Page 5 of 24
IM2.6-9 | ACS Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit and document a structured history for suspected ACS including onset, character of pain, radiation, associated symptoms, risk factors, and prior cardiac history
- Perform and document a focused cardiovascular and vascular examination appropriate to ACS presentation
- Generate and prioritise a differential diagnosis for acute chest pain using a 'cannot miss, most likely' framework
- Distinguish stable angina, unstable angina, NSTEMI, and STEMI based on clinical features alone
INSTRUCTIONS
Clinical evaluation of suspected ACS is a time-critical skill — your history and examination findings in the first 10 minutes determine triage, investigation priority, and reperfusion eligibility. This module builds the structured clinical reasoning framework for chest pain evaluation, equipping you to distinguish life-threatening causes from benign ones and to differentiate across the ACS spectrum using clinical features alone.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 35 — Chest Pain (textbook)
- API Textbook of Medicine, 10th ed., Ch. on Acute Coronary Syndromes (textbook)
- Davidson's Principles & Practice of Medicine, 24th ed., Ch. 18 — Cardiology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 11 PM in the emergency department. A 55-year-old man walks in holding his chest, pale and diaphoretic. He says the pain started two hours ago while he was watching television — 'a heavy pressure, like someone sitting on my chest' — radiating to both arms and the jaw. His wife adds that he looked grey and vomited once. His pulse is 92/min and regular, blood pressure 140/88 mmHg. You have two minutes before the ECG machine arrives. What are the five most important questions you need answered — and what examination findings in the next three minutes will change his immediate management? Your clinical evaluation in this window is not merely documentation: it determines whether this man goes immediately to the catheterisation laboratory or receives thrombolysis, whether he needs urgent pacing, and whether his risk of cardiogenic shock requires pre-emptive intervention. This module builds the systematic skill set for ACS clinical evaluation — history, examination, differential diagnosis construction, and clinical ACS classification — to equip you for exactly this scenario.
WHY THIS MATTERS
The NMC competencies IM2.6–2.9 are designated at the SH (Skill and Higher) level — the highest competency tier — meaning clinical evaluation of ACS is not merely a knowledge domain but a practised skill that you must be able to perform, demonstrate, and document in real patient encounters. The ability to elicit a structured chest pain history, perform a focused cardiovascular examination, generate a prioritised differential, and clinically distinguish stable angina from ACS is a threshold capability for any final-year student entering clinical rotations in general medicine, emergency medicine, and surgery. In India, where the majority of STEMI patients first arrive at non-catheterisation-capable district hospitals, the clinical evaluation by a final-year student or junior doctor is often the first triage decision — with direct consequences for reperfusion timing.
RECALL
Recall from the preceding module that ACS comprises three entities: STEMI (complete occlusion, ST elevation), NSTEMI (partial occlusion, troponin elevation without ST elevation), and unstable angina (transient occlusion, no troponin rise). The coronary territories govern which leads show ischaemic changes: inferior wall → RCA (leads II, III, aVF); anterior wall → LAD (V1–V4); lateral wall → LCx (I, aVL, V5–V6). From your clinical skills training, recall the SOCRATES mnemonic for pain history (Site, Onset, Character, Radiation, Associated symptoms, Timing, Exacerbating/relieving factors, Severity). The cardiovascular examination sequence moves from inspection to palpation of the praecordium, auscultation of heart sounds and murmurs, and assessment of peripheral vasculature and venous pressure. Keep these structural anchors in mind as you build the ACS-specific clinical reasoning layer.
Clinical Indication and Urgency of ACS Evaluation
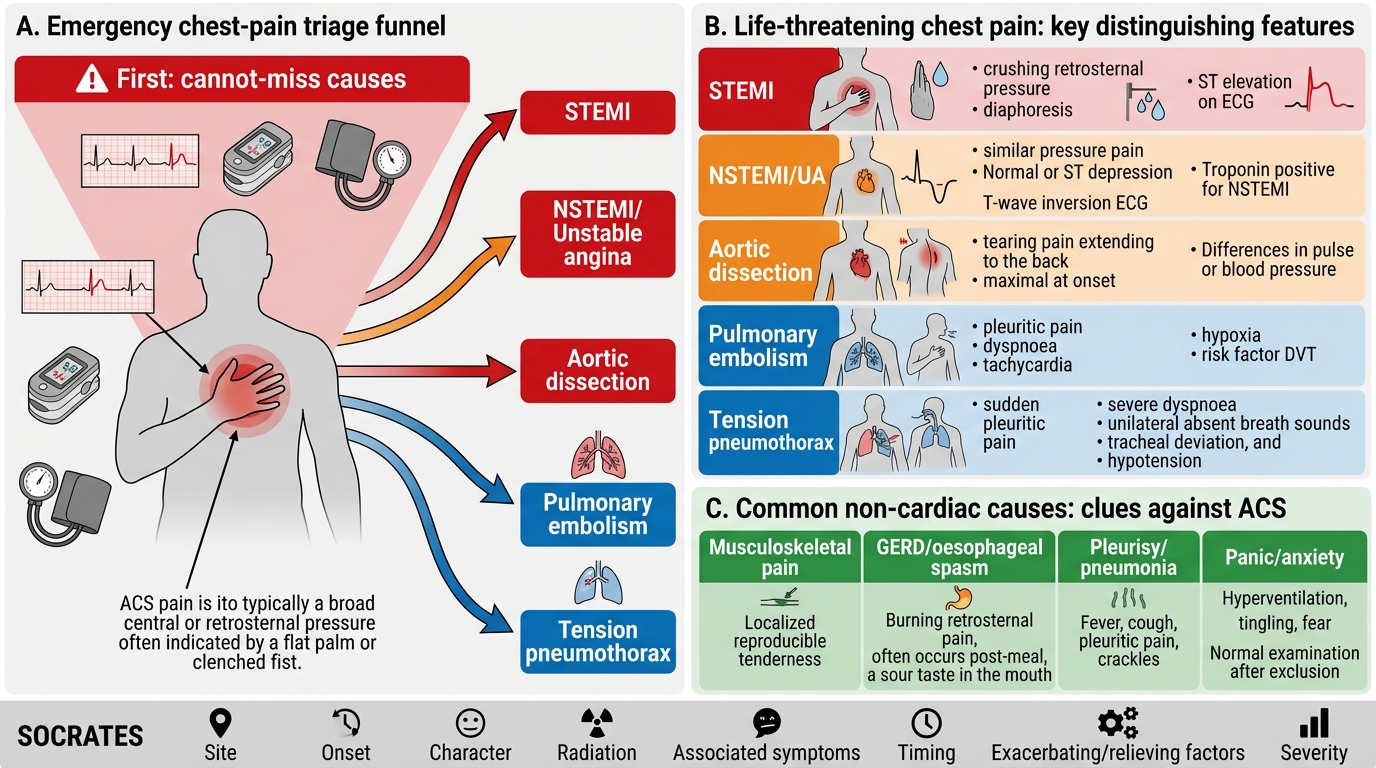
Acute chest pain is the cardinal presenting symptom of ACS, but it is also a symptom shared by a broad spectrum of conditions — some immediately life-threatening, some entirely benign. The clinical indication for a structured ACS evaluation is any presentation of chest, upper abdominal, jaw, arm, or back pain that is new, unexplained, and cannot be confidently attributed to a non-cardiac cause on first assessment. The urgency of the evaluation is determined by the pre-test probability of a life-threatening cause — and in the emergency setting, a systematic 'cannot miss' approach is mandatory.
The life-threatening causes of acute chest pain that must not be missed — the 'cannot miss' diagnoses — form a short list that every final-year student must hold in immediate recall:
- STEMI — complete coronary occlusion; time-critical for reperfusion within 120 minutes (total ischaemic time <12 hours for benefit)
- NSTEMI / Unstable angina — partial/transient occlusion; requires urgent risk stratification and early invasive strategy
- Aortic dissection — tearing chest pain radiating to the back, unequal arm pulses, widened mediastinum; thrombolysis is catastrophically contraindicated and must be excluded before treating as STEMI
- Pulmonary embolism — pleuritic chest pain, dyspnoea, tachycardia, haemoptysis, risk factors (immobilisation, DVT, malignancy, oral contraceptives)
- Tension pneumothorax — sudden pleuritic pain, absent breath sounds unilaterally, tracheal deviation, haemodynamic collapse
- Oesophageal rupture (Boerhaave syndrome) — severe retrosternal pain after forceful vomiting, subcutaneous emphysema
Note that aortic dissection deserves special emphasis in the ACS context: a type A dissection involving the coronary ostia may produce ECG changes and troponin elevation mimicking STEMI. Administering thrombolysis to a patient with aortic dissection causes catastrophic haemorrhage. The clinical red flags — tearing quality, maximal at onset, radiation to the back, unequal blood pressures in both arms, pulse deficits, and new aortic regurgitation murmur — must be actively sought before the thrombolytic decision.
Common but less immediately dangerous causes in the differential include musculoskeletal chest pain (costochondritis, rib fracture), pleuritis, pericarditis, oesophageal spasm, GORD, anxiety/hyperventilation, and herpes zoster. These are diagnoses of exclusion in the acute setting — never assume a benign cause until the dangerous ones are excluded.
Chest Pain Differential: Cannot-Miss vs Common Causes
Governing Principles: Structured Chest Pain History
The history in suspected ACS has two simultaneous purposes: to characterise the pain and associated symptoms with sufficient precision to distinguish ACS from other causes, and to identify clinical features that risk-stratify the patient and guide immediate management decisions (reperfusion eligibility, anticoagulation safety, CCU admission). A structured approach ensures that every critical element is captured in a time-pressured emergency setting.
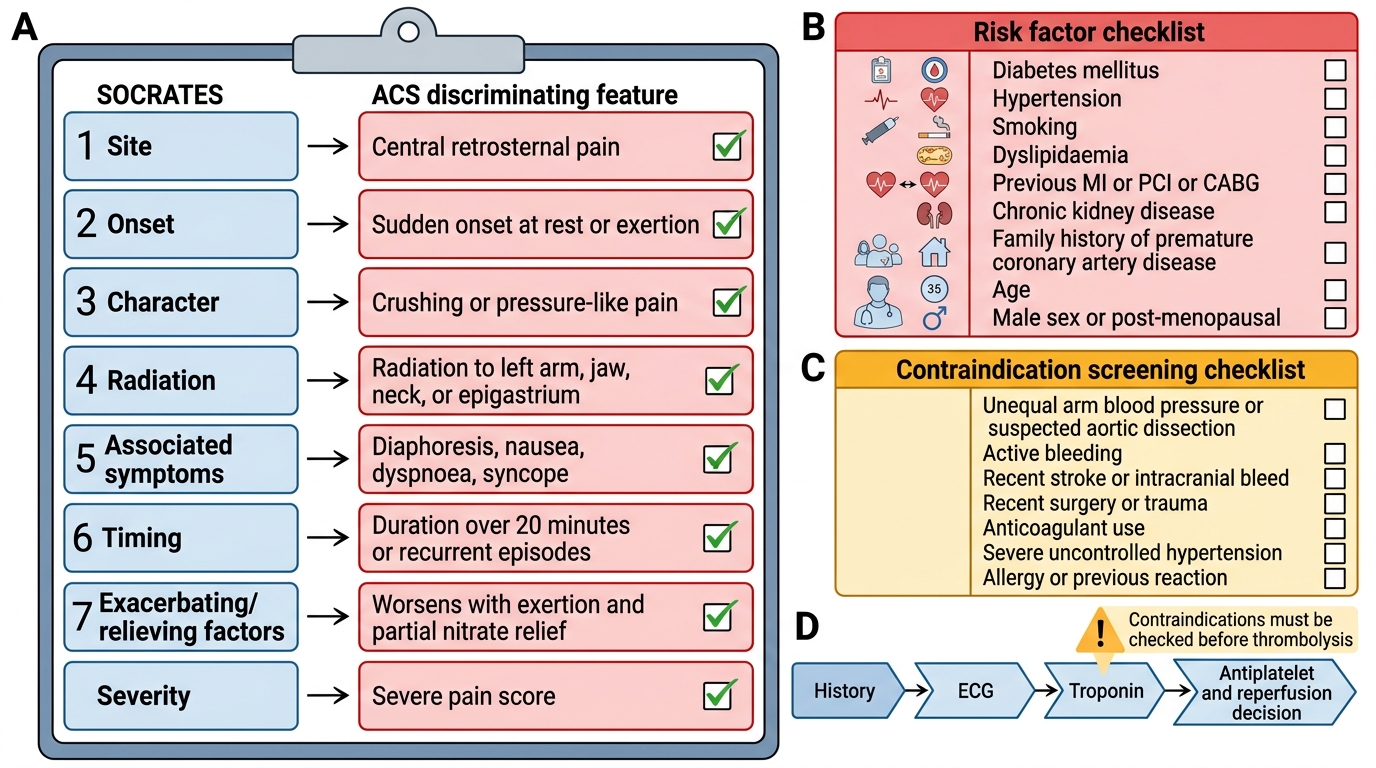
The SOCRATES framework applied to ACS chest pain:
Site: Classical ischaemic pain is central or retrosternal — a broad, diffuse discomfort that the patient typically indicates with a flat palm or clenched fist (Levine's sign) rather than a pointed finger. Localised, well-defined, point-tenderness reproducible with palpation is more consistent with musculoskeletal or pleuritic cause. Pain that migrates or changes location during the history suggests dissection.
Onset: ACS pain typically builds over minutes rather than reaching maximum intensity instantaneously (unlike aortic dissection, which is maximal at onset — 'tearing from the chest to the back') or suddenly with exertion and then resolving (stable angina). Onset at rest or during light activity is more concerning than pure exertional onset with immediate relief.
Character: The classic descriptor is pressure, heaviness, tightness, or squeezing — often described as 'elephant sitting on the chest', 'a vice', or 'a band around the chest'. Sharp, stabbing, or knife-like pain is less typical of ACS (though not excluding) and more consistent with pericarditis, pleuritis, or musculoskeletal cause. However, never dismiss atypical descriptors in high-risk patients — diabetics, elderly women, and patients with autonomic neuropathy frequently describe ischaemic pain as 'burning', 'indigestion', or 'breathlessness without pain'.
Radiation: Ischaemic pain classically radiates to the left arm (ulnar aspect), both arms, jaw, or neck. Radiation to the back is the hallmark of aortic dissection. Right shoulder radiation may suggest hepatobiliary cause.
Associated symptoms: This is arguably the most discriminating part of the ACS history:
- Diaphoresis (cold sweat) — a highly specific marker of sympathetic activation accompanying severe ischaemia; significantly increases pre-test probability of ACS
- Dyspnoea — may reflect acute LV dysfunction or pulmonary oedema complicating large MI; may be the predominant symptom in diabetic or elderly patients ('angina equivalent')
- Nausea and vomiting — common in inferior STEMI (RCA occlusion activates the Bezold-Jarisch reflex via vagal activation from the inferior wall)
- Syncope or pre-syncope — may indicate haemodynamic compromise or an arrhythmia (complete heart block with inferior MI, VF with anterior MI)
- Palpitations — suggest arrhythmia complicating ischaemia
- Haemoptysis or pleuritic component — raises PE probability
Timing: Duration matters critically. Stable angina resolves within 5 minutes with rest or sublingual nitrate. Rest pain lasting >20 minutes is a defining feature of unstable angina/NSTEMI and indicates ACS until proven otherwise. Duration of STEMI symptoms determines reperfusion eligibility — beyond 12 hours of symptoms, the myocardium may have completed necrosis and primary PCI benefit diminishes (though evidence supports PCI up to 24 hours if symptoms or evidence of ongoing ischaemia persist).
Exacerbating and Relieving factors: Stable angina is precipitated by exertion, cold, and emotional stress, and relieves promptly (<5 min) with rest or sublingual nitrate. ACS pain may not fully respond to nitrate, may occur at rest, and has no consistent relationship to exertion. Positional variation (better sitting forward) suggests pericarditis. Pain worsened by breathing suggests pleuritis or pericarditis.
Severity: Use a numeric scale (0–10 NRS or visual analogue scale) both for documentation and for tracking response to analgesia. Ischaemic pain is typically 7–10/10 — severe pain that the patient cannot ignore.
The critical IHD risk factor history must be obtained in parallel:
- Diabetes mellitus (increases silent ischaemia risk — atypical presentations are the norm)
- Hypertension (documented systolic >180 mmHg is a relative contraindication to thrombolysis)
- Smoking (current or recent) and pack-year history
- Hypercholesterolaemia and current statin use
- Family history of premature CAD (first-degree relative MI <55 M, <65 F)
- Prior cardiac history: previous MI, PCI/stenting, CABG (which vessel? any in-stent restenosis?), known coronary anatomy
- Medication history: current antiplatelet agents (aspirin, clopidogrel/ticagrelor — affects loading dose decision), anticoagulants (warfarin/DOAC — INR if warfarin, timing of last DOAC dose — affects procedural bleeding risk), nitrates, beta-blockers
- Contraindications to thrombolysis: recent surgery (<2 weeks), head injury/stroke (<3 months), active bleeding, severe hypertension (>180/110 mmHg uncontrolled)
Focused ACS History Checklist
Procedure: Focused Cardiovascular Examination in ACS
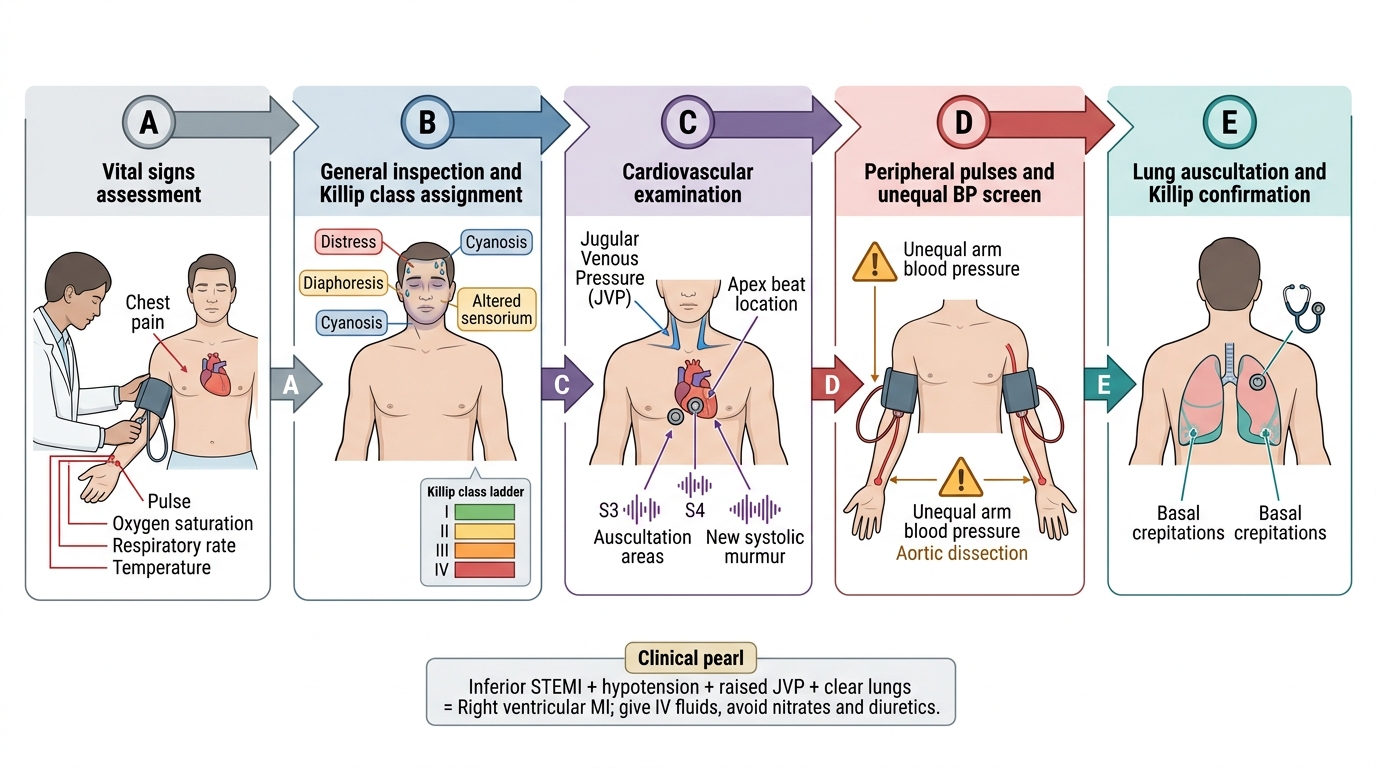
The physical examination in suspected ACS serves two purposes simultaneously: to identify signs that confirm or challenge the ACS diagnosis, and to detect complications of MI (haemodynamic compromise, acute LV failure, mechanical complications) that require immediate intervention. A focused but systematic examination can be completed within 3–5 minutes without sacrificing critical information. The examination is not a formality — it answers specific management-critical questions: Is this patient in cardiogenic shock? Is there evidence of right ventricular infarction requiring fluids rather than diuretics? Does the haemodynamic picture suggest a mechanical complication such as papillary muscle rupture or ventricular septal defect? Is the unequal arm blood pressure that would contraindicate thrombolysis present? Each examination finding either confirms or excludes a specific diagnosis or complication, and the sequence below is designed to prioritise those findings.
General appearance and vital signs: This is the first and most revealing 30 seconds of the examination. Note immediately: diaphoresis (cold, clammy skin = sympathetic activation, high ACS probability), pallor (anaemia, low cardiac output, or shock), cyanosis (severe hypoxia from acute pulmonary oedema), and the patient's level of distress. Vital signs define haemodynamic status:
- Heart rate: tachycardia (>100) may indicate sympathetic activation, LV failure, or arrhythmia; bradycardia with inferior MI suggests sinus node ischaemia or complete heart block (RCA supplies SA and AV nodes in 90% of people)
- Blood pressure: hypotension (systolic <90 mmHg) with tachycardia suggests cardiogenic shock (Killip class IV) — a life-threatening emergency; unequal blood pressure in both arms (>20 mmHg difference) is the key examination finding for aortic dissection and must not be missed before thrombolysis
- Respiratory rate: tachypnoea suggests acute pulmonary oedema or PE
- Oxygen saturation: SpO2 <94% requires supplemental oxygen
- Temperature: fever may suggest pericarditis (days after MI — Dressler syndrome) or an infectious cause mimicking ACS
The Killip classification uses clinical examination findings to stratify acute haemodynamic severity at presentation and predicts 30-day mortality:
- Killip class I: no signs of heart failure (no rales, no S3) — 30-day mortality ~6%
- Killip class II: mild-moderate heart failure — basal crepitations (rales in lower lung fields), S3 gallop, JVP elevated — mortality ~17%
- Killip class III: severe heart failure — pulmonary oedema (bilateral crepitations extending to mid-zone or beyond, marked dyspnoea) — mortality ~38%
- Killip class IV: cardiogenic shock — hypotension (systolic <90 mmHg) + evidence of poor peripheral perfusion (cold extremities, oliguria, confusion) ± pulmonary oedema — mortality ~67%
Assigning Killip class at admission is a mandatory part of ACS documentation — it enters the GRACE score and determines management intensity.
Praecordial examination:
- Inspection: look for abnormal pulsations, visible apex beat displacement (cardiomegaly from prior MI)
- Palpation: locate the apex beat (normal: 5th intercostal space, midclavicular line; displaced laterally suggests LV dilatation); palpate for a parasternal heave (RV enlargement), a systolic thrill (suggests acute MR or VSD from papillary muscle rupture/IVS rupture — mechanical complications)
- Percussion: not routinely performed in acute evaluation; cardiac dullness area can be assessed if pericardial effusion is suspected
- Auscultation: the most critical component
- Heart sounds: S1 and S2 — diminished in LV dysfunction; S3 gallop = LV failure (pathological in adults); S4 = stiff, non-compliant LV (common in hypertension and acute ischaemia)
- New murmurs: a new pansystolic murmur at the apex radiating to the axilla = acute mitral regurgitation (papillary muscle ischaemia/rupture — occurs 2–5 days post-MI); a new harsh pansystolic murmur at the left sternal border = ventricular septal defect (VSD) from septal rupture; an early diastolic decrescendo murmur at the left sternal border = aortic regurgitation (may accompany aortic dissection, or rarely be a pre-existing finding); a pericardial friction rub = pericarditis (may be early Dressler syndrome or viral pericarditis)
- Document whether new murmurs are present: their detection changes the diagnosis and management immediately
Peripheral vascular examination:
- Peripheral pulses: assess all major peripheral pulses (radial, brachial, femoral, popliteal, dorsalis pedis, posterior tibial); absent/diminished pulses suggest peripheral arterial disease (marker of diffuse atherosclerosis) or, crucially, pulse deficits suggesting aortic dissection
- Jugular venous pressure (JVP): elevated in right heart failure; paradoxically elevated in inferior MI with right ventricular infarction (JVP rises with inspiration — Kussmaul sign); a normal or low JVP with hypotension in inferior MI is a classic triad suggesting right ventricular MI (managed with IV fluids, NOT diuretics)
- Peripheral oedema: pitting oedema of ankles suggests chronic heart failure; its presence alters the differential diagnosis
- Lung bases: auscultate for crepitations (fine inspiratory crackles = pulmonary oedema), absent breath sounds (pleural effusion or pneumothorax), or pleural rub (pleuritis, infarction)
ACS-Focused Physical Examination Sequence
SELF-CHECK
A 60-year-old man with inferior STEMI presents with hypotension (BP 80/60 mmHg), bradycardia (HR 48/min), elevated JVP, and clear lung fields. What is the most likely complication and what is the CORRECT initial management?
A. Cardiogenic shock from LV failure — start IV dobutamine and furosemide
B. Right ventricular MI — administer IV fluid bolus and avoid diuretics
C. Complete heart block — immediate temporary pacing without fluid
D. Aortic dissection — urgent CT aortography
Reveal Answer
Answer: B. Right ventricular MI — administer IV fluid bolus and avoid diuretics
The triad of hypotension + elevated JVP + clear lung fields in the context of inferior STEMI is the classic presentation of right ventricular (RV) infarction. The RCA supplies the RV in most individuals; RV infarction causes RV failure with impaired preload delivery to the left side. The key distinguishing feature from cardiogenic LV shock is the clear lung fields — if it were LV failure (Killip III/IV), there would be pulmonary oedema. Management: IV fluid boluses (to maintain RV preload), avoid nitrates and diuretics (which reduce preload catastrophically), and reperfuse urgently (primary PCI). ST elevation in right-sided lead V4R confirms RV involvement. Complete heart block may coexist but the primary haemodynamic driver here is RV failure — fluids are appropriate.