Page 13 of 32
IM25.10-11 | Geriatric COPD and Surgical Care — SDL Guide
Learning Objectives
- Describe the pathophysiology of COPD including the distinct mechanisms of emphysema and chronic bronchitis, and identify Indian-specific risk factors
- Apply the GOLD spirometric staging and ABE classification to determine appropriate stable COPD pharmacological management
- Manage an acute COPD exacerbation including controlled oxygen, bronchodilators, corticosteroids, antibiotics, and NIV for type 2 respiratory failure
- Conduct a pre-operative risk assessment for an elderly patient using ASA classification, RCRI, frailty scale, and spirometry
- Describe perioperative medication management for elderly patients on corticosteroids, anticoagulants, and antiplatelets
- Outline post-operative prevention priorities: delirium (HELP bundle), respiratory complications, VTE, and pain management in the elderly surgical patient
INSTRUCTIONS
COPD is among the most prevalent chronic diseases in elderly Indians, and surgery is a frequent intervention in this age group. This module covers both: the GOLD-based management of stable COPD and exacerbations, and the systematic perioperative risk assessment and optimisation framework for elderly surgical patients. The integration of both topics reflects the clinical reality that many elderly patients with COPD will need surgery.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 289 — Chronic Obstructive Pulmonary Disease (textbook)
- API Textbook of Medicine, 11th ed., Chapter on COPD and Geriatric Surgical Care (textbook)
- GOLD 2023 Global Strategy for the Diagnosis, Management and Prevention of COPD (guideline)
- AHA/ACC 2014 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Subramaniam is 76 years old, a retired factory supervisor and former smoker (40 pack-years, stopped at 65). He presents to the emergency with his third exacerbation in eight months — each time requiring hospitalisation. He is breathless at rest, SpO₂ 84% on air, using accessory muscles to breathe. His chest X-ray shows hyperinflation and a flattened diaphragm. Spirometry from his last outpatient visit shows FEV₁ 31% predicted, FEV₁/FVC ratio 0.52. Two weeks later, he requires emergency laparotomy for a perforated viscus. The anaesthetist identifies him as 'high risk' — not because of his age alone, but because he has severe COPD with reduced respiratory reserve, is nutritionally depleted, and his post-operative pulmonary complication risk is very high. These two challenges — managing advanced COPD in the elderly and managing the elderly patient through major surgery — illustrate the distinctive demands of geriatric medicine: disease that has progressed for decades meeting the acute physiological stress of surgery, in a body with limited reserve to compensate.
WHY THIS MATTERS
COPD is the third leading cause of death globally and one of the most prevalent chronic respiratory diseases in elderly Indians, with an estimated 14% prevalence in adults over 60. The combination of lifetime tobacco exposure, occupational dust, indoor air pollution (biomass burning — a major Indian-specific risk factor), and age-related lung function decline creates a large population of elderly patients with advanced COPD, frequent exacerbations, and high hospital mortality. Simultaneously, the elderly undergo a disproportionate share of major surgical procedures — approximately 30% of all surgeries are performed on patients over 65 — and the risk of post-operative morbidity and mortality is substantially amplified by COPD, frailty, polypharmacy, and cognitive impairment. NMC competencies IM25.10 and IM25.11 require KH-level competency in both areas.
RECALL
Activate your respiratory physiology. Forced expiratory volume in 1 second (FEV₁) is the volume of air expelled in the first second of a forced exhalation; the most important spirometric measure of airway obstruction. FVC (forced vital capacity) is the total volume expelled in a forced exhalation. FEV₁/FVC ratio < 0.70 (post-bronchodilator) confirms airflow limitation — the spirometric definition of COPD. Residual volume (RV) is the volume remaining after maximal exhalation — elevated in emphysema due to air trapping. Diffusion capacity (DLCO) measures alveolar gas exchange efficiency — reduced in emphysema (alveolar destruction). Recall also the oxygen-haemoglobin dissociation curve — its significance in COPD: the Bohr effect (acidosis/hypercapnia right-shifts the curve, promoting oxygen offloading to tissues). And recall the concept of hypoxic drive: in severe COPD with chronic CO₂ retention, the respiratory centre adapts to use hypoxia (not hypercapnia) as its primary drive for breathing — over-correcting hypoxia can dangerously reduce ventilatory drive.
COPD in the Elderly: Pathophysiology and Presentation
Chronic obstructive pulmonary disease (COPD) is a common, preventable, and treatable disease characterised by persistent respiratory symptoms and airflow limitation due to airway and/or alveolar abnormalities, usually caused by significant exposure to noxious particles or gases. The GOLD (Global Initiative for Chronic Obstructive Lung Disease) definition requires post-bronchodilator FEV₁/FVC < 0.70 on spirometry to confirm the diagnosis. In the elderly, this spirometric threshold requires careful interpretation because of age-related FEV₁ decline — the FEV₁/FVC ratio naturally falls with age even in the absence of COPD; using the fixed ratio threshold of 0.70 may over-diagnose COPD in elderly never-smokers and under-diagnose it in younger smokers. Using the lower limit of normal (LLN) — derived from reference equations stratified by age, sex, and height — is more precise but less operationally available.
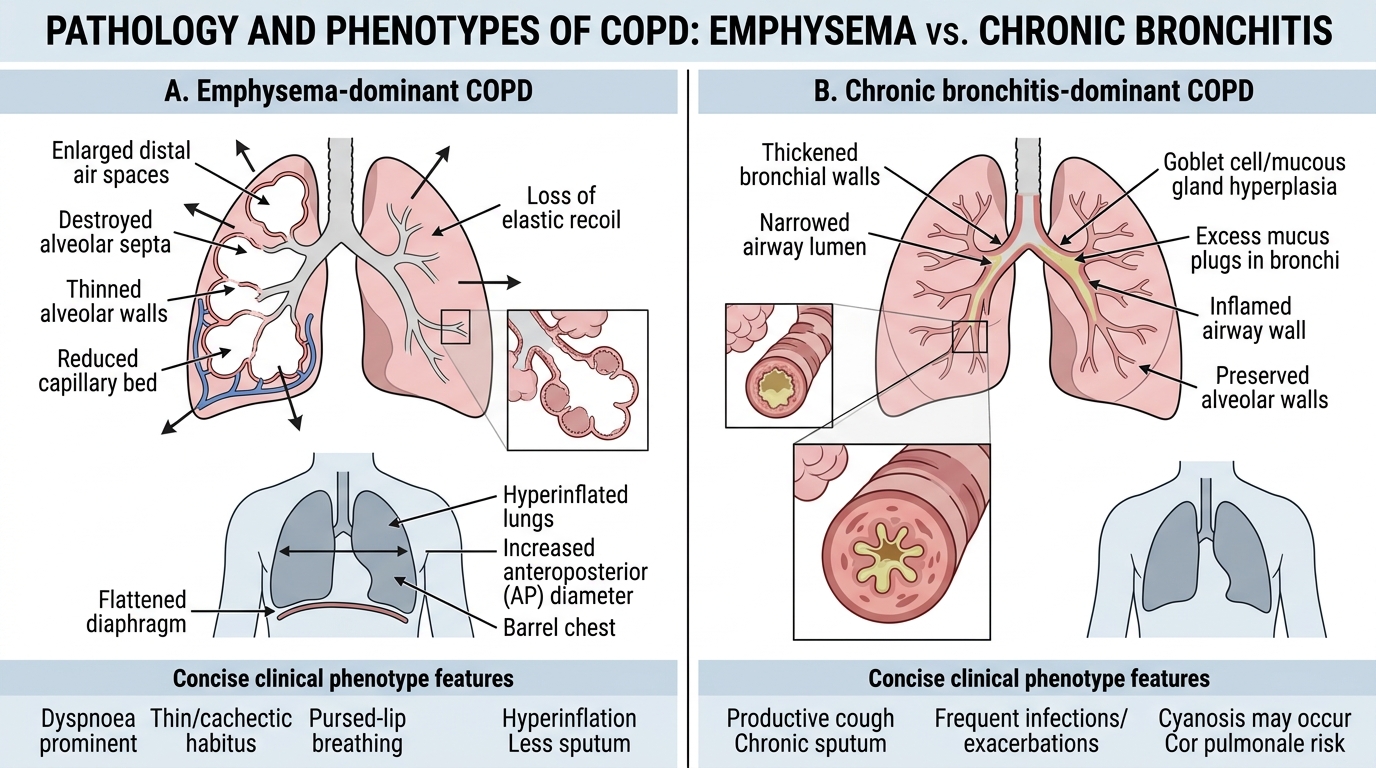
Pathological components of COPD: Two processes coexist in varying proportions: (1) Chronic bronchitis — defined clinically as productive cough for ≥3 months per year for ≥2 consecutive years; pathologically, mucosal gland hypertrophy (Reid index >0.4), goblet cell metaplasia, and chronic inflammatory infiltration of the bronchial wall; leads to increased airway resistance and mucus hypersecretion — the 'blue bloater' phenotype (type B). (2) Emphysema — defined pathologically as abnormal permanent enlargement of the airspaces distal to the terminal bronchioles, with destruction of alveolar walls without obvious fibrosis; leads to loss of alveolar surface area (reduced DLCO), loss of elastic recoil (air trapping, barrel chest, hyperinflation), and dynamic airway collapse during expiration — the 'pink puffer' phenotype (type A). Most elderly COPD patients have a mixed picture.
Indian-specific risk factors: While tobacco smoking is the dominant cause worldwide, Indian COPD has distinctive additional contributors: biomass fuel combustion (wood, dung, crop residue burning for cooking — indoor air pollution; disproportionately affects rural women and non-smoking elderly exposed over decades); occupational dust (agriculture, construction, textile, mining); outdoor air pollution (PM2.5 and NO₂ exposure in urban areas); and childhood respiratory infections (early-life lung function deficits that compound age-related decline). The spirometric phenotype of biomass COPD may differ from tobacco COPD: more airway-predominant disease, less emphysema.
Atypical presentation in elderly COPD: The classical presenting symptoms — dyspnoea on exertion, productive cough, and wheeze — may be underreported in elderly patients because: (a) activity curtailment (elderly patients gradually reduce their activity level to avoid dyspnoea, so exertional breathlessness may not be volunteered as a problem); (b) attribution to ageing ('I'm just getting old, doctor'); (c) cognitive impairment (reduced ability to describe and quantify symptoms). Clinical examination may reveal: barrel chest (increased AP diameter), hyperresonance on percussion, reduced breath sounds with prolonged expiration, pursed-lip breathing, use of accessory muscles, and signs of cor pulmonale in advanced disease (elevated JVP, ankle oedema, right ventricular heave, loud P2). Important: digital clubbing is NOT a feature of COPD — its presence should prompt investigation for lung malignancy, bronchiectasis, or interstitial lung disease.
Emphysema vs Chronic Bronchitis Pathology in COPD
COPD Diagnosis, Staging and Management
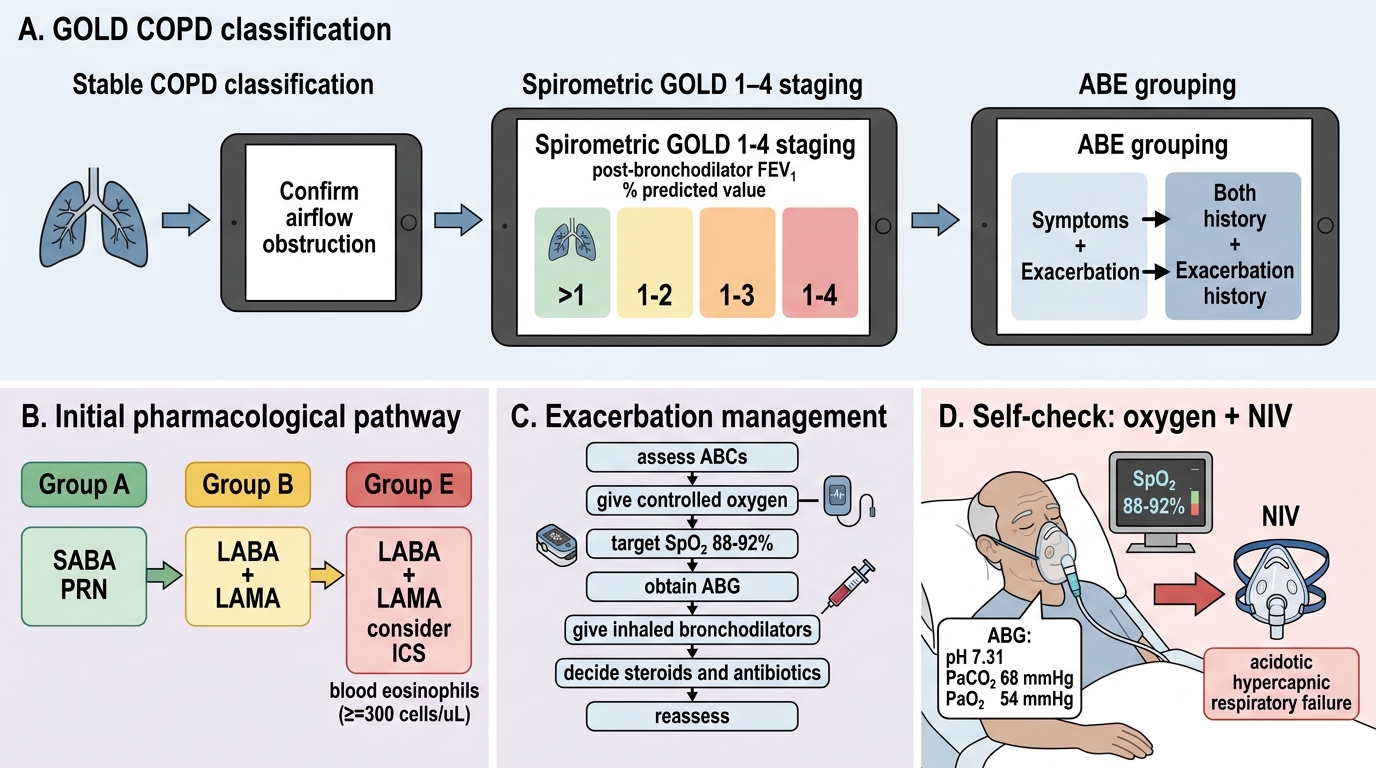
The GOLD spirometric staging of COPD severity is based on post-bronchodilator FEV₁ as percentage of predicted value in patients with confirmed airflow obstruction (FEV₁/FVC <0.70): GOLD 1 (mild): FEV₁ ≥80% predicted; GOLD 2 (moderate): 50% ≤ FEV₁ < 80%; GOLD 3 (severe): 30% ≤ FEV₁ < 50%; GOLD 4 (very severe): FEV₁ < 30%. However, the GOLD 2023 update emphasises that spirometric grade does not fully capture COPD severity — the ABE classification additionally considers symptom burden (mMRC dyspnoea scale or CAT score) and exacerbation history (frequency and severity) to stratify patients into groups A, B, and E (formerly C and D merged into E based on exacerbation risk). Group B: GOLD 1–2 + high symptoms; Group E: any GOLD grade + ≥2 moderate exacerbations per year or ≥1 hospitalised exacerbation. Subramaniam's FEV₁ 31% (GOLD 3) with multiple hospitalisations = Group E.
Stable COPD management — pharmacological: The bronchodilator backbone of COPD management: short-acting beta-2 agonists (SABA — salbutamol MDI 100 mcg/puff, 2 puffs PRN for immediate relief) and long-acting bronchodilators. For most stable COPD: long-acting beta-2 agonist (LABA) (salmeterol, formoterol, indacaterol) + long-acting muscarinic antagonist (LAMA) (tiotropium, glycopyrronium, umeclidinium). Dual bronchodilation with LABA + LAMA is superior to either agent alone and is now the recommended initial maintenance therapy for symptomatic stable COPD. Inhaled corticosteroids (ICS) — added in patients with Group E (frequent exacerbations) especially with blood eosinophil count ≥300 cells/μL (eosinophilic phenotype predicts ICS response). The triple combination LABA + LAMA + ICS is used for group E with high eosinophil counts or frequent exacerbations. ICS monotherapy is NOT recommended in COPD (unlike asthma) — must be combined with bronchodilators. Roflumilast (PDE4 inhibitor, oral) — add-on for Group E with FEV₁ <50% and chronic bronchitis phenotype to reduce exacerbation frequency. Azithromycin (250–500 mg three times weekly) — prophylactic for frequent exacerbations in ex-smokers; reduces exacerbation frequency in selected patients. N-acetylcysteine (mucolytic) — limited evidence but commonly used in India for chronic bronchitis phenotype.
Long-term oxygen therapy (LTOT): Indicated when PaO₂ ≤55 mmHg (SpO₂ ≤88%) at rest on room air on two measurements ≥3 weeks apart, or PaO₂ 56–59 mmHg with cor pulmonale, polycythaemia, or nocturnal desaturation. LTOT ≥15 hours/day improves survival in severe COPD (NOTT and MRC trials, 1980 — still the landmark evidence). Target SpO₂ in LTOT: 88–92% (avoid over-correction in CO₂ retainers — maintaining hypoxic drive safety). Pulmonary rehabilitation — structured supervised exercise training and disease education — is the most effective intervention for improving exercise tolerance, dyspnoea, and quality of life in stable COPD (Cochrane: mean improvement in 6-minute walk distance approximately 43 metres); eligible from GOLD 2 onwards.
COPD exacerbation management: An exacerbation is an acute event characterised by worsening respiratory symptoms beyond normal day-to-day variation. The commonest precipitant in elderly patients is bacterial infection (Haemophilus influenzae, Streptococcus pneumoniae, Moraxella catarrhalis) or viral infection (rhinovirus, influenza). Assessment severity: CURB-65 is designed for pneumonia; exacerbation severity uses clinical indicators: SpO₂, respiratory rate, use of accessory muscles, ABG (type 1 = low PaO₂, normal/low PaCO₂; type 2 = respiratory failure with elevated PaCO₂ — CO₂ retention). Management: controlled oxygen (target SpO₂ 88–92% — NOT 94–98% to avoid hypercapnic respiratory failure in type 2 respiratory failure); nebulised SABA (salbutamol) and SAMA (ipratropium); systemic corticosteroids (prednisolone 40 mg daily ×5 days — reduces recovery time and treatment failure; equivalent to 5-day course); antibiotics if clinical evidence of bacterial infection (increased sputum volume, purulence — amoxicillin 500 mg TDS ×5 days first-line or doxycycline/co-amoxiclav; adjust based on local resistance patterns); NIV (non-invasive ventilation, BiPAP) for type 2 respiratory failure (PaCO₂ >6 kPa with acidosis pH <7.35) — reduces intubation and hospital mortality (evidence from Brochard 1995, plant 2000); venous thromboembolism prophylaxis (low-molecular-weight heparin — COPD exacerbation is prothrombotic state).
GOLD COPD Classification and Management Algorithm
SELF-CHECK
A 74-year-old man with severe COPD (GOLD 3, FEV₁ 35%) is admitted with an exacerbation. On arrival: RR 28/min, SpO₂ 82% on air. Arterial blood gas: pH 7.31, PaO₂ 54 mmHg, PaCO₂ 68 mmHg. He is alert and cooperative. What is the MOST appropriate initial oxygen strategy?
A. High-flow oxygen via non-rebreather mask to achieve SpO₂ ≥95% as rapidly as possible
B. Controlled oxygen via Venturi mask (24–28% FiO₂) to achieve target SpO₂ 88–92%, and arrange non-invasive ventilation for the acidotic hypercapnic respiratory failure
C. No oxygen until ABG is repeated — risk of inducing hypercapnic coma
D. Immediate intubation and mechanical ventilation — pH 7.31 mandates invasive support
Reveal Answer
Answer: B. Controlled oxygen via Venturi mask (24–28% FiO₂) to achieve target SpO₂ 88–92%, and arrange non-invasive ventilation for the acidotic hypercapnic respiratory failure
This patient has type 2 respiratory failure (elevated PaCO₂ = 68 mmHg) with acidosis (pH 7.31). The target SpO₂ in COPD with known or suspected CO₂ retention is 88–92% — achieving this corrects life-threatening hypoxia without suppressing hypoxic drive (which in chronic CO₂ retainers is the dominant ventilatory stimulus). Over-oxygenation (SpO₂ >94%) worsens hypercapnia via the Haldane effect and abolishes hypoxic drive. The acidotic hypercapnic respiratory failure (pH 7.31, PaCO₂ 68) is the indication for NIV (BiPAP) — which reduces intubation rates and mortality. Intubation is not the first step when NIV is available and the patient is alert and cooperative.
Geriatric Surgical Care: Perioperative Assessment and Optimisation
Surgery in the elderly is not merely 'the same operation in an older body' — it is a distinct clinical context in which the physiological reserve of the patient determines the outcome as much as the technical skill of the surgeon. Approximately 30% of all surgical procedures are performed on patients aged 65 years and above. Elderly patients have a 3–10 fold higher rate of post-operative mortality and morbidity compared to younger patients undergoing equivalent procedures, driven by reduced physiological reserve (homeostenosis), frailty, multimorbidity, polypharmacy, and pre-operative nutritional and cognitive impairment.
Pre-operative risk assessment: The ASA Physical Status Classification (I–VI) provides a simple, widely used grading of physiological reserve: ASA I (healthy), ASA II (mild systemic disease), ASA III (severe systemic disease — not incapacitating, e.g., controlled COPD, diabetes), ASA IV (severe systemic disease that is a constant threat to life — e.g., acute MI, acute respiratory failure), ASA V (moribund — not expected to survive 24 hours without the operation). Most elderly surgical patients are ASA III–IV. The Revised Cardiac Risk Index (RCRI — Lee 1999) quantifies perioperative major adverse cardiac event (MACE) risk in non-cardiac surgery: 6 independent predictors (high-risk surgery, ischaemic heart disease, heart failure, cerebrovascular disease, diabetes on insulin, serum creatinine >2 mg/dL) — each scores 1 point; ≥3 points = >11% MACE risk. The ACS NSQIP Surgical Risk Calculator provides procedure-specific risk estimates incorporating multiple patient variables.
Cardiopulmonary assessment: All elderly patients undergoing intermediate or high-risk surgery should have 12-lead ECG, full blood count, metabolic panel, and coagulation screen pre-operatively. Echocardiography if clinical evidence of cardiac disease or unexplained reduced exercise tolerance. Pulmonary function testing (spirometry, DLCO) — indicated before major thoracic surgery (pneumonectomy/lobectomy — calculate predicted post-operative FEV₁; minimum threshold for pneumonectomy: ppo-FEV₁ ≥40%; for lobectomy ≥30%) and in any elderly patient with known or suspected COPD undergoing major abdominal/thoracic surgery. Six-minute walk test (6MWT) — measures functional exercise capacity; <400 metres predicts higher post-operative complication rate.
Frailty assessment before surgery: The Clinical Frailty Scale (CFS) or Fried frailty phenotype should be applied to all elderly patients undergoing elective or semi-elective surgery. Frailty (CFS ≥5 or Fried ≥3/5) is an independent predictor of post-operative 30-day mortality (OR approximately 2.5), prolonged hospital stay, post-operative delirium, and failure to return home. Frailty should be documented and disclosed as part of the surgical consent discussion. In urgent/emergency surgery, frailty cannot be modified but the information guides post-operative intensity of monitoring, prophylaxis, and rehabilitation planning. For elective surgery, prehabilitation — structured pre-operative exercise, nutritional optimisation, and medical comorbidity control for 4–8 weeks before surgery — can partially reverse frailty and reduce post-operative complication rates.
Polypharmacy and medication management in the perioperative period: Comprehensive medication review using STOPP/START criteria before surgery. Critical drug management: anticoagulants — warfarin stopped 5 days pre-operatively with heparin bridging for high-risk patients (mechanical valves, recent VTE, high CHA₂DS₂-VASc AF); DOACs stopped 24–48 hours pre-operatively depending on renal function and agent (dabigatran — longer in CKD; apixaban/rivaroxaban shorter half-life); antiplatelet therapy — aspirin continued through surgery in patients with ischaemic heart disease (risk of coronary stent thrombosis if stopped); clopidogrel stopped 5–7 days pre-operatively; corticosteroids — patients on chronic steroids require surgical stress dosing to prevent adrenal crisis: hydrocortisone 25–50 mg IV 8-hourly for minor surgery, 50–100 mg IV 8-hourly for major surgery, tapering over 24–48 hours back to baseline; metformin — stop 24–48 hours before major surgery and when contrast given (risk of lactic acidosis in AKI); ACE inhibitors/ARBs — omit morning of surgery (risk of refractory hypotension on anaesthetic induction).
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
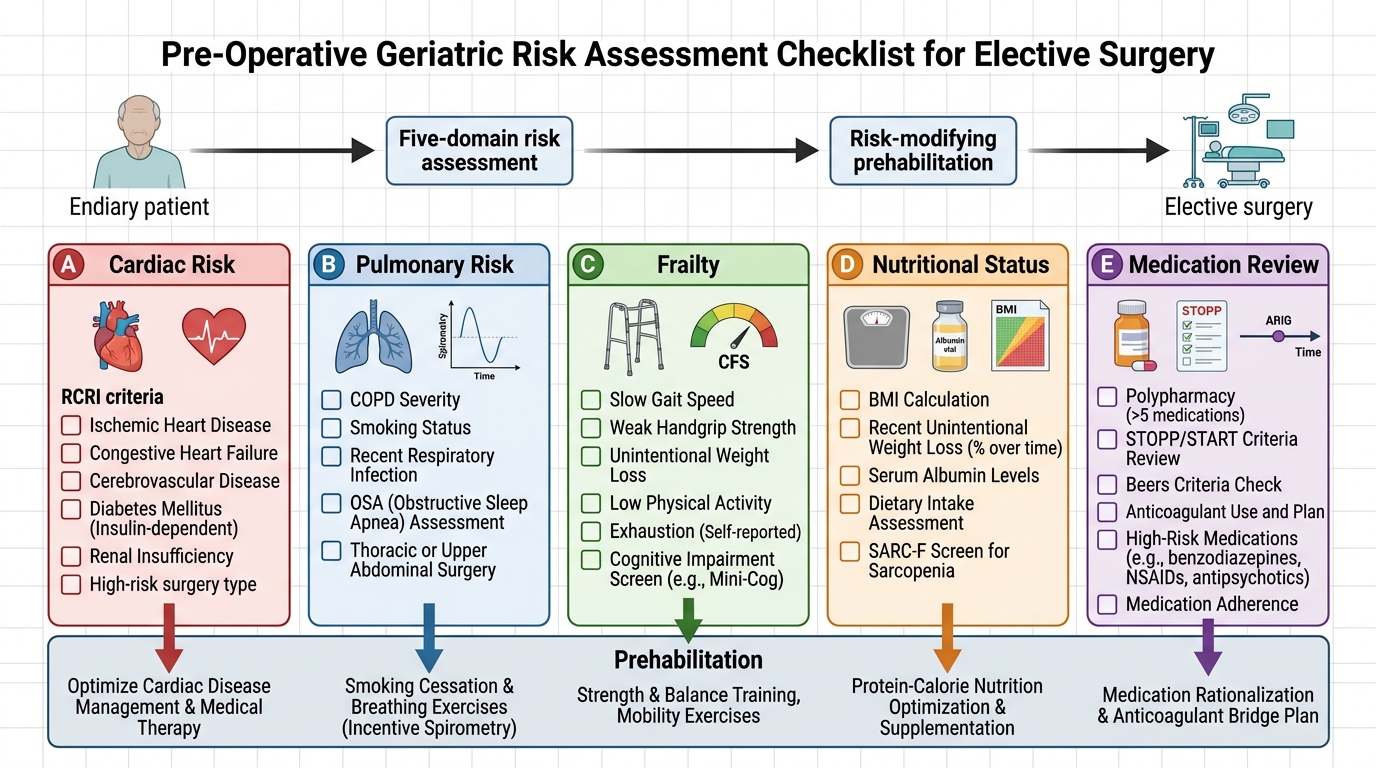
Pre-operative Geriatric Risk Assessment and Prehabilitation