Page 18 of 24
IM2.18 | Dyslipidemia Management in IHD — SDL Guide (Part 2)
Management: Pharmacotherapy for Dyslipidaemia
The pharmacological management of dyslipidaemia follows a treatment intensification ladder: lifestyle modification as the foundation, followed by statin monotherapy, then statin combination with non-statin agents (ezetimibe, PCSK9 inhibitors), and specific agents for hypertriglyceridaemia and rare disorders. Understanding the mechanism, efficacy, dose-response relationship, key adverse effects, and monitoring requirements for each drug class is the core of IM2.18.
STATINS (HMG-CoA reductase inhibitors) — the cornerstone of dyslipidaemia pharmacotherapy:
Mechanism: statins inhibit HMG-CoA reductase, the rate-limiting enzyme in the mevalonate pathway for cholesterol synthesis. Reduced intracellular cholesterol upregulates hepatic LDLR expression → increased LDL clearance from plasma. Statins also have pleiotropic effects (independent of LDL reduction): anti-inflammatory (reduced CRP, IL-6), endothelial-stabilising (increased nitric oxide production), plaque-stabilising (reduced macrophage activity, thicker fibrous cap), and antithrombotic (reduced tissue factor expression).
LDL-C reduction by statin intensity:
- High-intensity statins (≥50% LDL reduction expected):
- Atorvastatin 40–80 mg daily (most widely used in India; reference statin for most trials)
- Rosuvastatin 20–40 mg daily (slightly more potent per mg; preferred when maximum LDL reduction is needed)
- Moderate-intensity statins (30–49% LDL reduction expected):
- Atorvastatin 10–20 mg, Rosuvastatin 5–10 mg, Simvastatin 20–40 mg (note: simvastatin 80 mg is no longer recommended due to high myopathy risk)
- Pravastatin 40–80 mg, Fluvastatin 80 mg, Pitavastatin 2–4 mg
- Low-intensity statins (<30% LDL reduction): Lovastatin 20 mg, Simvastatin 10 mg
Statin adverse effects and monitoring:
- Myopathy/statin-associated muscle symptoms (SAMS): the most clinically important adverse effect. Spectrum:
- Myalgia (muscle pain without CK elevation): most common; reported in 5–10% of patients in observational registries (lower in RCTs due to selection); often resolves with dose reduction or statin switching
- Myositis (myalgia + CK elevation): CK 3–10× ULN requires dose reduction; CK >10× ULN requires temporary statin discontinuation
- Rhabdomyolysis (severe muscle breakdown + CK >40× ULN + myoglobinuria + acute kidney injury): rare (<0.1%); potentially fatal; immediate statin discontinuation + IV fluids + renal support
- Risk factors for statin myopathy: high statin dose, advanced age, female sex, low BMI, hypothyroidism, CKD, drug interactions (CYP3A4 inhibitors — clarithromycin, azithromycin, diltiazem, verapamil, amiodarone, ketoconazole — increase plasma statin levels; simvastatin + amlodipine interaction; avoid simvastatin >20 mg with amlodipine)
- Management: baseline CK not routinely needed; check CK if symptoms develop; if CK <4× ULN and symptoms mild — continue statin with monitoring; if CK >4× ULN or symptoms significantly limiting — hold statin, switch to a different statin (inter-statin myopathy transfer rate is ~30%; try a less myopathic statin such as pravastatin or rosuvastatin); 'statin holiday' and rechallenge at lower dose
- Statin-induced liver enzyme elevation: asymptomatic transaminase elevation >3× ULN in <3% of patients; clinically significant hepatotoxicity is extremely rare (1:100,000); baseline LFTs before starting, then only if symptoms develop (not routine annual monitoring)
- New-onset diabetes: statins increase the relative risk of new-onset diabetes by ~10% (statin dose-dependent; more common with high-dose statins, existing pre-diabetes, and metabolic syndrome). Net benefit in high-risk patients far exceeds this risk (JUPITER trial: 1 new case of diabetes per 498 patient-years of treatment; 1 major cardiovascular event prevented per 155 patient-years). Monitor HbA1c annually in pre-diabetic patients on statins.
- Cognitive effects: post-marketing reports of memory impairment; rigorous RCT data (PROSPER, JUPITER) and the HOPE-3 trial show no excess cognitive impairment with statin therapy. FDA label includes a precautionary note but randomised evidence does not support routine concern.
EZETIMIBE:
Mechanism: inhibits intestinal cholesterol absorption by blocking the NPC1L1 transporter at the brush border of intestinal enterocytes; reduces cholesterol entering the enterohepatic circulation, which secondarily upregulates hepatic LDLR. Reduces LDL-C by approximately 15–20% as monotherapy; when added to maximally tolerated statin, provides an additional 18–24% LDL reduction (additive with statin — different mechanism).
Dose: 10 mg once daily (single tablet; fixed-dose combination with atorvastatin or rosuvastatin available).
Trial evidence: IMPROVE-IT trial (2015) — ezetimibe added to simvastatin in post-ACS patients reduced LDL-C further (53 → 50 mg/dL) and produced a modest but statistically significant 6.4% relative risk reduction in cardiovascular events at 7 years. This trial established the 'lower is better' principle for LDL and justified adding ezetimibe when statin alone is insufficient.
Adverse effects: well tolerated; slight increase in diarrhoea; rare cases of myopathy (very rare compared to statins); monitor LFTs if used with statins (additive hepatic risk, though still very low).
Indication: add to maximally tolerated statin when LDL-C target is not achieved; approved as monotherapy in statin-intolerant patients.
PCSK9 INHIBITORS (evolocumab, alirocumab):
Mechanism: monoclonal antibodies against PCSK9 (proprotein convertase subtilisin/kexin type 9), the hepatic protease that binds to LDLR and directs it to lysosomal degradation after LDL uptake. Inhibiting PCSK9 prevents LDLR degradation → more LDLR recycled to the hepatocyte surface → dramatically increased LDL clearance. Reduces LDL-C by 50–60% on top of maximally tolerated statin.
Dosing: evolocumab 140 mg SC every 2 weeks or 420 mg SC monthly; alirocumab 75 or 150 mg SC every 2 weeks.
Trial evidence: FOURIER trial (evolocumab, 2017) — 27,564 post-MI/stroke patients on statin; achieved median LDL-C 30 mg/dL; 15% relative risk reduction in primary MACE endpoint. ODYSSEY OUTCOMES (alirocumab, 2018) — post-ACS patients; achieved LDL-C 38 mg/dL; 15% MACE reduction + mortality benefit in patients with highest baseline LDL.
Adverse effects: injection site reactions (mild, local); rare neurocognitive concerns (not confirmed in RCTs). Extremely well tolerated.
Current indication: very high-risk patients (post-ACS, FH) in whom LDL-C target is not achieved on maximally tolerated statin + ezetimibe; approved by drug regulators globally. High cost limits availability in India — currently restricted to tertiary hospital use.
FIBRATES (fenofibrate, gemfibrozil):
Mechanism: PPARα agonists → increase lipoprotein lipase (LPL) expression (faster TG hydrolysis) + decrease VLDL synthesis + increase HDL-C synthesis (ApoA-I upregulation). Primary effect: TG reduction 30–50%; modest HDL increase (~10%); modest LDL reduction (~5–15%).
Dose: fenofibrate 145–200 mg daily (dose-reduce in CKD); gemfibrozil 600 mg BD (gemfibrozil interacts with statins — significantly increases statin plasma levels and myopathy risk; avoid gemfibrozil + statin combination).
Indication: severe hypertriglyceridaemia (TG >500 mg/dL — pancreatitis prevention is the primary goal); atherogenic dyslipidaemia (TG + low HDL pattern) as adjunct to statin. Do NOT use fenofibrate + statin in combination for cardiovascular event prevention without specific TG/HDL indication — ACCORD-Lipid trial (fenofibrate + simvastatin vs simvastatin alone in type 2 diabetes) showed no additional cardiovascular benefit.
Adverse effects: myopathy risk (especially gemfibrozil + statin); hepatotoxicity; cholelithiasis (increased bile lithogenicity); monitor LFTs, CK, creatinine.
OMEGA-3 FATTY ACIDS:
Mechanism: EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) reduce hepatic VLDL synthesis → TG reduction 20–30% at prescription doses. At very high doses (4 g/day icosapentaenoic acid — EPA only), EPA reduces cardiovascular events independently of TG lowering (REDUCE-IT trial, 2018 — 25% relative risk reduction in MACE in statin-treated patients with TG >150 mg/dL; mechanism controversial but possibly involves membrane phospholipid incorporation and anti-inflammatory effects).
Dosing: dietary omega-3 (fish oil supplements) at 1–3 g/day reduce TG modestly; prescription icosapentaenoic acid (EPA, Vascepa) 4 g/day for cardiovascular event reduction in high TG patients on statin (REDUCE-IT indication).
Adverse effects: fishy taste/eructation; minor bleeding tendency at high doses (caution with dual antiplatelet therapy); high DHA preparations may slightly raise LDL-C.
BILE ACID SEQUESTRANTS (cholestyramine, colestipol, colesevelam):
Mechanism: non-absorbable resins bind bile acids in the gut → interrupt enterohepatic circulation → liver increases cholesterol conversion to bile acids → upregulates LDLR. LDL reduction ~15–20%.
Use: limited by poor tolerability (bloating, constipation, drug interactions — interfere with absorption of warfarin, digoxin, thyroxine, fat-soluble vitamins); historical role in FH (before statins); colesevelam is better tolerated and now mainly used as add-on in FH when statin + ezetimibe + PCSK9i is insufficient.
NIACIN (nicotinic acid): Historically used for HDL raising (15–35% increase) and TG reduction; largely abandoned since AIM-HIGH and HPS2-THRIVE trials showed no additional cardiovascular benefit over statin therapy despite HDL elevation; significant adverse effects (flushing, hepatotoxicity, hyperglycaemia, gout). No longer recommended in routine dyslipidaemia management.
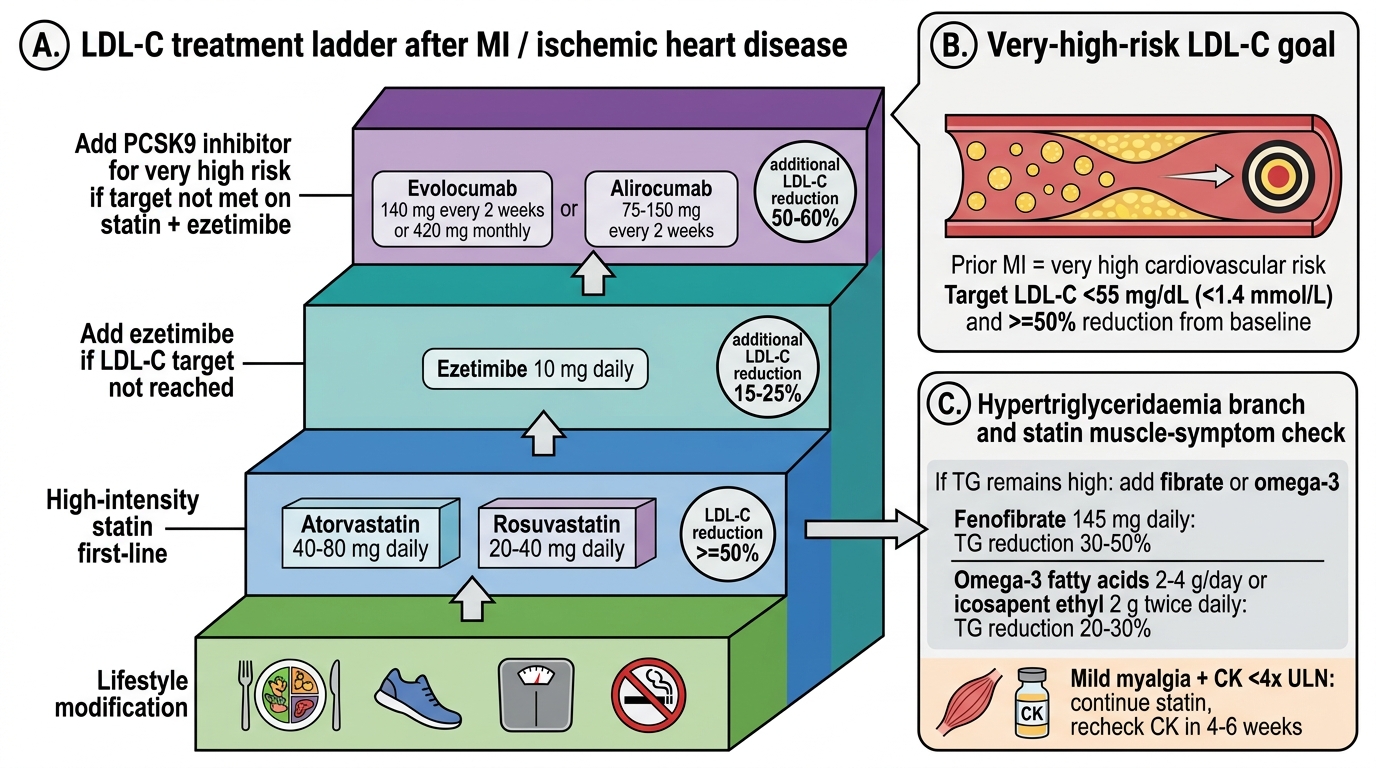
Dyslipidaemia Treatment Ladder After MI
SELF-CHECK
A 52-year-old woman with a prior MI (3 years ago) is on atorvastatin 80 mg daily. Her latest LDL-C is 2.8 mmol/L (108 mg/dL). She is complaining of mild bilateral thigh aching for the past 4 weeks. CK is 280 U/L (normal <200 U/L — approximately 1.4× ULN). According to ESC/EAS 2019 guidelines, her LDL-C target is <55 mg/dL (1.4 mmol/L). What is the MOST appropriate next step?
A. Stop atorvastatin immediately — any CK elevation requires drug discontinuation to prevent rhabdomyolysis
B. Continue atorvastatin 80 mg unchanged — the CK elevation is less than 4× ULN and the symptoms are mild; continue and recheck CK in 4–6 weeks
C. Switch to rosuvastatin 40 mg and add ezetimibe 10 mg — she has not reached her LDL target and needs an alternative statin if tolerability is borderline
D. Add ezetimibe 10 mg to atorvastatin 80 mg without addressing the muscle symptoms first
Reveal Answer
Answer: B. Continue atorvastatin 80 mg unchanged — the CK elevation is less than 4× ULN and the symptoms are mild; continue and recheck CK in 4–6 weeks
CK elevation <4× ULN with mild muscle symptoms does not require statin discontinuation. The ESC 2019 guidance: if CK <4× ULN AND symptoms are mild and tolerable, continue the statin and recheck CK after 4–6 weeks. If symptoms worsen or CK rises above 4× ULN, then reduce dose or switch to a different statin. Stopping the statin abruptly in a very high-risk post-MI patient (LDL target <55 mg/dL) for mild, low-CK myalgia would leave her unprotected from statin's pleiotropic and LDL-lowering benefits — the risk of doing nothing far exceeds the risk of continuing at mild CK elevation. The LDL intensification question (adding ezetimibe, switching to rosuvastatin) is a separate decision that should be made after confirming tolerability.
Self-Assessment: Dyslipidaemia Management in Clinical Scenarios
The following clinical scenarios test your ability to interpret a lipid profile in context, select the appropriate drug and dose, recognise and manage adverse effects, and apply risk-stratified LDL-C targets. Work through each scenario independently before reading the analysis. The core competency being tested — IM2.18 — requires you to know not just which drug to use but the dose, the expected LDL reduction, the key adverse effects, and the monitoring parameters for each agent. The scenarios are designed to reflect the most common clinical situations encountered in Indian medicine wards and outpatient clinics.
Scenario A: Ramesh (from the opening hook) — a 48-year-old with 10-year ASCVD risk 18% (high risk), on atorvastatin 40 mg for 6 weeks, LDL-C 120 mg/dL (down from 158 mg/dL), with 3 weeks of bilateral thigh myalgia. CK is 180 U/L (0.9× ULN — normal). His LDL target is <70 mg/dL (high risk). What is your management plan?
Analysis: CK is normal (below ULN) — statin-associated myalgia without biochemical myositis. The myalgia is likely SAMS (statin-associated muscle symptom) but the absence of CK elevation makes the causal link less certain. Options: (1) Statin switch: switch from atorvastatin to rosuvastatin 20 mg (rosuvastatin is generally considered to have lower myopathy risk than atorvastatin at equivalent doses; pravastatin and fluvastatin are also options for patients with prominent SAMS — they are less lipophilic and potentially less muscle-penetrating). (2) Dose reduction: reduce atorvastatin to 20 mg to assess if myalgia resolves, with addition of ezetimibe 10 mg to maintain LDL-lowering intensity. (3) His current LDL at 120 mg/dL is still above target (<70 mg/dL); any regimen change should aim for intensification. A practical approach: switch to rosuvastatin 20 mg + add ezetimibe 10 mg (combined LDL reduction ~55–60% from baseline, likely to achieve target) — then recheck lipids and CK at 6 weeks.
Scenario B: A 30-year-old woman with no prior cardiac history presents for a routine medical examination. She has no symptoms. Fasting lipid profile: LDL-C 9.2 mmol/L (355 mg/dL), TG 1.4 mmol/L (normal), HDL 1.2 mmol/L. Physical examination: bilateral Achilles tendon xanthomata. Her father had an MI at age 38. TSH and renal function are normal. Formulate a diagnosis and outline the management plan.
Analysis: Clinical diagnosis: heterozygous familial hypercholesterolaemia (Dutch Lipid Clinic Network criteria: LDL-C >6.5 mmol/L at age <40 = 3 points; tendinous xanthomata = 6 points; first-degree relative with premature CVD = 1 point; total ≥8 = definite FH). Management: (1) High-intensity statin immediately — atorvastatin 80 mg or rosuvastatin 40 mg; target ≥50% LDL reduction (target LDL <2.6 mmol/L — 100 mg/dL — as minimum; very high-risk target <1.4 mmol/L after age 40 if established CVD). (2) Add ezetimibe 10 mg if LDL target not met on statin alone (expected; FH often requires combination therapy). (3) Genetic testing and cascade screening of first-degree relatives (parents, siblings — one or both parents likely have FH; cascade testing identifies other high-risk individuals before CVD develops). (4) Counsel on lifestyle modification (diet, exercise), but lifestyle alone will NOT achieve LDL target in FH — pharmacotherapy is mandatory. (5) Long-term follow-up: if LDL-C target not achieved with statin + ezetimibe, consider PCSK9 inhibitor (indication approved for FH regardless of prior CVD). Annual lipid profile, LFTs, CK monitoring.
Scenario C: A 60-year-old man with type 2 diabetes and hypertension presents with TG 12 mmol/L (1062 mg/dL) and epigastric pain for 12 hours. Serum amylase is 850 U/L (>3× ULN). His plasma appears cream-coloured ('lipaemic'). What is the complication, what is the immediate management, and what is the long-term drug treatment for his TG?
Analysis: Acute pancreatitis from severe hypertriglyceridaemia (TG >10 mmol/L is the threshold for TG-induced pancreatitis; TG >20 mmol/L is very high risk). Cream-coloured plasma = chylomicronaemia (Type IV or V hyperlipoproteinaemia). Immediate management: (1) Nil by mouth (fasting reduces chylomicron production); (2) IV fluid resuscitation (standard acute pancreatitis management); (3) Insulin infusion (even if euglycaemic — insulin activates LPL, rapidly clearing TG; target TG reduction to <500 mg/dL); (4) Heparin infusion (activates endothelial LPL, releases more LPL — debated; some centres use in severe cases). Long-term drug treatment: fenofibrate (145–200 mg daily) as first-line for TG reduction; optimise glycaemic control in diabetes (insulin resistance is driving TG); restrict dietary fat (<10–15% of calories) during acute episode; reduce alcohol; weight loss. Omega-3 (fish oil 3–4 g/day) can be added as adjunct. Target TG <500 mg/dL for pancreatitis prevention; ideally <150 mg/dL for cardiovascular risk.
SELF-CHECK
A 55-year-old man with type 2 diabetes, post-MI, and hypertension is on atorvastatin 40 mg + fenofibrate 145 mg + ezetimibe 10 mg. He develops severe muscle pain and his CK is reported as 4200 U/L (21× ULN). Which statement BEST describes the mechanism of this complication and the correct management?
A. Statin + ezetimibe combination always causes rhabdomyolysis — stop both and restart statin monotherapy after 4 weeks
B. CK elevation of 21× ULN meets the threshold for rhabdomyolysis (>40× ULN) — no action required unless renal function deteriorates
C. The combination of statin + fibrate increases myopathy risk; CK >10× ULN indicates myositis requiring statin discontinuation; check renal function and urine for myoglobinuria immediately
D. Ezetimibe is the most likely cause — stop ezetimibe and continue statin + fenofibrate
Reveal Answer
Answer: C. The combination of statin + fibrate increases myopathy risk; CK >10× ULN indicates myositis requiring statin discontinuation; check renal function and urine for myoglobinuria immediately
CK >10× ULN is myositis (severe myopathy) and requires immediate statin discontinuation. The threshold for rhabdomyolysis is CK >40× ULN plus myoglobinuria and AKI — this patient at 21× ULN may be progressing toward rhabdomyolysis. The combination of statin + fibrate significantly increases myopathy risk (fenofibrate is safer than gemfibrozil with statins, but the combination still carries higher myopathy risk than statin alone). Correct actions: (1) Stop statin immediately (and fenofibrate if it is a significant contributor); (2) Check serum creatinine and urinalysis (dipstick for haemoglobin — positive in the absence of RBCs indicates myoglobinuria); (3) IV fluid hydration if creatinine is rising (to prevent myoglobin-induced tubular injury); (4) Monitor CK until normalisation; (5) After CK normalises, restart a different statin at low dose with careful titration. Ezetimibe alone very rarely causes myopathy and is not the likely culprit here.
CLINICAL PEARL
The 'statin dose-response plateau' is one of the most important practical facts in lipid management: doubling the statin dose produces only an additional 6% LDL-C reduction (the '6% rule'). Therefore, when a patient is not achieving their LDL target on moderate-dose statin, the most efficient next step is to add ezetimibe (18–24% additional LDL reduction) rather than to double the statin dose (only 6% additional reduction with double the dose-dependent adverse effects). This makes statin + ezetimibe combination much more cost-effective and better tolerated than statin dose maximisation.
Second pearl: hypothyroidism is the most important secondary cause of elevated LDL-C to exclude before starting a patient on a statin. TSH should be checked at baseline in every patient with newly identified dyslipidaemia — hypothyroidism causes both LDL elevation (reduced LDLR expression) and increases statin myopathy risk (hypothyroid myopathy makes the muscle more vulnerable to statin-induced injury). Treating hypothyroidism first may normalise the LDL-C without any need for lipid-lowering pharmacotherapy.