Page 6 of 24
IM2.6-9 | ACS Clinical Evaluation — SDL Guide (Part 2)
Interpretation of Findings: Differential Diagnosis Construction
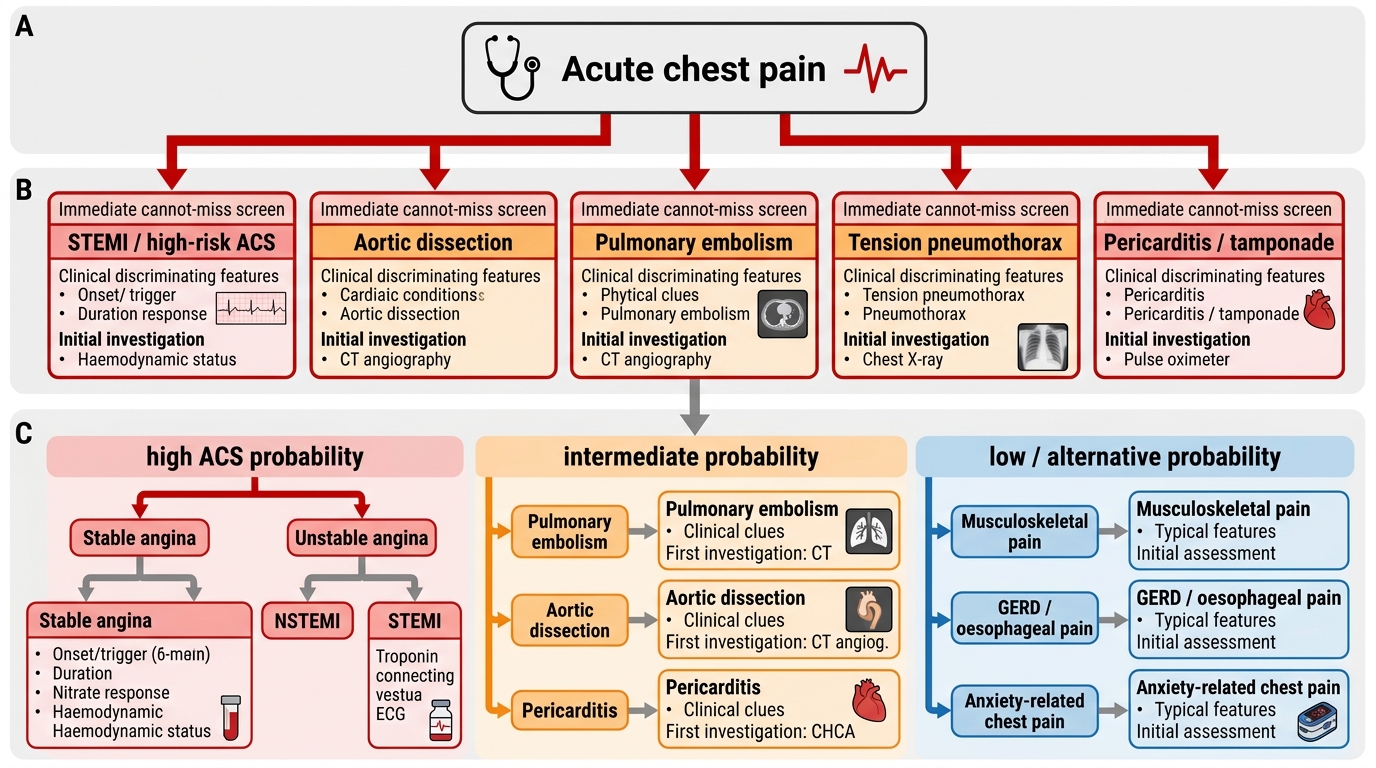
Constructing a differential diagnosis for acute chest pain requires simultaneous application of two frameworks: a 'cannot miss' urgency filter and a probability filter based on the pre-test likelihood from the clinical features assembled. These frameworks operate in sequence — the cannot-miss diagnoses are always considered first regardless of probability, because the consequence of missing them is catastrophic and irreversible. Once the immediately life-threatening causes are either confirmed or adequately excluded based on initial clinical assessment, the probability-weighted differential guides further investigation. The discipline of structured differential construction is not merely an academic exercise — in the emergency setting, presenting the differential in a cant-miss-first order to a supervisor communicates clinical reasoning and flags the urgency of investigation. Students who habitually lead with the reassuring diagnosis and bury the dangerous one create conditions for missed diagnoses and delayed treatment. The following framework trains the correct habit.
The 'cannot miss' filter (discussed fully in arc step 1) requires active consideration and exclusion of: STEMI, NSTEMI/UA, aortic dissection, pulmonary embolism, and tension pneumothorax at every presentation. The clinical features that trigger immediate concern for each are:
- STEMI/NSTEMI: central chest pressure, radiation, diaphoresis, risk factors → ECG immediately
- Aortic dissection: tearing quality, maximal at onset, back radiation, unequal arm BP, pulse deficits, new AR murmur → ECG (to exclude STEMI), then CT aortography
- PE: pleuritic pain + dyspnoea + tachycardia + risk factors (immobility, DVT history, malignancy, OCP) → oxygen, Wells score, D-dimer or CT-PA
- Tension pneumothorax: sudden severe chest pain, absent breath sounds unilaterally, tracheal deviation → clinical diagnosis, immediate decompression without waiting for CXR
Probability-based differential construction: after the cannot-miss screen, the differential is weighted by:
- ACS probability: high when — central pressure/tightness, radiation to jaw/arms, associated diaphoresis, duration >20 minutes, onset at rest in a patient with multiple IHD risk factors
- Pericarditis: sharp pleuritic pain, better sitting forward, pericardial friction rub, recent viral illness, fever; ECG shows saddle-shaped ST elevation in multiple leads without reciprocal changes
- Oesophageal/GORD: burning, related to meals, relieved by antacids, no diaphoresis, no radiation to arms, normal ECG
- Musculoskeletal: localised, reproducible with palpation, recent physical exertion or injury, no diaphoresis or haemodynamic change
- Anxiety/hyperventilation: young patient, situational trigger, circumoral tingling, no risk factors, rapid onset and offset
Prioritising the differential: the NMC competency IM2.8 specifically requires that you prioritise based on 'cannot miss', most likely, and severity. In clinical documentation and verbal presentation, this means:
1. Lead with the cannot-miss diagnosis you are actively evaluating (e.g., 'I am treating this as an inferior STEMI until the ECG proves otherwise')
2. State the most likely diagnosis based on the full clinical picture
3. List the diagnoses excluded or less likely and the clinical reasoning for their exclusion
A common error is inverting this hierarchy — presenting the most likely 'reassuring' diagnosis first while burying the cannot-miss concern at the bottom of the list. This inverted reasoning has caused deaths from missed aortic dissections and PEs in patients labelled with 'musculoskeletal chest pain' or 'GORD'.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
Clinical Prioritisation of Acute Chest Pain
Applied Practice: Distinguishing Stable Angina, UA, NSTEMI, and STEMI Clinically
The NMC competency IM2.9 specifically requires the ability to distinguish and differentiate stable angina, unstable angina, and AMI based on clinical presentation — that is, using history and examination alone, before ECG and biomarker results are available. This clinical-first classification is a foundational skill because it determines initial triage, immediate treatment priorities, and communication with the receiving team. In the real clinical environment, the ECG may take several minutes to arrive and the troponin result will not be available for at least 3 hours. In that window, the clinician's assessment of clinical ACS probability — derived from the history and examination — determines whether the patient is taken immediately to the resuscitation bay, given antiplatelet loading, and activates the reperfusion pathway, or whether they are observed in a lower-acuity area. Practising this clinical-first reasoning with a structured framework prevents both under-triage of high-risk presentations and over-investigation of low-risk cases.
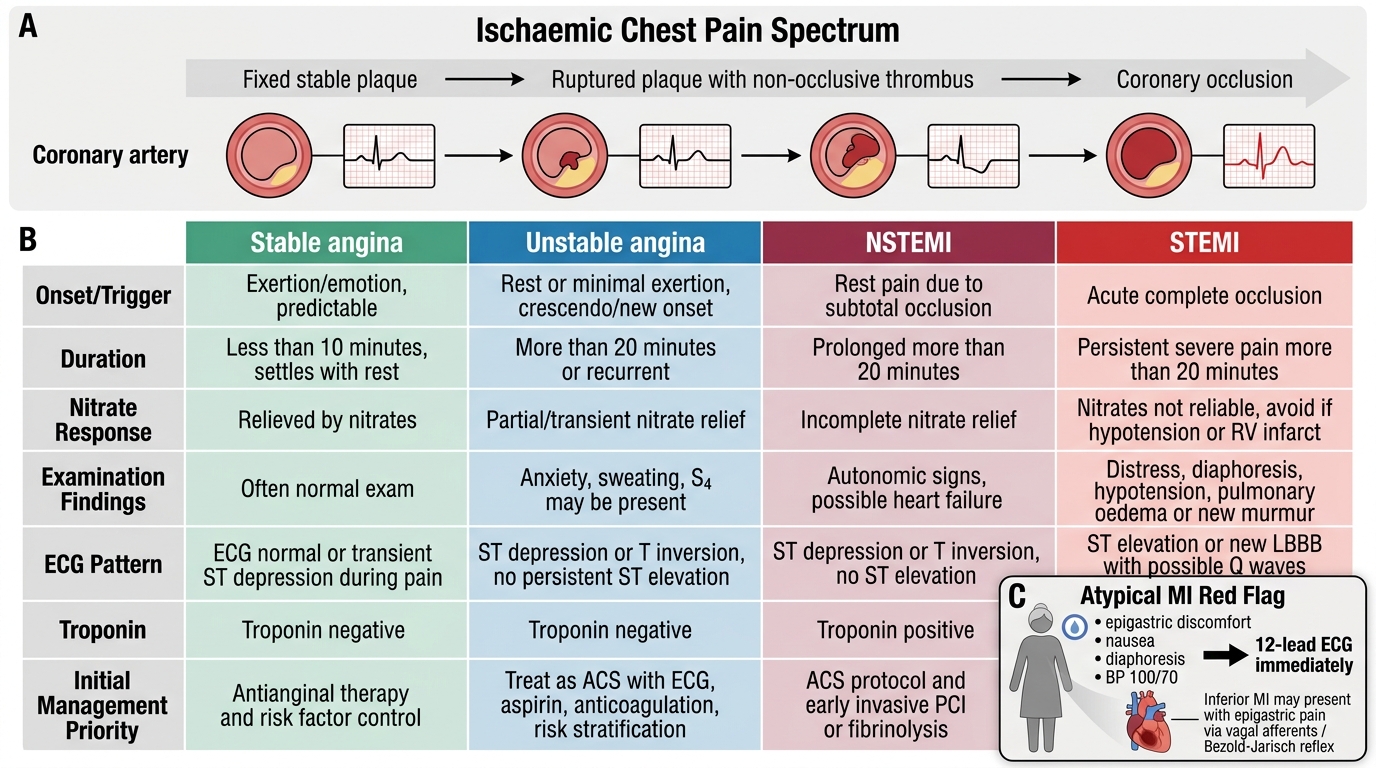
The four key clinical discriminants — onset/trigger, duration, response to nitrate, and haemodynamic/examination findings — create a clinical matrix that allows rapid classification:
Stable (chronic) angina:
- Onset: always triggered by a consistent level of exertion, emotional stress, or cold exposure
- Duration: <5 minutes — pain resolves promptly with cessation of the trigger
- Response to nitrate: complete relief within 2–3 minutes of sublingual glyceryl trinitrate (GTN)
- Examination: typically normal between episodes; may have signs of risk factors (hypertension, xanthelasma, corneal arcus); no S3, no new murmurs
- Pattern: entirely predictable over weeks to months; Canadian Cardiovascular Society (CCS) class is stable
Unstable angina (UA):
- Onset: characteristically at rest (rest angina), or with minimal exertion that previously did not trigger pain (crescendo pattern), or as new-onset severe angina at CCS class III or IV
- Duration: >20 minutes if rest angina; may be shorter in crescendo pattern
- Response to nitrate: incomplete or absent relief with sublingual GTN — a clinical red flag
- Examination: often normal; the absence of examination findings does not reduce urgency; haemodynamic instability is uncommon but possible
- ECG (when available): may show transient ST depression or T-wave changes during pain, resolving between episodes; troponin is negative (normal on serial sampling)
NSTEMI:
- Clinically indistinguishable from UA on history and examination alone — the differentiation requires troponin measurement
- History is similar to UA: rest or minimal-exertion pain, incomplete nitrate response
- Examination: may show signs of LV dysfunction (S3, basal crepitations) if a large territory of subendocardial muscle is ischaemic; Killip class should be assessed
- The decision to treat as NSTEMI rather than UA is based on troponin positivity — but clinically, NSTE-ACS is managed the same way pending troponin results
STEMI:
- Onset: typically at rest (in the setting of spontaneous plaque rupture) or with moderate exertion; severe, sustained, unremitting pain
- Duration: >30 minutes of severe ischaemic pain unresponsive to nitrate in the large majority
- Character: typically the most severe chest pain the patient has experienced — 9–10/10 on NRS
- Associated symptoms: diaphoresis (highly sensitive for large MI), vomiting (especially inferior STEMI — Bezold-Jarisch reflex), dyspnoea (LV dysfunction), syncope (VF or complete heart block)
- Examination findings that distinguish STEMI from other ACS:
- Haemodynamic compromise: hypotension, Killip class III/IV in anterior MI involving large LAD territory
- S3 gallop: acute LV dysfunction
- New pansystolic murmur: papillary muscle ischaemia (MR) — peak incidence day 2–5 post-MI
- Elevated JVP + clear lungs: RV infarction (inferior STEMI with RCA occlusion)
- Pericardial rub: early pericarditis (day 1–2) or Dressler syndrome (weeks 2–8)
The atypical presentation problem in India: A substantial proportion of ACS presentations in India are atypical — particularly in diabetics, elderly patients, and women. Atypical presentations include: epigastric pain or discomfort (particularly inferior STEMI, where vagal activation produces epigastric pain and vomiting that can be mistaken for acute abdomen or GORD); breathlessness or fatigue as the sole symptom (angina equivalent, especially in patients with autonomic neuropathy); jaw or tooth pain without chest pain; left arm pain in isolation. In any diabetic or elderly patient with unexplained new dyspnoea, diaphoresis, epigastric pain, or presyncope — always obtain an ECG and troponin before attributing the symptoms to a non-cardiac cause.
Stable Angina and ACS: Clinical Comparison
SELF-CHECK
A 62-year-old woman with type 2 diabetes presents with 2 hours of epigastric discomfort, nausea, and diaphoresis. She denies any chest pain. She has a history of hypertension and a 30-pack-year smoking history. Her BP is 100/70 mmHg. The MOST important immediate step is:
A. Administer IV ranitidine and order a gastroscopy
B. Obtain a 12-lead ECG immediately — this presentation must be treated as ACS until proven otherwise
C. Order a serum lipase and ultrasound abdomen to exclude acute pancreatitis
D. Reassure the patient that atypical symptoms are unlikely to represent ACS in a woman
Reveal Answer
Answer: B. Obtain a 12-lead ECG immediately — this presentation must be treated as ACS until proven otherwise
Epigastric discomfort + diaphoresis + haemodynamic compromise (BP 100/70) in a diabetic woman with multiple IHD risk factors is an inferior STEMI until proven otherwise. Inferior MI (RCA occlusion) characteristically activates vagal afferents from the inferior wall, producing the Bezold-Jarisch reflex — nausea, vomiting, and epigastric pain without classic chest pressure. Diabetic neuropathy additionally blunts the chest pain perception. Diaphoresis in this context is a red flag for sympathoadrenal activation accompanying large ischaemia. A 12-lead ECG is the single most important immediate step — it will show ST elevation in II, III, aVF and will change all subsequent management. Delaying ECG to investigate gastrointestinal or biliary causes first in this clinical context is a preventable error that carries risk of fatal delay.
SELF-CHECK
A 50-year-old man presents with 25 minutes of severe central chest pressure at rest. He has a known history of stable angina (CCS class II) managed with isosorbide mononitrate and atenolol. He took one sublingual GTN tablet but the pain did not fully resolve. His BP is 138/84 mmHg, HR 78/min, SpO2 97%. Examination reveals an S4 gallop and no new murmurs. Which ACS category is MOST consistent with this clinical picture before investigations?
A. Stable angina — reassure and increase his nitrate dose
B. Unstable angina or NSTEMI — this is NSTE-ACS pending troponin result
C. STEMI — begin immediate reperfusion protocol without waiting for the ECG
D. Aortic dissection — unequal arm blood pressure must be checked before ECG
Reveal Answer
Answer: B. Unstable angina or NSTEMI — this is NSTE-ACS pending troponin result
Rest pain lasting >20 minutes with incomplete GTN response in a patient with previously stable angina represents either unstable angina (if troponin is negative) or NSTEMI (if troponin is elevated) — both are NSTE-ACS and are managed identically at this stage. The S4 gallop is consistent with ischaemia-related stiffening of the LV. The clinical picture does not suggest STEMI (which would require ECG confirmation of ST elevation before reperfusion) or dissection (no features pointing to dissection, but BP equality should be verified as part of a complete exam). The critical clinical point is that a change from stable to unstable pattern — rest onset, longer duration, incomplete GTN response — requires urgent evaluation and risk stratification as NSTE-ACS.
Self-Assessment: ACS Clinical Evaluation Integrated
This self-assessment section integrates all six arc steps — clinical indication, structured history principles, examination technique, differential diagnosis construction, and clinical ACS classification — into a set of structured scenarios designed to replicate the clinical reasoning demanded in the emergency department. For each scenario, form your clinical assessment before reading the analysis. The key disciplines being tested are: identifying cannot-miss diagnoses proactively, constructing the history to discriminate rather than merely describe, and assigning the correct ACS category based on clinical features before investigations are returned.
Scenario A: A 48-year-old male smoker presents with 40 minutes of central crushing chest pain radiating to the left arm, onset at rest, associated with profuse sweating and one episode of vomiting. He takes metformin for diabetes. On examination: BP 90/60 mmHg, HR 110/min, respiratory rate 26/min. JVP is elevated. You hear bilateral basal crepitations extending to mid-zone, and a soft S3. What is the Killip class, the most likely ACS category, and the immediate management priority?
Analysis: Killip class III (pulmonary oedema — bilateral crepitations + S3; hypotension makes it borderline Killip III/IV). The clinical presentation — central crushing pain, radiation, diaphoresis, vomiting, at rest, duration >20 min, haemodynamic compromise — is consistent with large STEMI (anterior or inferoposterior depending on ECG). Management priorities: immediate 12-lead ECG, supplemental oxygen if SpO2 <94%, IV access, analgesia (morphine titrated to response), aspirin 300 mg loading dose, and immediate activation of the reperfusion pathway — primary PCI or thrombolysis depending on centre capability and time from onset.
Scenario B: A 38-year-old woman on combined oral contraceptive pills presents with acute onset right-sided pleuritic chest pain and breathlessness that began 2 hours after a 14-hour international flight. She has no cardiac history, no IHD risk factors. BP 120/78 mmHg, HR 104/min, SpO2 92% on room air. Lung examination reveals a pleural rub at the right base and dullness to percussion at the right base.
Analysis: The cannot-miss diagnosis here is pulmonary embolism — not ACS. Clinical features: OCP use (thrombophilia risk), prolonged immobility (flight >6 hours), pleuritic (not pressure) pain, right-sided, tachycardia, low SpO2, pleural rub and dullness (pulmonary infarction with small haemorrhage → pleuritis and haemorrhagic pleural effusion). The Wells score for PE: HR >100 (+1.5), alternative diagnosis less likely (+3), immobilisation >3 days (+1.5) = 6 = high probability. Management: supplemental oxygen, IV access, LMWH anticoagulation, CT pulmonary angiography (CTPA) urgently. An ECG should still be performed (may show S1Q3T3, sinus tachycardia, right heart strain — V1 T-wave inversion) and troponin (elevated in large PE from RV strain), but these are supportive, not diagnostic.
Scenario C: A 72-year-old male ex-smoker with known hypertension presents with sudden severe tearing chest pain that was maximal at its very onset and radiates straight through to the interscapular back. He appears extremely distressed. BP right arm 190/110 mmHg, BP left arm 150/90 mmHg (difference of 40 mmHg systolic). Radial pulse is absent on the left. On auscultation, there is an early diastolic decrescendo murmur at the left sternal border.
Analysis: This is aortic dissection (type A — ascending aorta) until proven otherwise. Red flags: tearing quality, maximal at onset (contrast with ACS which builds over minutes), back radiation, unequal arm BPs (40 mmHg difference — diagnostic if >20 mmHg), absent radial pulse (subclavian involved), aortic regurgitation murmur (aortic root involvement). Do NOT give thrombolysis. Do not assume this is STEMI even if the ECG shows changes (dissection can involve coronary ostia → inferolateral territory ischaemia). Immediate management: IV analgesia, heart rate and blood pressure control (labetalol or esmolol to target HR <60/min, SBP 100–120 mmHg), urgent CT aortography, cardiothoracic surgical referral.
CLINICAL PEARL
The single most dangerous clinical error in ACS evaluation is thrombolysing an aortic dissection. The clinical features that should trigger dissection consideration before any thrombolytic decision are: pain quality that is tearing and maximal at onset, radiation to the back, unequal arm blood pressure (>20 mmHg difference), pulse deficit in any limb, and a new aortic regurgitation murmur. In India, where many STEMI patients are thrombolysed at district hospitals without immediate CT scanning, the clinical screen for dissection before thrombolysis is a life-saving habit — not optional.
Second pearl: the Bezold-Jarisch reflex — vagal activation from inferior wall ischaemia producing bradycardia, hypotension, nausea, and epigastric pain — is responsible for the high rate of inferior STEMI being initially diagnosed as 'acute abdomen' or 'gastroenteritis' in Indian emergency departments. Any patient presenting with unexplained epigastric pain + diaphoresis + haemodynamic instability needs an ECG within 2 minutes, not an ultrasound abdomen.