Page 6 of 13
IM20.3-5 | Seizure Disorder Management and Safety — SDL Guide (Part 2)
Drug Interactions and Monitoring
Antiepileptic drugs are among the most pharmacokinetically complex medications in clinical practice, largely because many older AEDs are potent inducers or inhibitors of the cytochrome P450 enzyme system and because most AEDs have narrow therapeutic indices. Understanding the principal interaction patterns is essential not only for managing poly-pharmacy in refractory epilepsy but also for managing the common and clinically important interactions with non-AED medications — particularly oral contraceptives, anticoagulants, and antimicrobials.
Provided image
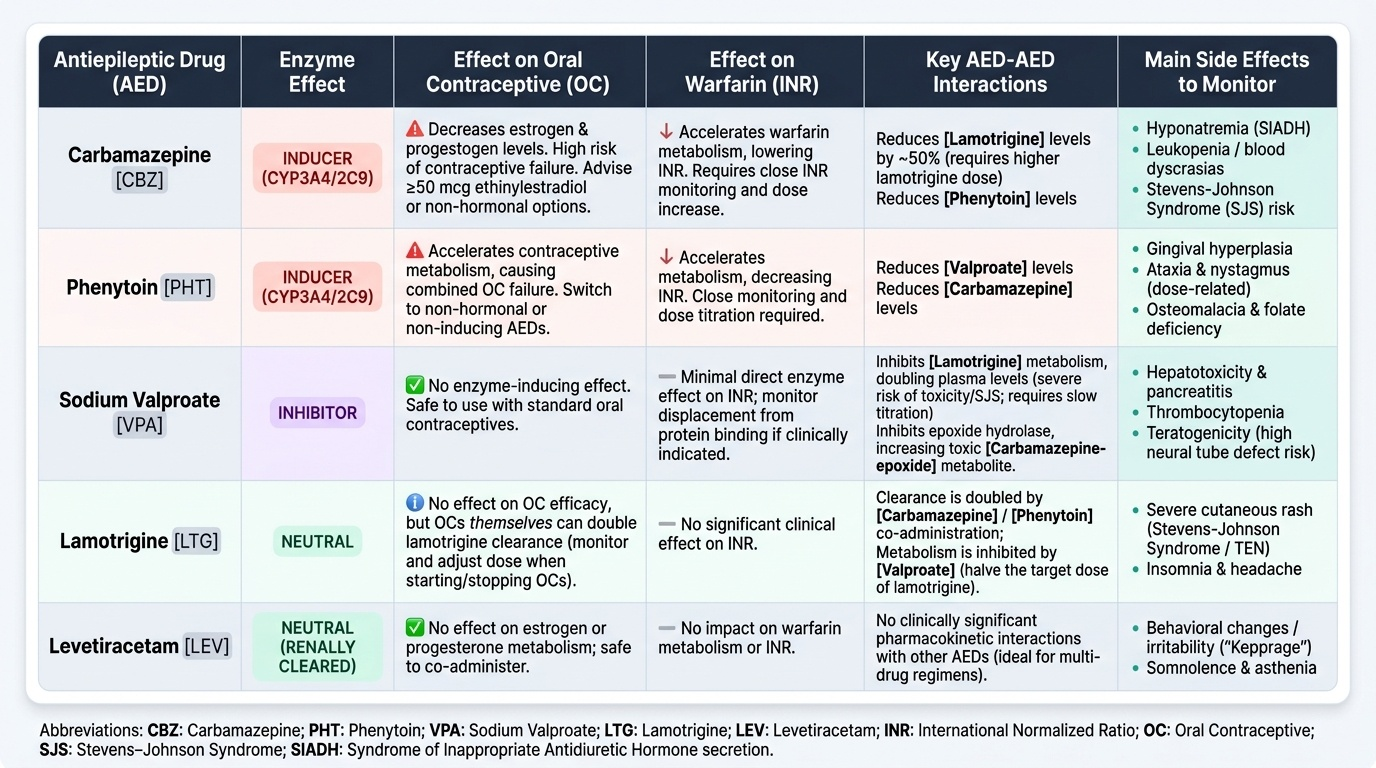
The three most important pharmacokinetic drug interaction mechanisms in epilepsy practice are enzyme induction, enzyme inhibition, and pharmacodynamic synergy or antagonism.
Enzyme-inducing AEDs (EI-AEDs): The classic EI-AEDs are carbamazepine, phenytoin, phenobarbital, and oxcarbazepine (partial inducer). These drugs upregulate hepatic CYP3A4 and CYP2C9, thereby accelerating the metabolism of co-administered drugs and reducing their plasma levels. The clinically critical interactions are:
- Oral contraceptives (OCs): EI-AEDs reduce plasma oestrogen and progestogen concentrations, causing combined OC failure — this is a major and frequently unrecognised cause of unintended pregnancy in women with epilepsy. Women of childbearing age on EI-AEDs who wish to use OCs must be advised to use higher-dose oestrogen pills (≥50 mcg ethinylestradiol), or better, to switch to a non-enzyme-inducing AED (lamotrigine, levetiracetam) or use a non-hormonal contraceptive (copper IUD, condoms).
- Warfarin: EI-AEDs reduce INR by accelerating warfarin metabolism; starting or stopping an EI-AED requires close INR monitoring and dose adjustment.
- AED-AED interactions: carbamazepine reduces plasma levels of lamotrigine by ~50% (requiring higher lamotrigine doses); phenytoin reduces valproate and carbamazepine levels; valproate inhibits lamotrigine metabolism (increases lamotrigine levels — risk of toxicity and Stevens-Johnson syndrome, requiring much slower lamotrigine titration).
Enzyme-inhibiting AEDs: Sodium valproate is the most clinically significant enzyme inhibitor in epilepsy practice. It inhibits the metabolism of lamotrigine (double the plasma level) and phenobarbital, and inhibits the epoxide hydrolase enzyme that metabolises carbamazepine epoxide (the toxic metabolite of carbamazepine) — potentially causing carbamazepine toxicity at standard doses.
Phenytoin — unique pharmacokinetics: Phenytoin exhibits zero-order (saturable) kinetics at clinical concentrations — meaning that small increases in dose produce disproportionately large increases in plasma level once the enzymatic elimination pathway is saturated. This makes phenytoin toxicity unpredictable and over-shooting common. Signs of phenytoin toxicity: nystagmus (earliest sign, occurs at levels >20 mg/L), ataxia (>30 mg/L), dysarthria, and encephalopathy (>40 mg/L). Routine therapeutic drug monitoring (target range: 10–20 mg/L) is mandatory with phenytoin.
Routine monitoring during AED therapy:
- All AEDs: LFT, FBC, and electrolytes at baseline and after dose changes (carbamazepine → hyponatraemia; valproate → thrombocytopaenia, hyperammonaemia).
- Phenytoin: serum levels, FBC (macrocytosis from folate impairment), gum examination (gingival hyperplasia), bone density (long-term — CYP-induced vitamin D catabolism).
- Valproate: LFT (hepatotoxicity risk, especially in children under 2 years), ammonia level if confusion (valproate-induced hyperammonaemia without liver failure is a distinct entity), weight (valproate causes weight gain), polycystic ovary morphology on pelvic ultrasound if menstrual irregularity develops.
- Carbamazepine: serum sodium (SIADH), CBC, serum levels if toxicity suspected.
- Lamotrigine: rash surveillance — early truncal macular rash within the first 8 weeks mandates immediate drug cessation (risk of SJS progression).
SELF-CHECK
A 25-year-old woman with focal epilepsy has been on carbamazepine 400 mg twice daily for 2 years with good seizure control. She now wishes to start the combined oral contraceptive pill for contraception. What is the MOST important advice to give her?
A. The combined OCP is safe at standard doses; no interaction with carbamazepine
B. Carbamazepine is a hepatic enzyme inducer and significantly reduces oestrogen levels, causing potential contraceptive failure — switch to a non-inducing AED or use non-hormonal contraception
C. Switch to sodium valproate as it does not interact with the OCP
D. Use the progesterone-only pill, which is not affected by enzyme inducers
Reveal Answer
Answer: B. Carbamazepine is a hepatic enzyme inducer and significantly reduces oestrogen levels, causing potential contraceptive failure — switch to a non-inducing AED or use non-hormonal contraception
Carbamazepine is a potent hepatic enzyme inducer (CYP3A4) that reduces the plasma concentration of both oestrogen and progestogen in combined oral contraceptives, risking contraceptive failure and unintended pregnancy. This interaction is clinically well-established. The safest options are: (1) switch carbamazepine to a non-enzyme-inducing AED (lamotrigine or levetiracetam) if seizure control allows, or (2) use non-hormonal contraception (copper IUD, barrier methods). Sodium valproate does not induce enzymes and does not impair OCP efficacy — however, valproate has significant teratogenicity risks and is not an appropriate switch for a woman who may become pregnant. The progesterone-only pill (mini-pill) is ALSO rendered less effective by enzyme inducers — it is NOT a safe alternative with carbamazepine.
Patient Safety Counselling — Driving, Occupation, and Lifestyle
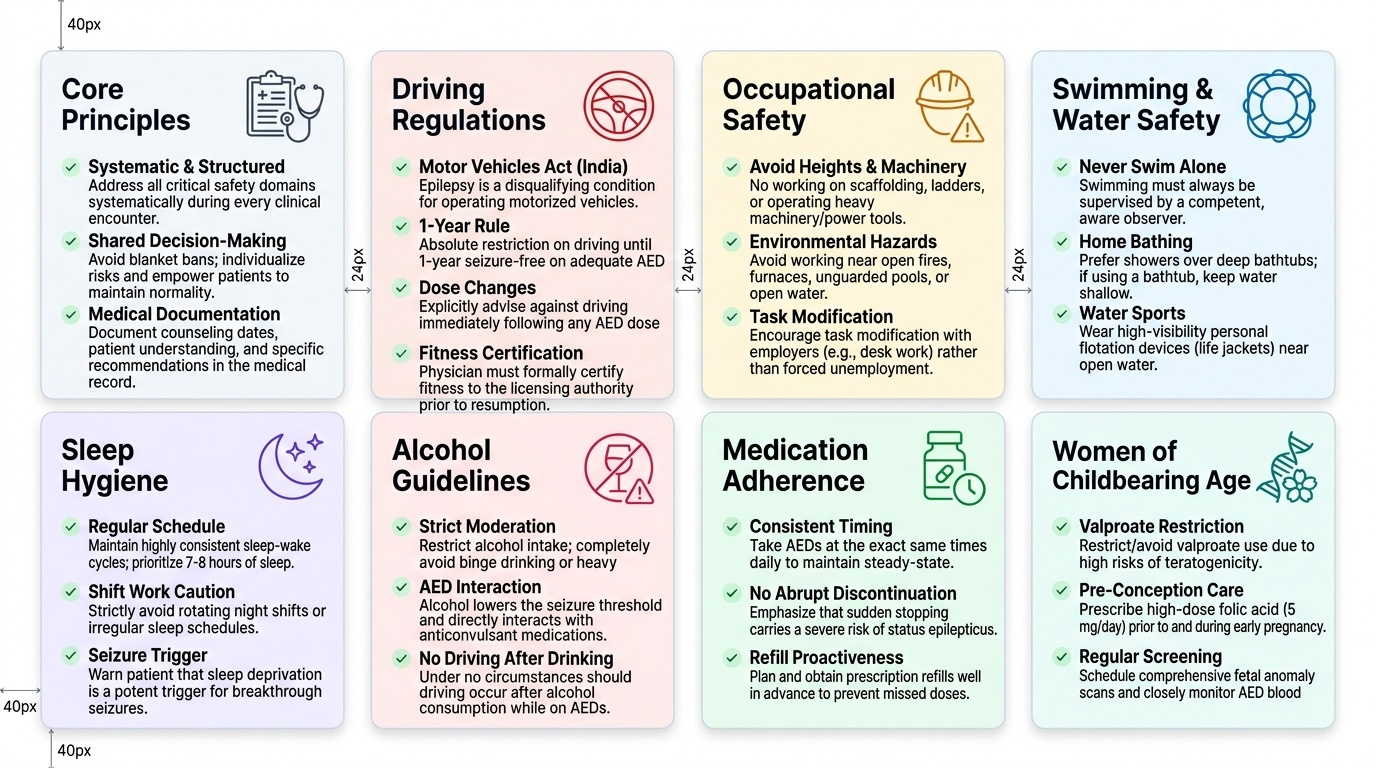
Safety counselling for patients with epilepsy is a core clinical skill (NMC IM20.4, SH level — you must be able to demonstrate the counselling). The aim is to empower the patient to lead as normal a life as possible while managing the real risks posed by unpredictable seizure activity. Effective counselling is structured, covers all domains, avoids excessive restriction, and uses shared decision-making. It must be documented in the medical record. The following domains must be addressed systematically with every patient who has active seizure disorder.
Provided image
Driving regulations (India and general principles):
Under the Motor Vehicles Act 1988 (India), epilepsy is a disqualifying condition for driving a motor vehicle. A patient with a diagnosis of epilepsy — including a single unprovoked seizure with high recurrence risk — must not drive until they have been seizure-free for a minimum of one year on adequate AED therapy, and only if their physician certifies fitness to drive to the licensing authority. In practice: patients must be explicitly told not to drive until seizure-free for one year; this applies to cars, motorcycles, and commercial vehicles (commercial licences require longer seizure-free periods). They should also be advised not to drive after any dose change that might affect seizure control. Document the counselling and the date in the medical record.
Occupational safety:
Patients with active epilepsy should avoid occupations and tasks that carry risk of serious injury or harm to others in the event of a seizure: working at heights (scaffolding, rooftops, ladders), operating heavy machinery or power tools without guard rails, driving professional vehicles (buses, trucks, taxis), working near open water or unguarded pools, working near open fires or furnaces. The assessment is not blanket — a desk-based software engineer has virtually no occupational seizure risk, while a construction worker at heights has a life-threatening risk from the same seizure. Occupational counselling should be individualised and, where uncertainty exists, documented advice to modify tasks (rather than leave employment). The patient should inform their employer of the diagnosis in safety-critical roles, and the physician should be available to provide a medical letter if required.
Water and swimming safety:
Drowning is a leading cause of accidental death in people with epilepsy — the risk is 15–20 times higher than in the general population. Patients must never swim alone. When swimming with others, a companion must be aware of the epilepsy diagnosis and able to assist in an emergency. Baths should be kept shallow or the patient should shower rather than bathe; bathroom doors should not be locked. Hot tubs and jacuzzis should be avoided due to the additional hyperthermia seizure trigger.
Sleep hygiene:
Sleep deprivation is a potent and near-universal seizure trigger. Patients must be counselled to maintain regular sleep and wake times, avoid all-night studying or shift work that severely disrupts sleep, and be aware that shift work is a specific risk factor for breakthrough seizures. Social situations that lead to late nights (parties, festive events) should be navigated with advance planning — patients can take their AED dose close to their normal time even if the social event continues.
Alcohol:
Alcohol lowers the seizure threshold directly and, more importantly, causes sleep disruption after drinking that lowers the threshold the next morning — this is why most JME seizures occur the morning after parties. Patients should be told: (1) avoid heavy or binge drinking entirely; (2) moderate consumption (1–2 units for women, 2–3 units for men on any occasion) is acceptable for most patients if AED adherence is maintained; (3) never drive after any alcohol consumption if on AEDs (combined sedation); (4) alcohol withdrawal after habitual heavy drinking is a major seizure trigger and patients should seek medical supervision if attempting to stop.
Medication adherence:
Most breakthrough seizures in known epileptics are caused by missed doses. Counsel patients: take AEDs at the same time each day; use a pill organiser; do not stop AEDs abruptly — sudden withdrawal can precipitate status epilepticus even in well-controlled epilepsy. When stopping AED therapy after a prolonged seizure-free period, dose must be tapered over weeks to months under medical supervision.
Women of childbearing age — special safety counselling:
As detailed in the AED section: sodium valproate must not be used in women of childbearing potential without a pregnancy prevention programme. All women on AEDs who wish to become pregnant should seek pre-conception counselling. Key messages: (1) continue the AED — uncontrolled seizures during pregnancy are more dangerous than the AED; (2) switch to the safest AED for the seizure type BEFORE conception, not after discovering pregnancy; (3) prescribe high-dose folic acid 5 mg/day from at least 3 months before conception; (4) detailed anomaly scan at 18–20 weeks; (5) breastfeeding is generally safe with most AEDs (levetiracetam and lamotrigine pass into breast milk but at low levels; valproate passes in very low concentrations).
First aid training for family members:
Family members and caregivers should receive training in seizure first aid: lateral recovery position, do not restrain, do not insert objects in mouth, time the seizure, call ambulance if >5 minutes or first-ever seizure, administer rescue medication (buccal midazolam or rectal diazepam) if prescribed.
SELF-CHECK
A 19-year-old woman with juvenile myoclonic epilepsy is started on sodium valproate for the first time. She is currently not sexually active but plans to marry in two years. Which of the following statements about sodium valproate counselling is CORRECT?
A. Sodium valproate is safe in pregnancy and does not require special counselling
B. She should be advised about sodium valproate teratogenicity now, a pregnancy prevention programme should be documented, and alternative AEDs such as levetiracetam should be discussed
C. Sodium valproate teratogenicity counselling is only required when she becomes pregnant or announces she wants to conceive
D. She can be reassured that the risks of valproate are similar to lamotrigine in pregnancy
Reveal Answer
Answer: B. She should be advised about sodium valproate teratogenicity now, a pregnancy prevention programme should be documented, and alternative AEDs such as levetiracetam should be discussed
Sodium valproate carries the highest teratogenicity risk of commonly used AEDs: 4–5× increased risk of neural tube defects, increased risk of autism spectrum disorder, and reduced cognitive development in children exposed in utero. Under NICE 2022 guidance and EU regulatory requirements, all girls and women of childbearing potential on valproate must be enrolled in a Pregnancy Prevention Programme (PPP) from the time of prescription — not only when they express a wish to conceive. This means: documented counselling about the risks, confirmed understanding, and either use of effective contraception or a confirmed plan for discussion before conception. Delaying this counselling until she is pregnant risks harm. While levetiracetam is a better alternative for JME in women, if valproate is used the PPP is mandatory from day one. Valproate's teratogenicity is substantially worse than lamotrigine's.
Long-Term Management and Special Populations
The long-term management of epilepsy extends well beyond AED prescribing to include monitoring for drug efficacy and tolerability, adjustment for life circumstances, planning around specific high-risk periods, and determining when (and if) AED therapy can eventually be withdrawn. A structured long-term management approach reduces breakthrough seizures, prevents drug-related complications, and addresses the psychological and social dimensions of a chronic neurological condition that often affects young patients at formative life stages.
Monitoring therapy and defining treatment failure:
The goal of AED therapy is complete seizure freedom with no adverse effects — achievable in approximately 70% of patients. The working definition of drug-resistant epilepsy (also termed refractory epilepsy) is failure of adequate trials of two tolerated, appropriately chosen AEDs (whether as monotherapy or in combination) to achieve sustained seizure freedom. This threshold — two drug failures — is clinically important because it identifies the patient who should be referred to a specialised epilepsy centre for evaluation for resective surgery, vagus nerve stimulation, responsive neurostimulation, or ketogenic diet. Epilepsy surgery is underutilised — temporal lobectomy for mesial temporal sclerosis achieves seizure freedom in 60–70% of patients; surgically remediable focal cortical dysplasia is another well-established indication. The referral to a tertiary epilepsy service should happen after the second drug failure, not after the fifth or sixth.
Pregnancy and epilepsy:
Pregnancy does not predictably worsen seizure control — approximately one-third of women have more seizures, one-third have fewer, and one-third are unchanged. The major risks to the pregnancy arise from: (1) AED teratogenicity (addressed in drug selection — avoid valproate; use high-dose folate); (2) maternal seizures, particularly GTCS, which cause foetal hypoxia, placental abruption, and trauma risk; and (3) pharmacokinetic changes in pregnancy (increased renal clearance and volume of distribution reduce AED plasma levels — levetiracetam and lamotrigine levels fall significantly in pregnancy, requiring dose escalation and therapeutic drug monitoring in the second and third trimesters). Obstetric input with a specialist midwife and neurologist is essential throughout pregnancy. Vitamin K is recommended for the neonate exposed to enzyme-inducing AEDs (reduces the risk of neonatal haemorrhagic disease by preventing drug-induced vitamin K deficiency).
Elderly patients:
New-onset epilepsy over age 60 is most commonly post-stroke epilepsy (structural, focal onset). Preferred AEDs: lamotrigine and levetiracetam (favourable drug interaction profiles, no cardiac toxicity, well tolerated). Phenytoin should be avoided in the elderly: its zero-order kinetics make toxicity unpredictable, and it has significant interactions with the polypharmacy typical of this age group. Falls risk from all AEDs (especially carbamazepine and phenytoin causing ataxia and dizziness) must be explicitly addressed. Bone density monitoring is important — long-term enzyme-inducing AEDs cause secondary osteoporosis via accelerated vitamin D catabolism; calcium and vitamin D supplementation should accompany therapy.
Children — key considerations:
Many childhood epilepsy syndromes are self-limiting (childhood absence epilepsy remits in ~70% by adolescence). AED therapy in children must be weight-based. Sodium valproate is highly effective for generalised epilepsies in children but should be used only when no safer alternative exists, given its cognitive and developmental effects; it is absolutely avoided in girls once they reach puberty without a pregnancy prevention programme in place. Dravet syndrome (SCN1A mutation — loss of function in Nav1.1 inhibitory interneuron channels) is refractory to phenytoin, carbamazepine, and lamotrigine (which actually worsen it); it responds to valproate, stiripentol, clobazam, and fenfluramine. Lennox-Gastaut syndrome (multiple seizure types, slow spike-and-wave, cognitive impairment) is treated with valproate, clobazam, lamotrigine, rufinamide, and VNS.
AED withdrawal:
Withdrawal of AED therapy after a prolonged seizure-free period is appropriate in some patients but must be carefully planned. Factors favouring successful withdrawal: epilepsy syndrome known to have a natural remission (CAE), seizure-free for ≥2 years, normal MRI and EEG, and single seizure type. Factors against withdrawal: JME (85–90% relapse), focal epilepsy with structural substrate, previous status epilepticus, abnormal MRI. Withdrawal must always be gradual (over weeks to months) to avoid precipitating seizures or status epilepticus. The patient must be counselled that relapse is possible and driving restrictions apply during the withdrawal period.
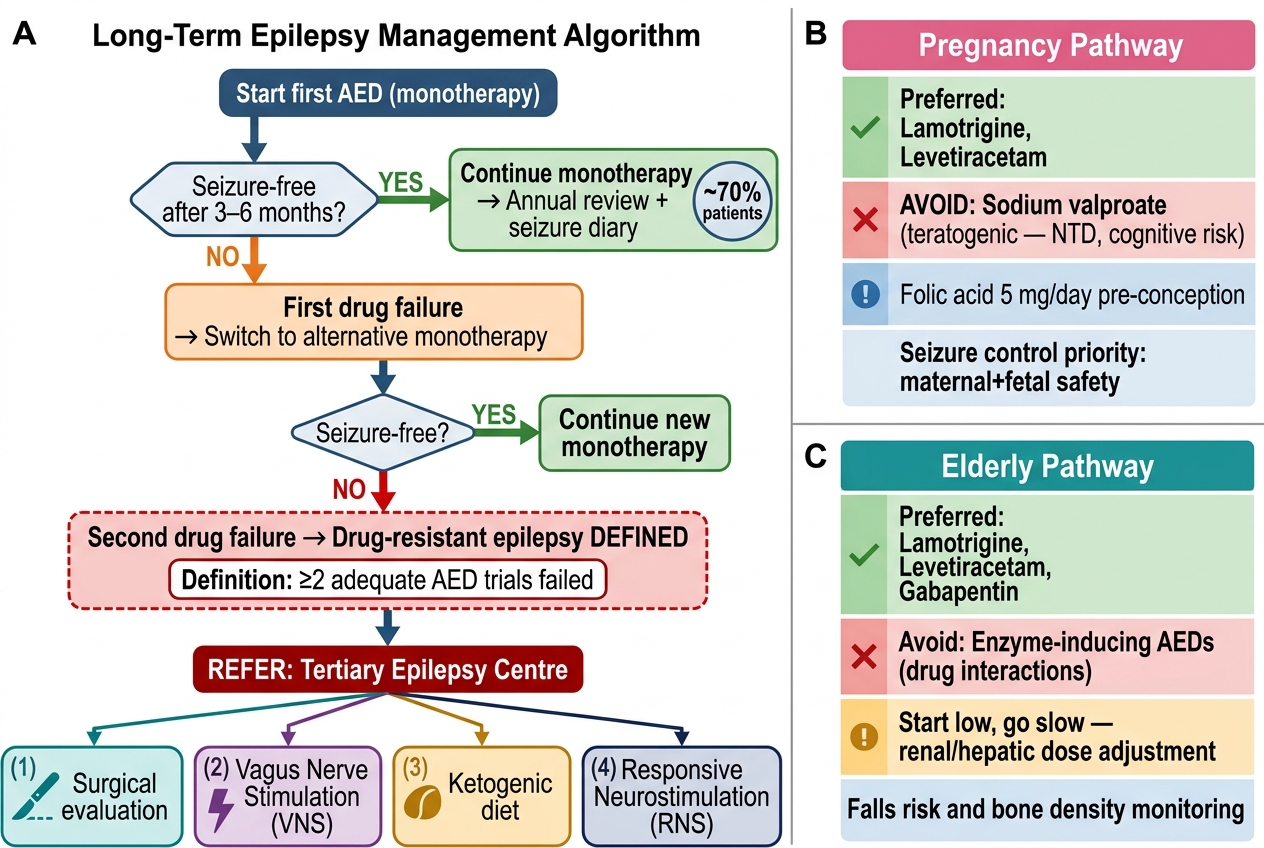
Epilepsy Long-Term Management Algorithm with Special Population Pathways
SELF-CHECK
A 32-year-old man with mesial temporal lobe epilepsy due to hippocampal sclerosis has failed adequate trials of carbamazepine (at therapeutic levels, well tolerated) and then levetiracetam (adequate dose, good adherence) — both discontinued due to lack of seizure control. He continues to have monthly focal impaired awareness seizures. What is the MOST appropriate next step in his management?
A. Add a third AED (combination polytherapy) as monotherapy has clearly failed
B. Switch to sodium valproate as the third monotherapy trial
C. Refer to a tertiary epilepsy centre for surgical evaluation
D. Reassure him that seizure control improves over time with dose adjustment
Reveal Answer
Answer: C. Refer to a tertiary epilepsy centre for surgical evaluation
This patient has drug-resistant epilepsy by the standard definition: failure of two adequately dosed, appropriately chosen AEDs. At this threshold, referral to a tertiary epilepsy centre for surgical evaluation is the correct next step — not a third drug trial. Mesial temporal sclerosis is the most surgically remediable form of epilepsy; anterior temporal lobectomy achieves seizure freedom in 60–70% of selected patients. Waiting for a third or fourth drug failure before referring is a common and harmful delay. A third AED has approximately a <5% chance of achieving seizure freedom in drug-resistant temporal lobe epilepsy, whereas surgery has a much higher probability. Valproate would be ineffective in focal epilepsy. Further reassurance without action is not appropriate.