Page 5 of 13
IM20.3-5 | Seizure Disorder Management and Safety — SDL Guide
Learning Objectives
- Describe the immediate first aid and acute management steps for a witnessed seizure
- Apply the stepwise status epilepticus management protocol with correct drug choices, doses, and timing thresholds (5–20–40–60 minutes)
- Select an appropriate first-line AED for a given seizure type and epilepsy syndrome, including recognition of contraindicated drug pairings
- Describe the clinically important drug interactions of antiepileptic medications, particularly with oral contraceptives and anticoagulants
- Counsel a patient with epilepsy on the six key safety domains: driving, occupation, swimming, sleep, alcohol, and medication adherence
- Apply special management considerations for women of childbearing age, the elderly, and patients with drug-resistant epilepsy
INSTRUCTIONS
This module covers the clinical management of seizure disorders — from the acute emergency of status epilepticus to long-term AED selection, drug interactions, and structured patient safety counselling. It pairs with the companion foundations module (IM20.1 and IM20.2) and requires application of seizure classification knowledge to treatment decisions. Pay particular attention to the time-stamped status epilepticus protocol and the AED contraindication rules — both are directly testable in clinical settings.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 418 — Seizures and Epilepsy (textbook)
- API Textbook of Medicine, 10th ed. — Neurology: Epilepsy Management (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed., Ch. 28 — Epilepsy Management (textbook)
- NICE Clinical Guideline CG137: Epilepsies — diagnosis and management (updated 2022) (guideline)
- Neurocritical Care Society Status Epilepticus Guideline 2012 (updated recommendations) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 11 PM in the emergency department. A 28-year-old woman with known epilepsy is brought in by ambulance — she has been convulsing continuously for 12 minutes. Her husband says she ran out of her levetiracetam four days ago and missed three doses. The paramedic has already given diazepam 10 mg IV en route, but the tonic-clonic movements persist. The registrar asks: what do you give next, how much, and how fast? In parallel, a different scenario: a 22-year-old man with newly diagnosed temporal lobe epilepsy asks your advice before returning to his construction job — can he drive? Can he work at heights? Can he go swimming alone? Can he continue his social drinking on weekends? These are not peripheral lifestyle questions; they are core safety counselling competencies that you will be expected to demonstrate, and errors — telling him it is safe to drive when it is not, or failing to warn him about alcohol — carry real medicolegal and safety consequences. This module gives you the clinical framework for both: the time-critical algorithm for managing an acute seizure and status epilepticus, and the structured approach to AED selection and patient safety counselling.
WHY THIS MATTERS
Management competency in seizure disorders operates on two time scales: the acute (minutes to hours) and the chronic (months to years). In the acute setting, delayed or incorrect treatment of status epilepticus causes preventable neuronal death and has a mortality of 10–20% — a figure that falls sharply with early, protocol-driven benzodiazepine administration. In the chronic setting, wrong AED selection (e.g., carbamazepine in juvenile myoclonic epilepsy), failure to counsel about driving restrictions, or failure to address sodium valproate teratogenicity in a woman of childbearing age all lead to patient harm. The NMC competencies for this module are IM20.3 (discuss epilepsy management including AEDs and drug interactions — KH level), IM20.4 (counsel patients and relatives about seizure safety — SH level, meaning you must be able to demonstrate the counselling), and IM20.5 (discuss acute management of a seizure episode — KH level). Together these span the full arc from emergency management to long-term outpatient care.
RECALL
Before proceeding, activate your knowledge from the companion module on seizure foundations. Recall: epilepsy requires ≥2 unprovoked seizures or one unprovoked seizure with ≥60% recurrence risk. AED selection is seizure-type specific — carbamazepine and phenytoin worsen myoclonic and absence seizures. The pathophysiology relevant to treatment: seizure generation involves an imbalance of GABA-mediated inhibition and glutamate-mediated excitation; most AEDs work by enhancing GABA (benzodiazepines, vigabatrin), blocking voltage-gated sodium channels (carbamazepine, phenytoin, lamotrigine, sodium valproate), blocking T-type calcium channels (ethosuximide), or inhibiting glutamate release (levetiracetam's SV2A mechanism). Status epilepticus arises when normal seizure-termination mechanisms fail — GABA-A receptors are internalised after ~5 minutes of continuous seizure activity, which progressively reduces the efficacy of benzodiazepines and is the pharmacological rationale for a time-sensitive, stepwise treatment protocol.
Acute Management of a Seizure Episode
The acute management of a seizure — whether a first-ever event or a breakthrough seizure in a known epileptic — begins with the same core priorities: protect the patient from injury, maintain airway patency, and determine whether the seizure is self-terminating or evolving into status epilepticus. This initial assessment must be completed within the first two minutes while simultaneously gathering the history and checking vital signs. The distinction between a brief, self-terminating seizure and one that will require pharmacological intervention is made at the five-minute mark — if the seizure has not terminated by five minutes, it meets the operational definition of status epilepticus and the stepwise treatment protocol must begin immediately.
For a witnessed, self-terminating tonic-clonic seizure in a known epileptic, immediate management consists of: place the patient in the lateral recovery (left lateral decubitus) position to protect the airway and reduce the risk of aspiration; clear the surrounding space of hard or sharp objects; do not restrain the convulsive movements; do not attempt to put anything in the mouth (this is dangerous and does not prevent tongue biting, which occurs at seizure onset before intervention is possible); loosen tight clothing around the neck; time the duration of the seizure from onset. An oxygen mask should be applied if available. Once the seizure terminates, assess airway, breathing, and circulation, and check capillary blood glucose immediately. Post-ictal examination includes a focused neurological assessment — any new focal deficit (Todd's palsy) or persistent altered consciousness beyond 20–30 minutes should prompt urgent neuroimaging. The patient should not be left alone until fully oriented.
In the community setting, bystander rescue medication can be prescribed for patients at high risk of prolonged seizures (known refractory epilepsy, seizures typically lasting >3–5 minutes). Rectal diazepam (5–10 mg, weight-adjusted, for adults and children) has been the traditional rescue medication; buccal midazolam (10 mg for adults) is now preferred in many settings for ease of administration, faster absorption, and lack of requirement for rectal access. Caregivers and family members should be trained in recognising seizure onset, timing the event, and administering rescue medication.
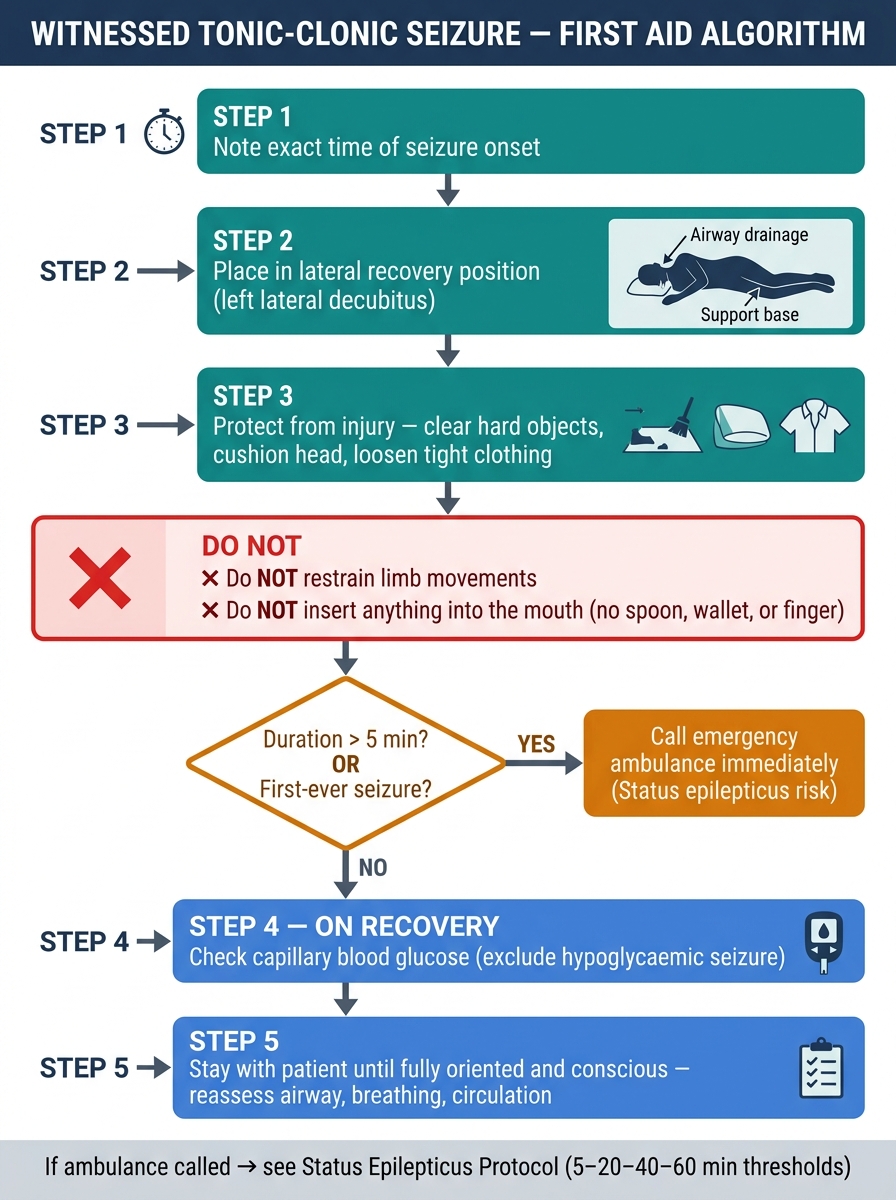
First Aid Algorithm for Witnessed Tonic-Clonic Seizure
Status Epilepticus — Stepwise Management
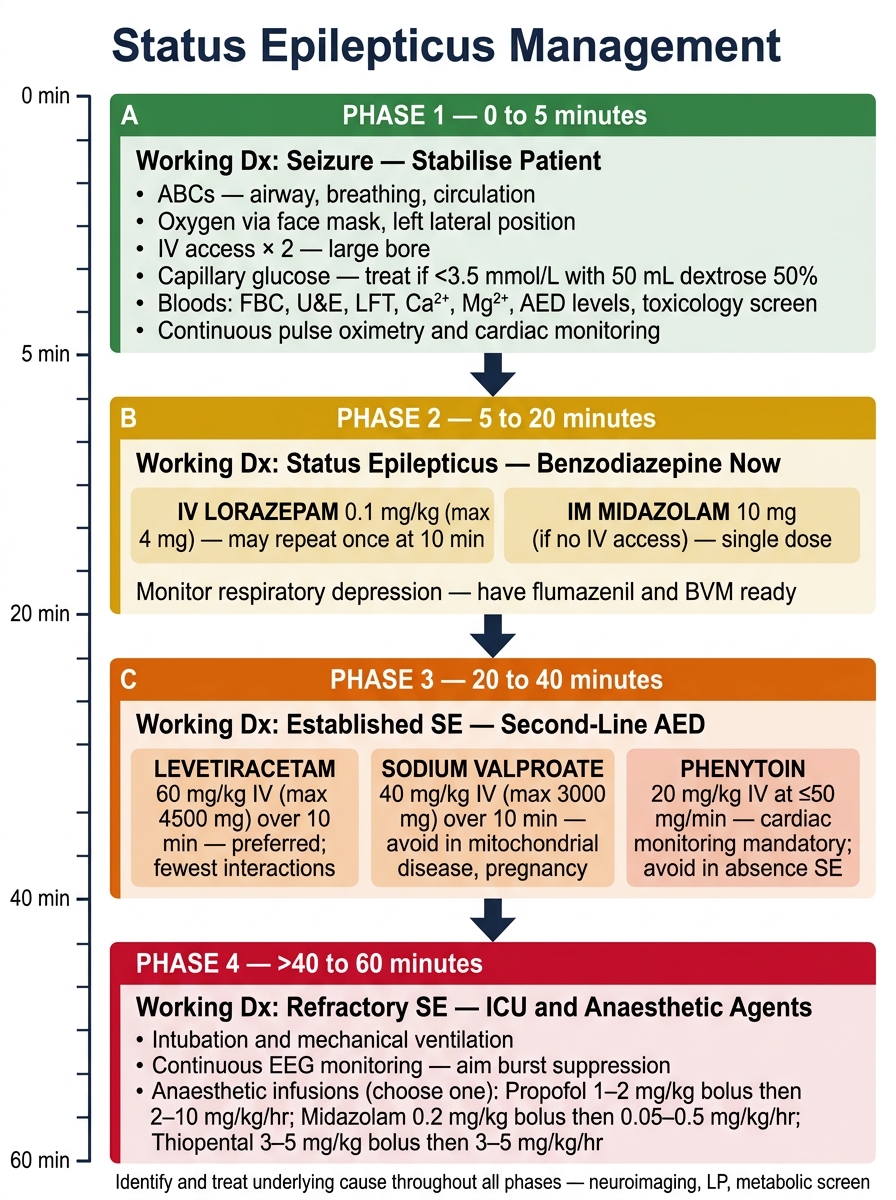
Status epilepticus (SE) is defined operationally as a seizure lasting ≥5 minutes, or two or more seizures without full recovery of consciousness between them. It is a neurological emergency with a mortality of 10–20% in convulsive SE and a risk of permanent neurological sequelae proportional to duration. Every minute of ongoing seizure activity causes progressive neuronal injury through glutamate excitotoxicity, mitochondrial failure, and hyperthermia. The management protocol is time-stamped — specific treatments are initiated at defined time points, not when the clinician feels ready. The mnemonic '5–20–40–60 minutes' captures the treatment escalation thresholds.
The stepwise management of convulsive status epilepticus proceeds as follows:
Phase 1 — Stabilisation (0–5 minutes): Simultaneously: secure airway (lateral position, suction, consider airway adjunct); high-flow oxygen 10–15 L/min; IV access (two large-bore peripheral cannulae) or IO access if IV fails; cardiac monitor and pulse oximetry; bedside capillary glucose — if hypoglycaemic, give thiamine 100 mg IV first then 50 mL of 50% dextrose (thiamine first prevents Wernicke's encephalopathy in the malnourished); blood tests (glucose, electrolytes, calcium, magnesium, FBC, LFT, ABG, AED levels, blood cultures if febrile, toxicology if overdose suspected). Do not delay treatment for investigations.
Phase 2 — Initial AED therapy (5–20 minutes): Benzodiazepine first-line.
- IV lorazepam 0.1 mg/kg (max 4 mg in adults) — preferred first-line IV benzodiazepine; slower offset than diazepam means less seizure recurrence. Give slowly over 2 minutes; can repeat once after 5 minutes if no response.
- If no IV access: IM midazolam 10 mg (adults) — at least as effective as IV lorazepam in RCTs and faster than IV access in prehospital settings.
- Alternatives: buccal midazolam 10 mg or rectal diazepam 10–20 mg if neither IV nor IM route available.
- Rationale for benzodiazepines: they enhance GABA-A receptor chloride conductance, hyperpolarising the neuron. They work rapidly (onset 1–2 min IV) and are effective while GABA-A receptors are still on the synapse — within the first 20 minutes of seizure onset.
Phase 3 — Second-line AED (20–40 minutes): IV AED loading — if benzodiazepine fails or seizure recurs.
Give ONE of the following (do not combine two sodium channel blockers):
- IV levetiracetam 60 mg/kg (max 4500 mg) over 15 minutes — preferred agent in many current guidelines (ESETT trial, ConSEPT trial) due to safety profile, no significant hepatic metabolism, no cardiac toxicity, and no drug interactions. Safe in liver disease.
- IV sodium valproate 40 mg/kg (max 3000 mg) over 15 minutes — highly effective, especially for generalised epilepsy; avoid in pregnancy and suspected metabolic hepatopathy.
- IV phenytoin 20 mg/kg (max 2000 mg) at ≤50 mg/min, cardiac monitoring mandatory (QT prolongation, hypotension, bradycardia, arrhythmia with rapid infusion) — or IV fosphenytoin 20 mg PE/kg (the prodrug, faster and safer IV infusion). Less preferred now due to cardiac toxicity risk.
- IV phenobarbital 20 mg/kg at 100 mg/min — equally effective, widely used where levetiracetam/valproate not available.
Phase 4 — Refractory status epilepticus (>40–60 minutes): Anaesthetic agents.
If seizures persist despite adequate dosing of a benzodiazepine and a second-line AED, the patient has refractory status epilepticus (RSE). This mandates: transfer to ICU, intubation and mechanical ventilation, and continuous EEG monitoring to detect non-convulsive SE (motor activity may cease but electrical status continues). Anaesthetic agent choices:
- Propofol infusion (1–2 mg/kg bolus then 2–10 mg/kg/hr) — rapid onset, easily titratable; risk of propofol infusion syndrome (lactic acidosis, cardiac failure) with prolonged high-dose use.
- Midazolam infusion (0.2 mg/kg bolus then 0.05–2 mg/kg/hr) — safe, widely available.
- Thiopental sodium (3–5 mg/kg bolus then 0.5–5 mg/kg/hr) — burst-suppression reliably achieved; prolonged coma with long context-sensitive half-life.
- Ketamine is emerging as an adjunct anaesthetic agent for RSE (NMDA antagonist, bronchodilatory, haemodynamically supportive).
Super-refractory SE (persisting >24 hours despite anaesthesia) requires consideration of immunotherapy (steroids, IVIG, plasma exchange for autoimmune encephalitis), ketogenic diet, hypothermia, and surgical intervention in selected cases.
Status Epilepticus Management Algorithm: Stepwise Drug Therapy by Time (0–60 min)
SELF-CHECK
A 35-year-old man is brought to the emergency department with a generalised tonic-clonic seizure that has lasted 8 minutes. IV access is obtained. His blood glucose is 95 mg/dL. He has no known epilepsy. What is the CORRECT first pharmacological treatment?
A. IV phenytoin 20 mg/kg over 20 minutes
B. IV lorazepam 0.1 mg/kg (max 4 mg) over 2 minutes
C. IV sodium valproate 40 mg/kg over 15 minutes
D. IM midazolam 10 mg immediately, then IV access
Reveal Answer
Answer: B. IV lorazepam 0.1 mg/kg (max 4 mg) over 2 minutes
A seizure lasting ≥5 minutes meets the definition of status epilepticus and requires immediate treatment. With IV access secured, the first-line agent is IV lorazepam 0.1 mg/kg (max 4 mg), given slowly over 2 minutes. Lorazepam is preferred over IV diazepam for first-line use because its slower redistribution from the brain means less seizure recurrence. IV phenytoin and sodium valproate are second-line agents used when benzodiazepines fail. IM midazolam is the correct choice only when IV access is unavailable — IV access is already obtained in this case, so IM midazolam is not the optimal route. Glucose is already normal so dextrose is not indicated.
Antiepileptic Drug Selection — Principles and First-Line Choices
The decision to start a long-term antiepileptic drug (AED) is made after confirming the diagnosis of epilepsy (ILAE 2014 criteria) and identifying the seizure type and epilepsy syndrome. A first unprovoked seizure without a high-risk structural lesion carries approximately a 40–50% recurrence risk over 2 years — which is generally below the threshold for initiating AED therapy unless there are specific risk factors (structural lesion, epileptiform EEG, family history, nocturnal seizure). Once the decision to treat is made, the drug chosen must be matched to the seizure type and syndrome — this is the most important principle in AED prescribing, and failure to apply it causes harm.
The overarching principle is that no AED is universally safe for all seizure types. Three broad categories guide initial drug selection:
Category 1 — Focal epilepsies (including focal to bilateral tonic-clonic):
- Carbamazepine (sodium channel blocker): first-line for focal seizures; highly effective; risk of hyponatraemia (SIADH), diplopia, ataxia at higher doses; induces hepatic CYP3A4 enzymes (interacts with warfarin, oral contraceptives, other AEDs). Begin at 100–200 mg twice daily, titrate slowly.
- Levetiracetam (SV2A synaptic vesicle protein modulator): increasingly used as first-line for focal and generalised epilepsies; excellent safety profile, no hepatic metabolism, no drug interactions via CYP system; side-effects include irritability and mood change (less frequent with extended-release formulations). 500 mg twice daily, titrate up to 1500–3000 mg/day.
- Lamotrigine (sodium channel blocker): effective for focal and generalised seizures including absence; requires very slow titration (risk of Stevens-Johnson syndrome / toxic epidermal necrolysis if escalated rapidly, especially when combined with valproate); preferred in women of childbearing age for its comparatively favourable teratogenicity profile. Start at 25 mg/day when used alone.
- Oxcarbazepine: prodrug-like relative of carbamazepine; fewer drug interactions; similar efficacy for focal seizures; risk of hyponatraemia more pronounced.
Category 2 — Generalised epilepsies (including JME, childhood absence, tonic-clonic of generalised onset):
- Sodium valproate (multiple mechanisms: sodium channel, GABA enhancement, T-Ca channel): the broadest-spectrum AED, effective across all generalised seizure types and as a second-line agent for focal seizures. However, it carries the highest teratogenicity risk of any commonly used AED — associated with neural tube defects (4–5 times baseline risk), autism spectrum disorder, and reduced cognitive development in children exposed in utero. The NICE 2022 guidance and EU regulatory restrictions explicitly state that sodium valproate must NOT be prescribed to girls and women of childbearing potential unless a pregnancy prevention programme is in place and the patient is counselled that she cannot become pregnant. This is a hard clinical rule for the IM20.4 counselling competency.
- Ethosuximide (T-type Ca²⁺ channel blocker): first-line for typical absence seizures only; ineffective against tonic-clonic seizures; hence preferred when the only seizure type is absence without GTCS.
- Levetiracetam: effective for JME and other generalised epilepsies; preferred alternative to valproate in women.
- Lamotrigine: effective for absence and GTCS in generalised epilepsy; less effective for myoclonic seizures (may worsen myoclonus in some JME patients at high doses — use with caution).
- AVOID in ALL generalised epilepsies with absence or myoclonic components: carbamazepine, oxcarbazepine, phenytoin, pregabalin, gabapentin, tiagabine, vigabatrin — all of these can worsen or precipitate absence and myoclonic seizures.
Category 3 — Special considerations:
- Women of childbearing age: prefer levetiracetam or lamotrigine over valproate; prescribe folic acid 5 mg/day (higher dose than the 400 mcg standard) before conception and through the first trimester for any woman on AEDs who may become pregnant; never stop AEDs suddenly in pregnancy (sudden discontinuation causes maternal seizures which are themselves teratogenic).
- Elderly (new-onset post-stroke epilepsy): lamotrigine and levetiracetam preferred (minimal drug interactions, no cardiac toxicity); carbamazepine tolerated but risks hyponatraemia.
- Hepatic disease: levetiracetam (renally cleared) is preferred; avoid valproate (hepatotoxic), carbamazepine, and phenytoin (hepatically metabolised).
- Renal disease: adjust renally cleared drugs — levetiracetam and gabapentin require dose reduction with declining eGFR.
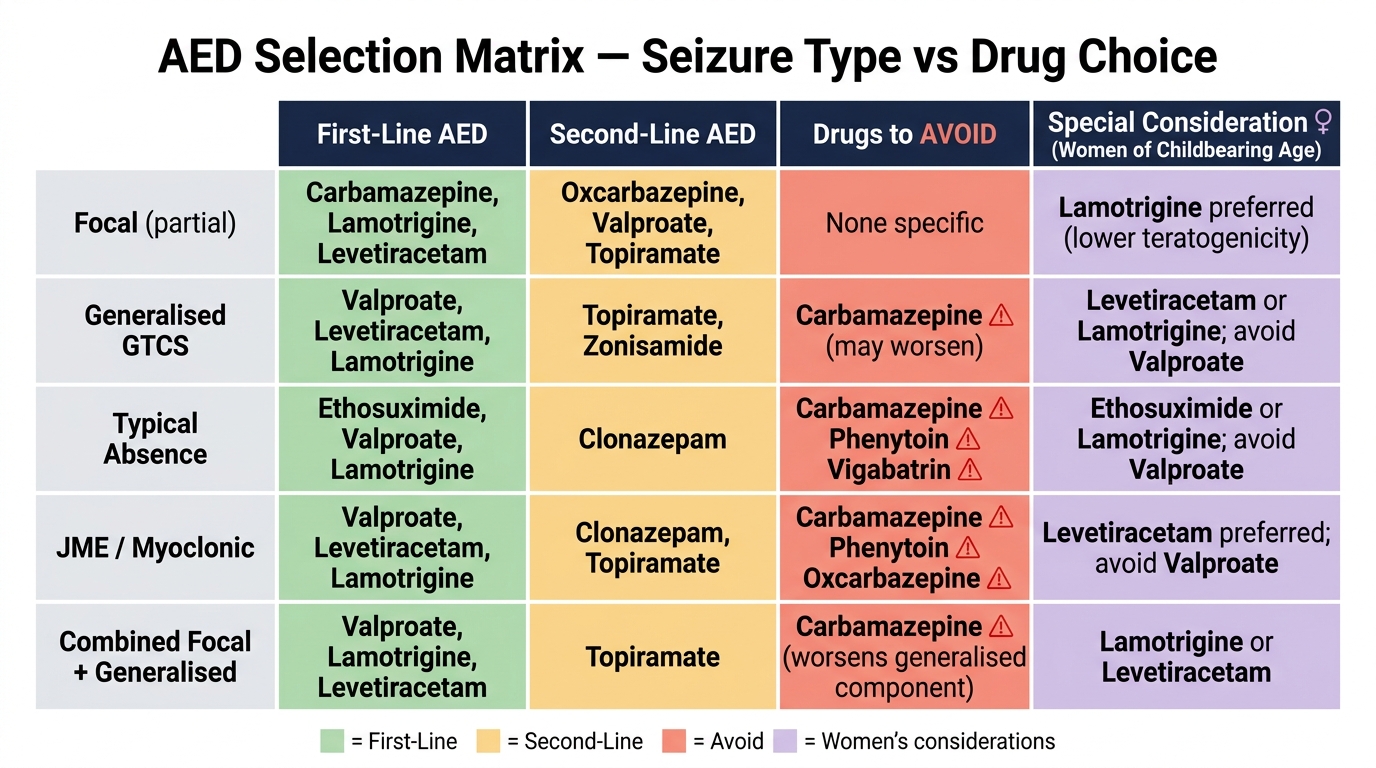
AED Selection Matrix by Seizure Type / Syndrome