Page 14 of 32
IM25.10-11 | Geriatric COPD and Surgical Care — SDL Guide (Part 2)
Post-Operative Management and Rehabilitation in the Elderly
Post-operative management of the elderly patient extends beyond the immediate recovery room and requires anticipation and prevention of the complications that are disproportionately common in this age group. The four most important post-operative complications in elderly patients are: delirium (post-operative delirium occurs in 15–25% of elderly general surgical patients and up to 50% following hip fracture surgery; it is independently associated with prolonged hospital stay, increased mortality, and accelerated cognitive decline — prevention with the HELP bundle, adequate analgesia, avoidance of anticholinergic drugs, and early mobilisation); respiratory complications (pneumonia, atelectasis, respiratory failure — the most common cause of post-operative mortality in COPD patients); venous thromboembolism (DVT/PE — elderly patients have higher baseline coagulation activity and are more immobile post-operatively; LMWH prophylaxis for all non-ambulatory post-operative elderly patients); and renal impairment (post-operative AKI from hypotension, nephrotoxic drugs, contrast — especially dangerous in pre-existing CKD).
Post-operative respiratory management in COPD patients: COPD-specific risks: atelectasis (increased with general anaesthesia), sputum retention (impaired mucociliary clearance), and bronchospasm. Prevention strategies: incentive spirometry (sustained maximal inspiration — reduces atelectasis); physiotherapy (active cycle of breathing techniques, early mobilisation); nebulised bronchodilators continued through the perioperative period; epidural analgesia or regional anaesthetic techniques where possible (reduce need for systemic opioids that suppress respiratory drive — a specific risk in CO₂ retainers); NIV (BiPAP) post-operatively if signs of respiratory failure emerging — reduces post-operative intubation in COPD. Suction and postural drainage for retained secretions. High-dependency or ICU monitoring for COPD GOLD 3–4 patients after major abdominal or thoracic surgery.
Analgesia in elderly surgical patients: Effective post-operative pain control is essential — inadequately treated pain causes sympathetic activation (tachycardia, hypertension — hazardous in coronary artery disease), impairs deep breathing and coughing (increasing respiratory complications), promotes delirium, and delays mobilisation. The analgesic ladder requires modification for the elderly: paracetamol is first-line (1 g QDS — maximum in elderly with liver disease or low body weight); NSAIDs avoided or minimised (GI bleeding, renal impairment, fluid retention — a STOPP criterion post-operatively); weak opioids (tramadol, codeine — use with caution; tramadol lowers seizure threshold and causes serotonin syndrome risk; codeine is a prodrug requiring CYP2D6 — poor metabolisers get no analgesia, ultra-rapid metabolisers get toxic morphine levels); strong opioids (morphine, fentanyl) in minimum effective doses with laxative co-prescription (constipation is universal with opioids in elderly; ileus risk is high). Regional anaesthetic techniques (wound infiltration, nerve blocks, epidural) reduce systemic opioid requirement and are strongly preferred.
Nutritional support and delirium prevention: Post-operative malnutrition in elderly patients delays wound healing, impairs immune function, reduces muscle mass, and prolongs rehabilitation. Resume oral feeding as soon as feasible (early feeding within 24 hours after most gastrointestinal operations reduces infection and length of stay). Oral nutritional supplements (ONS — high-calorie, high-protein drinks) if oral intake inadequate. Nasogastric or parenteral nutrition for patients unable to eat for >5–7 days. Delirium prevention bundle (HELP programme): familiar faces and objects, glasses and hearing aids from day 1, consistent nursing staff, clock and calendar, early mobilisation, adequate analgesia, avoid urinary catheterisation if not essential, avoid anticholinergic medications, protect sleep (night-time noise reduction, adjust lighting).
Rehabilitation after surgery: The goal is return to pre-surgical functional status — or better (via prehabilitation and rehabilitation). Physiotherapy begins day 1: sitting out of bed, standing, mobilising with assistance. Occupational therapy for ADL retraining and assistive device assessment. Discharge planning from admission: identifying social support requirements, home modifications, community physiotherapy, outpatient follow-up. Enhanced Recovery After Surgery (ERAS) protocols — multimodal perioperative care bundles including pre-operative carbohydrate loading, minimal fasting, regional anaesthesia, early feeding, and early mobilisation — reduce hospital stays by 1–3 days and complication rates by 30–50%, particularly relevant in colorectal and orthopaedic surgery.
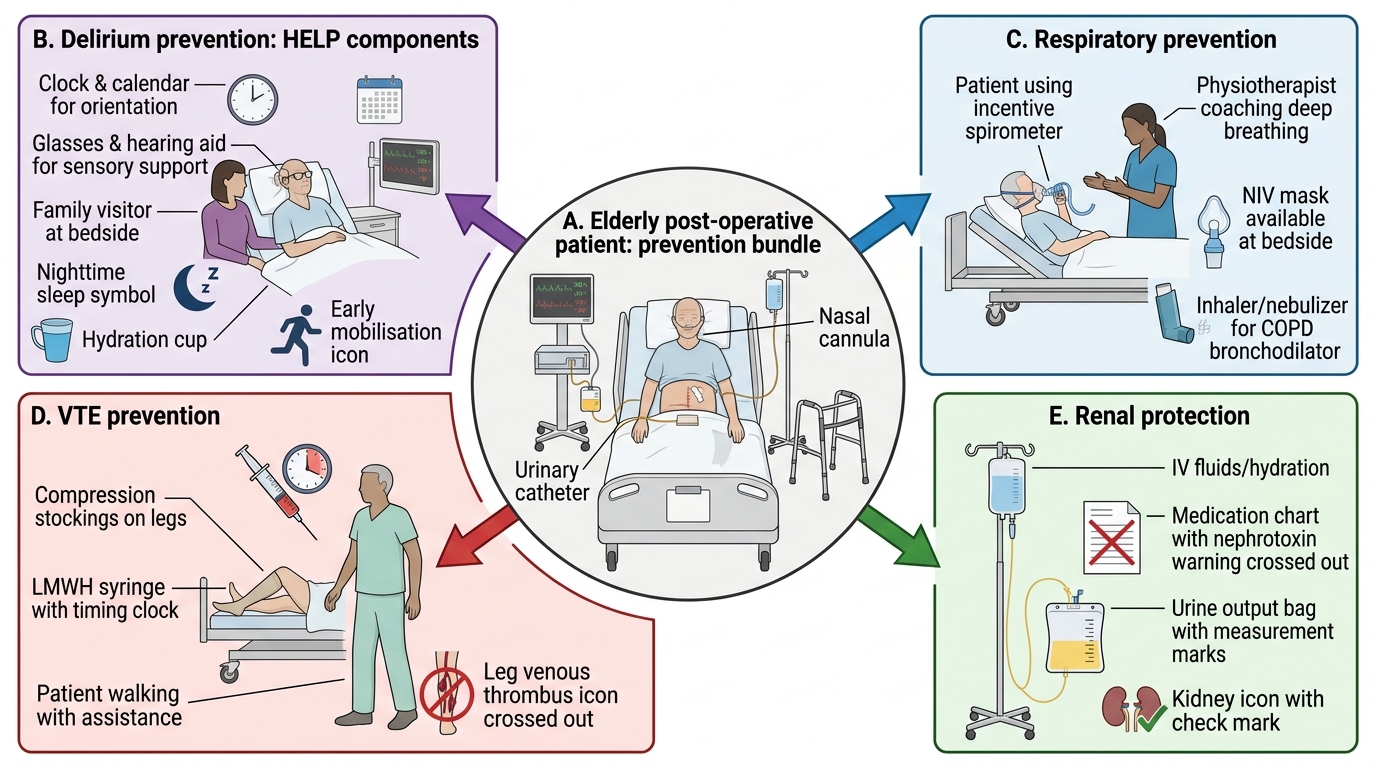
Post-operative Complication Prevention Bundle in Elderly Surgical Patients
SELF-CHECK
A 78-year-old man with COPD (GOLD 3) and ischaemic heart disease is admitted for elective sigmoid colectomy. He takes prednisolone 7.5 mg daily for his COPD, warfarin for AF (INR 2.4 on last check), aspirin 75 mg, and atorvastatin. Which perioperative medication management plan is MOST correct?
A. Stop prednisolone 5 days before surgery; continue warfarin through surgery; stop aspirin 7 days before surgery
B. Continue all medications unchanged — perioperative changes are only for anticoagulants
C. Give surgical stress-dose hydrocortisone (50–100 mg IV 8-hourly) during major surgery; stop warfarin 5 days pre-operatively with heparin bridging assessment; continue aspirin
D. Stop prednisolone and aspirin 5 days before surgery; switch to DOAC the night before
Reveal Answer
Answer: C. Give surgical stress-dose hydrocortisone (50–100 mg IV 8-hourly) during major surgery; stop warfarin 5 days pre-operatively with heparin bridging assessment; continue aspirin
Three separate principles apply: (1) Patients on chronic corticosteroids (prednisolone 7.5 mg/day) have suppressed HPA axis and require surgical stress-dose hydrocortisone to prevent adrenal crisis — 50–100 mg IV 8-hourly for major surgery, tapering back post-operatively. Simply stopping steroids pre-operatively would cause adrenal crisis. (2) Warfarin: stop 5 days pre-operatively; heparin bridging depends on CHA₂DS₂-VASc/AF stroke risk — this patient has AF with ischaemic heart disease and high scores, so bridging LMWH is appropriate until the morning of surgery. (3) Aspirin: continue in patients with ischaemic heart disease — stopping causes platelet rebound and risk of coronary stent thrombosis; perioperative aspirin continuation is standard in known coronary artery disease.
Self-Assessment: COPD and Surgical Care in Elderly Scenarios
These clinical scenarios integrate the full arc of both topics — stable and exacerbation COPD management in elderly patients and the perioperative geriatric assessment framework. Apply the management principles from this module before reading the analysis.
Scenario A: Mrs Kamakshi, 72 years old, is a non-smoker but has cooked over a wood-fire stove for 50 years. She presents with progressive breathlessness on exertion, chronic productive cough, and two hospitalisations in the past year. Spirometry: post-bronchodilator FEV₁ 48% predicted, FEV₁/FVC 0.61. Blood eosinophil count 450 cells/μL. She is on tiotropium alone. What further management change is indicated based on the GOLD framework?
Analysis: GOLD grade: FEV₁ 48% = GOLD 2. Exacerbation history: 2 hospitalisations in the past year = Group E (≥1 hospitalised exacerbation). Current therapy: LAMA alone is insufficient for Group E. Indicated next step: add LABA (e.g., formoterol or indacaterol) to achieve LABA + LAMA dual bronchodilation; and given blood eosinophil count 450 cells/μL (well above the 300 threshold predicting ICS response), add inhaled corticosteroid (triple therapy LABA + LAMA + ICS). Also: confirm biomass exposure (key history in Indian context); refer to pulmonary rehabilitation; annual influenza and pneumococcal vaccination (both evidence-based for reducing COPD exacerbations); check LTOT eligibility with resting SpO₂ and ABG. Risk of biomass COPD in women is an important Indian-specific pattern.
Scenario B: Mr Rajan, 79 years old with severe COPD (GOLD 4, FEV₁ 24%, PaCO₂ chronically 55 mmHg), is admitted with an exacerbation. On arrival he is drowsy, RR 22, SpO₂ 79% on air, pH 7.27, PaO₂ 48 mmHg, PaCO₂ 82 mmHg. He is maintained on LTOT at home (28% Venturi, 15 hours/day). What is the immediate management priority for this exacerbation?
Analysis: Severe type 2 respiratory failure with acidosis (pH 7.27) and drowsiness. Immediate NIV (BiPAP) is the most critical intervention — pH <7.35 with hypercapnia is the indication; drowsiness does not contraindicate NIV if the patient can protect his airway and cooperate minimally. Controlled oxygen: Venturi 28% to achieve SpO₂ 88–92% — no higher (severe CO₂ retainer). Simultaneously: salbutamol and ipratropium nebulisation (driven by air, not oxygen, to avoid oxygen-driven hypercapnia); IV or oral prednisolone 40 mg; antibiotics (amoxicillin or doxycycline). If pH does not improve with 1–2 hours of NIV and the patient deteriorates → discuss escalation with ICU. A goals-of-care conversation is appropriate given GOLD 4 disease and recurrent hospitalisations — intubation and mechanical ventilation may not be in the patient's best interest; an advance directive discussion is clinically and ethically appropriate at this point.
Scenario C: Mr Krishnaswamy, 84 years old, falls and sustains a fractured neck of femur (displaced subcapital). He has COPD (GOLD 3), hypertension, mild dementia (MMSE 22/30), and is taking amlodipine, tiotropium, and lorazepam. The orthopedic team proposes hemiarthroplasty under general anaesthesia. His CFS score is 6 (moderately frail). What are the key pre-operative considerations and post-operative priorities specific to his geriatric profile?
Analysis: Pre-operative: (1) RCRI assessment — no high-risk cardiac factors listed but COPD GOLD 3 = elevated pulmonary risk; ECG, metabolic panel, ABG if possible. (2) Stop lorazepam (benzodiazepine) — causes post-operative delirium and falls risk; taper not possible in emergency setting but anaesthetist should minimise sedatives. (3) Frailty (CFS 6) — inform surgical team; affects post-op recovery trajectory; document for consent; priority for post-op intensive rehabilitation and delirium prevention. (4) COPD management: continue tiotropium; prepare nebulised bronchodilators for post-op. (5) FIX 48 principle — surgery within 48 hours despite medical complexity. Post-operative priorities: NIV/respiratory physiotherapy (COPD + post-general anaesthesia atelectasis = high respiratory complication risk); HELP delirium prevention bundle (dementia doubles delirium risk); early mobilisation day 1; LMWH thromboprophylaxis; start bisphosphonate/zoledronate before discharge for osteoporosis. Goals-of-care discussion with family regarding realistic rehabilitation expectations given frailty and dementia.
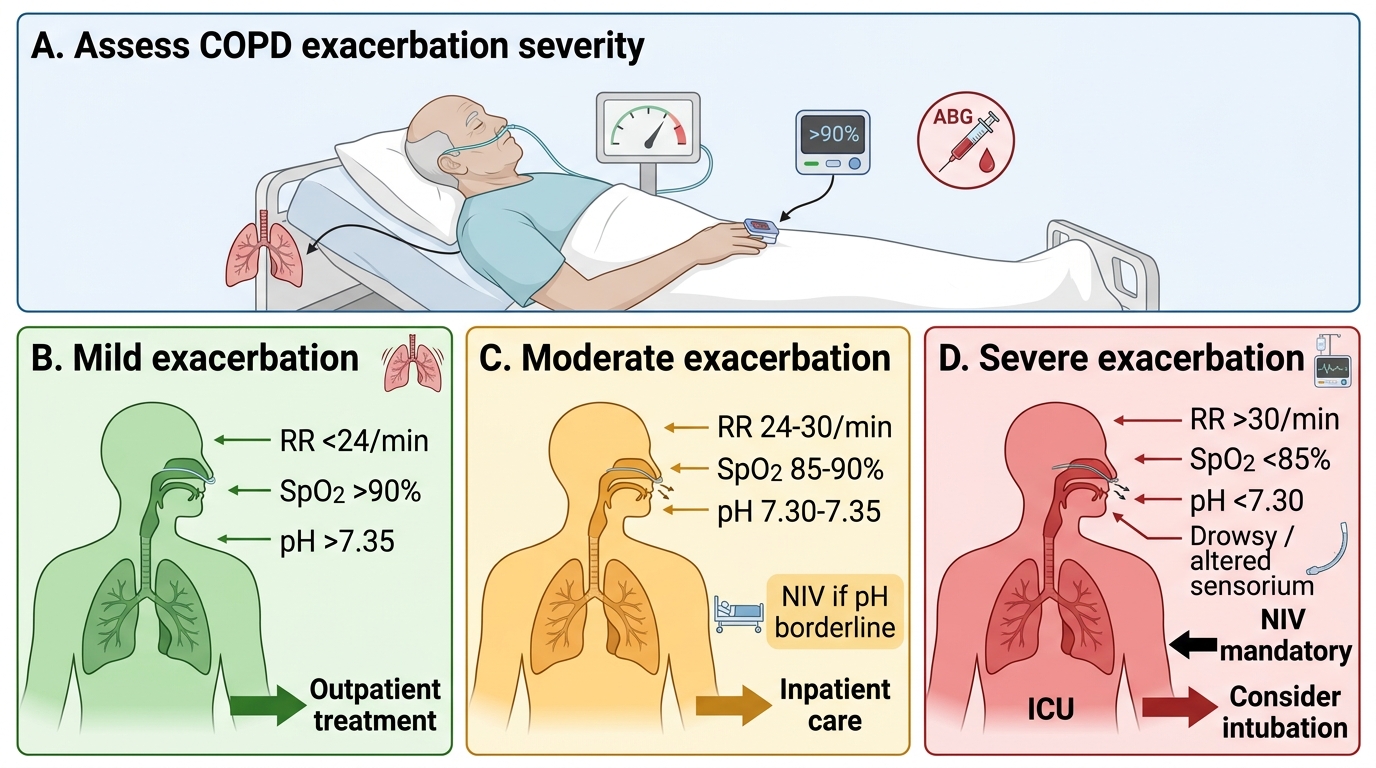
COPD Exacerbation Severity and Treatment Targets
CLINICAL PEARL
Two rules that prevent the most common dangerous errors in geriatric COPD and surgical care: (1) In COPD exacerbation with type 2 respiratory failure, the oxygen target is 88–92% — NOT 94–98%. Over-oxygenating a chronic CO₂ retainer suppresses hypoxic drive, worsens hypercapnia via the Haldane effect, and can precipitate hypercapnic coma. Use a controlled Venturi mask, not a simple face mask. (2) Patients on long-term systemic corticosteroids who undergo surgery require surgical stress-dose hydrocortisone — not steroid cessation. The HPA axis is suppressed by doses ≥5 mg/day for ≥3 months; without stress dosing, adrenal crisis (hypotension refractory to fluids and vasopressors) can occur intraoperatively or in the post-operative period. Any elderly patient on 'a steroid for their lungs or their joints' must have this risk flagged before surgery.