularly tardive dyskinesia); used to monitor and document the severity and extent of drug-induced or treatment-induced dyskinesias.
- Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS): assesses severity and disability from dystonia across body regions; used for generalised dystonias.
- Unified Huntington's Disease Rating Scale (UHDRS): comprehensive scale covering motor, cognitive, behavioural, and functional domains in Huntington's disease.
Generating the differential diagnosis:
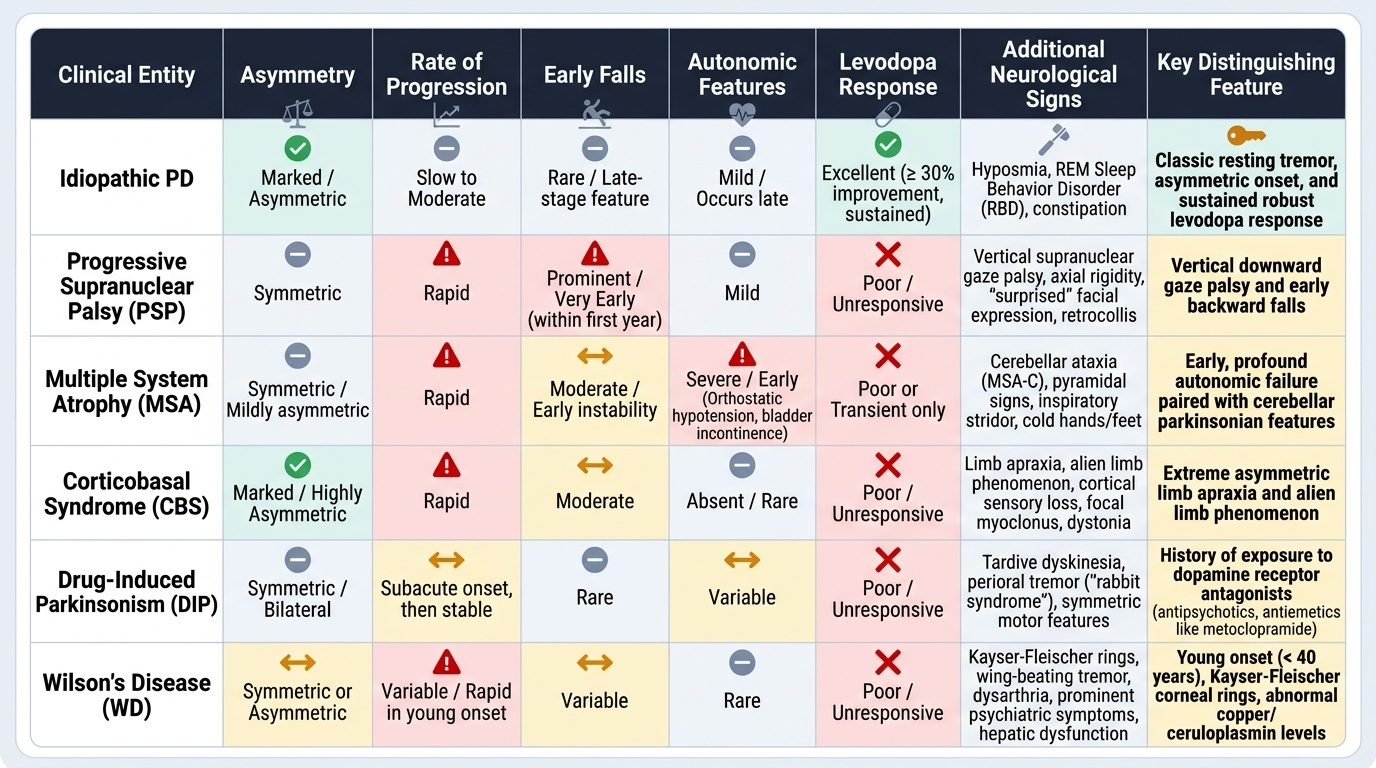
After completing the history and examination, generate the differential diagnosis by considering the findings in their totality. The differential should be ranked (most likely to least likely) and driven by the clinical pattern, not by a memorised list. The key clinical discriminators are:
1. Phenomenological category: rest tremor with TRAP features → parkinsonian syndrome; postural tremor + no bradykinesia/rigidity → essential tremor; irregular random movements → chorea; twisting postures → dystonia.
2. Asymmetry at onset: idiopathic PD is typically asymmetric at onset; drug-induced parkinsonism is often symmetric; Parkinson-plus syndromes are variably symmetric.
3. Age of onset: young (<40) with dystonia/chorea → Wilson's, DYT1, juvenile Huntington's; older adult with parkinsonism → PD vs Parkinson-plus.
4. Rate of progression: slowly progressive over years → PD; rapidly progressive → Parkinson-plus (especially MSA, PSP), drug-induced, or Wilson's.
5. Additional neurological features (red flags for Parkinson-plus):
- Early falls (within 3 years of onset) → PSP, MSA-P
- Vertical gaze palsy → PSP (cannot look down voluntarily)
- Early and prominent autonomic failure (orthostatic hypotension, urinary incontinence, erectile dysfunction) → MSA
- Cerebellar ataxia with parkinsonism → MSA-C
- Asymmetric limb rigidity + apraxia + alien limb phenomenon → corticobasal syndrome
- Cognitive fluctuations + visual hallucinations + parkinsonism → DLB
- Poor or no levodopa response → Parkinson-plus, drug-induced, Wilson's
SELF-CHECK
A 65-year-old man has a 3-year history of parkinsonism (rigidity, bradykinesia, tremor) that is symmetric from onset. He has been on metoclopramide 30 mg/day for gastroparesis for the past 4 years. Which feature MOST supports a diagnosis of drug-induced parkinsonism rather than idiopathic Parkinson's disease?
A. The presence of cogwheel rigidity at both wrists
B. Symmetric onset and known exposure to a dopamine receptor-blocking agent
C. Bradykinesia confirmed on finger-tapping test
D. Reduced arm swing on gait examination
Reveal Answer
Answer: B. Symmetric onset and known exposure to a dopamine receptor-blocking agent
Drug-induced parkinsonism (DIP) typically presents with symmetric motor features (bilateral from onset) in contrast to idiopathic PD which is characteristically asymmetric at onset. The critical additional feature here is long-term exposure to metoclopramide — a dopamine D2 receptor antagonist that crosses the blood-brain barrier (unlike domperidone) and can block the nigrostriatal dopaminergic pathway, causing TRAP features indistinguishable from PD on examination. Cogwheel rigidity, bradykinesia on finger tapping, and reduced arm swing all occur in both DIP and idiopathic PD — they confirm the parkinsonian syndrome but do not discriminate the cause. The combination of symmetry + DRBA exposure is the red flag.
Applied Practice: Anatomical Localisation and Diagnostic Formulation
The final step of the clinical evaluation is the diagnostic formulation — a concise, structured synthesis of the history and examination findings that specifies the anatomical location of the lesion or dysfunction, the nature of the pathological process, and the probable cause. This formulation is the output of the entire evaluation process and directly determines the investigations ordered and the treatment initiated. Writing a precise diagnostic formulation is itself a clinical skill that must be practised.
Provided image
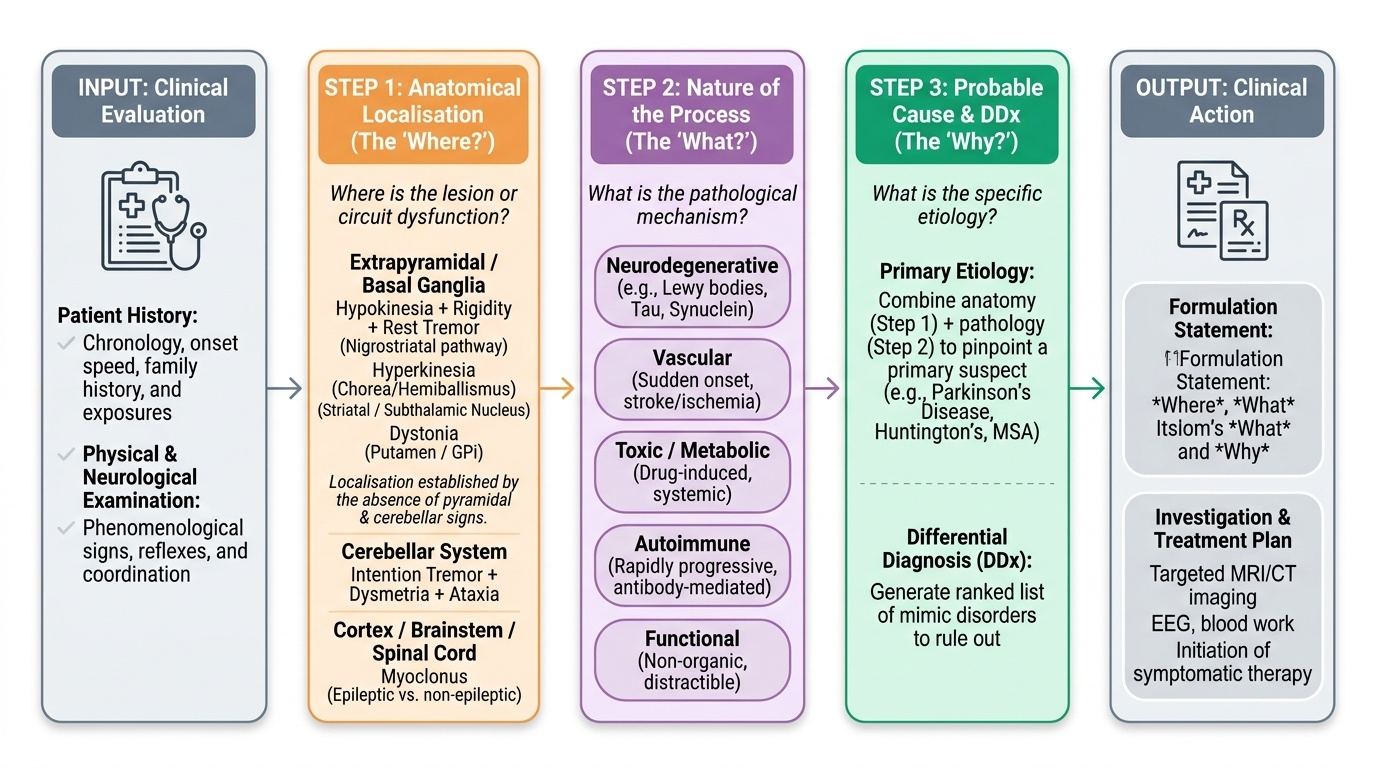
The three-part anatomical formulation for any neurological condition — including movement disorders — answers: (1) Where is the lesion? (2) What is the nature of the process? (3) What is the probable cause?
Step 1 — Anatomical localisation:
For movement disorders, localisation uses the phenomenological category as the key:
- Hypokinesia + rest tremor + rigidity → basal ganglia (primarily the nigrostriatal pathway, i.e., substantia nigra → striatum circuit)
- Hyperkinesia (chorea, hemiballismus) → basal ganglia (striatal or subthalamic nucleus involvement); chorea may also implicate the caudate nucleus preferentially (striatal atrophy in Huntington's)
- Intention tremor + dysmetria + ataxia → cerebellum or cerebellar connections
- Dystonia → basal ganglia (putamen, GPi) in secondary cases; primary dystonia may have a circuit abnormality without a visible structural lesion
- Myoclonus → can localise to cortex (cortical myoclonus = epileptic), brainstem, spinal cord, or peripheral nerve depending on EEG correlate and clinical context
For most movement disorders in the neurology outpatient setting, the anatomical localisation to the basal ganglia (extrapyramidal system) is established by excluding pyramidal signs (no weakness, no hyperreflexia, no upgoing plantar) and cerebellar signs (no intention tremor, no dysmetria, no nystagmus). The absence of these signs, combined with the presence of extrapyramidal features (TRAP, chorea, dystonia), localises the problem to the extrapyramidal system.
Step 2 — Nature of the process:
Common pathological processes in movement disorders:
- Neurodegenerative: progressive, no reversible cause, pathological hallmarks at autopsy (Lewy bodies in PD/DLB, tau inclusions in PSP/CBS, alpha-synuclein in MSA)
- Vascular: sudden onset (a vascular event in the basal ganglia); hemiballismus from STN infarct is the classic example
- Toxic/drug-induced: exposure to a causative agent; potentially reversible
- Metabolic: Wilson's disease, hepatic encephalopathy, hypo/hyperglycaemia, thyrotoxicosis
- Autoimmune/inflammatory: Sydenham's chorea (post-streptococcal), SLE-associated chorea (anti-phospholipid antibodies), paraneoplastic
- Genetic: inherited pattern, family history, gene testing
- Functional (psychogenic): inconsistency of phenomenology, entrainability to examiner's rhythm, distractibility of tremor, positive Hoover's sign
Step 3 — Probable cause:
Combine the localisation, the nature of the process, and the clinical demographic (age, sex, duration, associated features) to produce the most likely aetiology. Document this as: 'This is most likely [diagnosis], based on [clinical features], with [supporting evidence]. Alternatives include [ranked differential]. The diagnosis can be confirmed/excluded by [specific investigations].'
Example formulation (Parkinson's disease):
'This 63-year-old man presents with a 3-year history of asymmetric, insidiously progressive, hypokinetic-rigid syndrome with rest tremor. Anatomically, the findings (TRAP, right-sided > left-sided, positive pull test, shuffling gait with reduced right arm swing) localise to the basal ganglia — specifically the nigrostriatal dopaminergic pathway. The insidious onset, asymmetry, and age group suggest a neurodegenerative cause. No drug history of DRBAs, no features of Parkinson-plus (no early falls, no vertical gaze palsy, no autonomic failure, no cerebellar signs). Most likely diagnosis: idiopathic Parkinson's disease. Alternatives: drug-induced parkinsonism (no DRBA exposure — less likely); Parkinson-plus if levodopa response is poor. Investigations: DAT-SPECT if diagnostic uncertainty remains; MRI brain to exclude structural cause.'
SELF-CHECK
A 55-year-old woman presents with a 2-year history of right arm tremor that is worst when she holds her arm outstretched. On examination, there is no tremor at rest. Rapid alternating hand movements are slightly irregular but not fatiguing. The rest of the neurological examination is normal. Her mother had a similar tremor. What is the most likely anatomical basis and diagnosis?
A. Basal ganglia dopaminergic deficit — early asymmetric Parkinson's disease
B. Cerebellar pathway dysfunction — early multiple system atrophy, cerebellar type
C. No basal ganglia or cerebellar structural lesion — essential tremor with normal extrapyramidal and cerebellar examination
D. Cortical myoclonus — frontal lobe dysfunction
Reveal Answer
Answer: C. No basal ganglia or cerebellar structural lesion — essential tremor with normal extrapyramidal and cerebellar examination
Postural tremor (present when holding position, absent at rest) with no bradykinesia (no fatiguing on rapid alternating movements), no rigidity, no other neurological signs, bilateral predilection, and positive family history is essential tremor. Essential tremor is not caused by a structural lesion of the basal ganglia or cerebellum demonstrable on imaging — it reflects an abnormality of cerebellar-thalamo-cortical oscillatory circuits but does not have the cardinal features of cerebellar disease (intention tremor on finger-nose, dysmetria, ataxia) or parkinsonism (bradykinesia, rigidity, rest tremor). PD would show rest tremor that disappears or reduces with voluntary movement, not a purely postural tremor.
Self-Assessment: Practising the Structured Clinical Evaluation
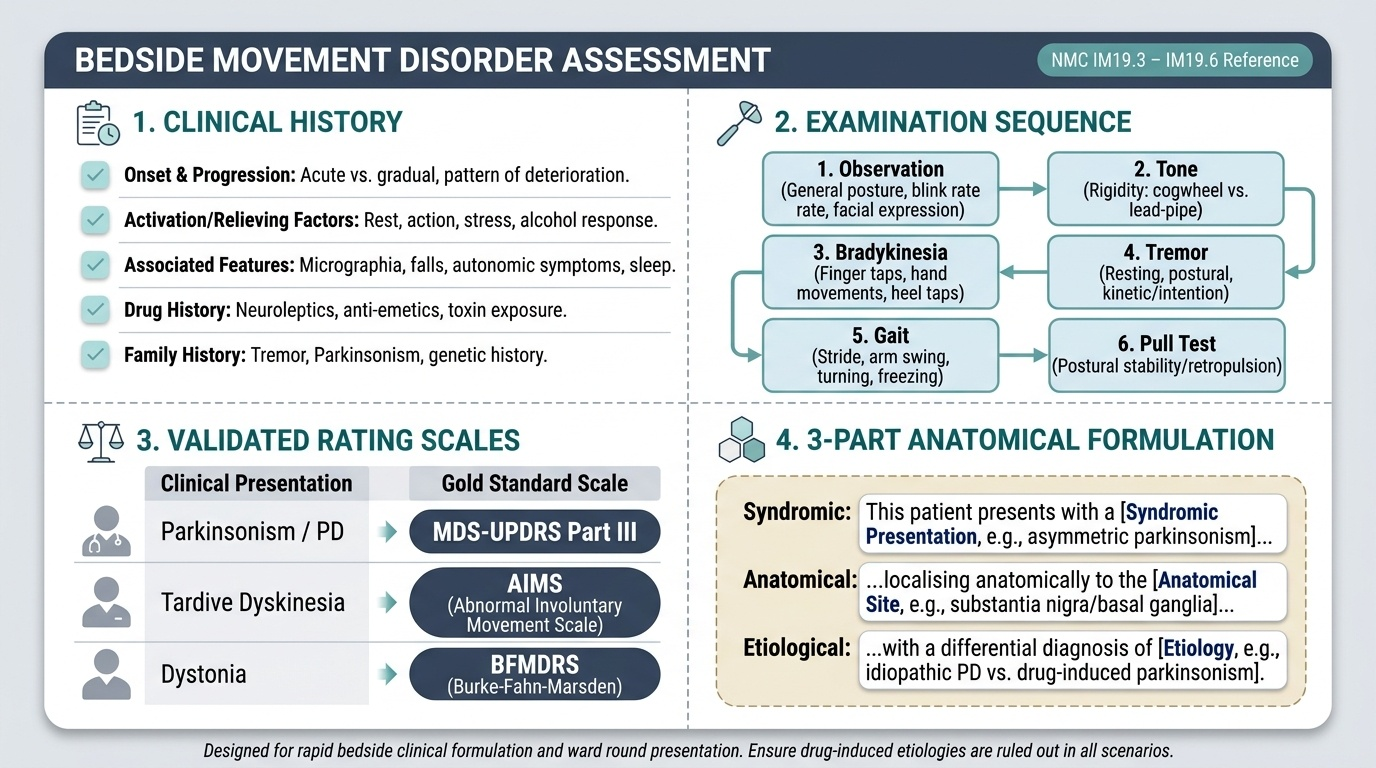
At this stage you have covered all components of the structured clinical evaluation for movement disorders: the focused history (onset, progression, precipitating/aggravating/relieving factors, associated symptoms, drug history), the systematic examination (general observation, tone assessment, bradykinesia testing, tremor characterisation, gait analysis, postural stability), the use of validated rating scales (MDS-UPDRS Part III for parkinsonism), and the three-part anatomical formulation. The self-assessment scenarios below ask you to apply each of these skills to a simulated patient and generate the clinical formulation before reading the analysis. This consolidates the procedural knowledge required for NMC IM19.3 through IM19.6 at the SH (Skills and Understanding in actual clinical settings) level. Practise verbalising the formulation as you would present it on a ward round or to a specialist.
Provided image
Scenario A: A 67-year-old man is referred with tremor. History: tremor noticed 4 years ago in the right hand; it is most prominent when he is sitting quietly watching television, and disappears when he reaches for his cup. He also notes his handwriting has become very small (micrographia). His wife reports he walks slowly and has fallen twice in the past year. He is on no medications. Examination: mask-like facies, reduced blink rate, hypophonic monotone speech, cogwheel rigidity both wrists (right > left), finger tapping shows fatiguing with progressive amplitude decrement at 10 repetitions, rest tremor right hand 4–6 Hz, gait shuffling with reduced bilateral arm swing (right > left), pull test shows 3 retropulsive steps before catching himself. No cerebellar signs.
Formulation: Anatomically: hypokinetic-rigid syndrome with rest tremor → basal ganglia (nigrostriatal pathway). Asymmetric (right > left) from onset, insidious onset over 4 years, progressive — neurodegenerative process. No drug exposure, no red flags for Parkinson-plus (no early falls before 3 years, no vertical gaze palsy, no prominent autonomic failure — though he does have some postural instability at 4 years into disease). Most likely: idiopathic Parkinson's disease. MDS-UPDRS Part 3 should be scored; levodopa challenge will confirm dopaminergic responsiveness. DAT-SPECT may confirm presynaptic dopaminergic deficit if clinical diagnosis is uncertain.
Scenario B: A 14-year-old girl is brought by her parents with 'funny movements' for 3 weeks. She had a sore throat treated with amoxicillin one month ago. Examination: she is restless with irregular, random, flowing movements of the limbs and face that shift unpredictably from limb to limb (chorea). Grip on examination is irregular (milkmaid sign). She is emotionally labile. Neurological examination otherwise normal. Heart: a soft systolic murmur is heard at the apex. ESR elevated; ASOT titre elevated.
Formulation: Anatomically: hyperkinetic disorder (chorea) → basal ganglia (striatal involvement). Acute/subacute onset (weeks) after streptococcal pharyngitis → autoimmune/post-infectious process (anti-basal-ganglia antibodies). Most likely: Sydenham's chorea (part of acute rheumatic fever — Duckett Jones criteria: chorea as a major criterion, murmur suggesting carditis as another major criterion, elevated ASOT as a minor criterion). Echocardiography to assess valvular damage. Penicillin to eradicate residual streptococcus; monthly benzathine penicillin prophylaxis for 5–10 years or until 21 years of age (whichever is longer) to prevent recurrence and progression of rheumatic heart disease.
Scenario C: A 30-year-old woman presents with involuntary turning of her head to the right for 6 months, which she describes as getting worse when she is tired and improving when she 'touches her chin.' Examination: the head is turned to the right with rotational torticollis; the right sternocleidomastoid is hypertrophied. She can temporarily reduce the head turning by placing her finger on the right side of her face (sensory trick — geste antagoniste). The rest of the neurological examination is normal. No family history. No drug exposure.
Formulation: Anatomically: focal dystonia (cervical dystonia / torticollis) → basal ganglia/motor circuit dysfunction localised to the cervical region. Sensory trick confirms dystonia (specific to this phenomenological type). Age-onset 30s, progressive, no secondary cause identified on history — idiopathic focal cervical dystonia (most likely primary cervical dystonia). First-line treatment: botulinum toxin injection into affected muscles (right sternocleidomastoid and contralateral splenius capitis). Refer to movement disorder specialist for injection series and interval assessment.
CLINICAL PEARL
The most powerful single observation in a movement disorder consultation is watching the patient walk in through the door before formal examination begins. A skilled neurologist can often characterise the movement disorder — and even narrow the differential — before asking a single question. Reduced arm swing asymmetrically (right arm not swinging → right-sided basal ganglia disease, i.e., left-sided Parkinson's), stooped posture, small shuffling steps, and hypomimia are all visible in the first 10 seconds of observation. Train your eyes to be diagnostic instruments.
For the MDS-UPDRS Part 3 examination, the single most sensitive item for detecting early PD is finger tapping (Item 3.4) — specifically the fatiguing phenomenon (progressive decrease in amplitude with repetition). Patients often do not subjectively feel their finger movements are slowing down, so the observation of fatiguing on repeated tapping is more sensitive than patient-reported bradykinesia. Always test this bilaterally and compare — the asymmetry is as informative as the absolute score.