Page 5 of 35
IM26.{8-11,14,17} | Bacterial Skin Visceral Urinary and Enteric Infections — SDL Guide
Learning Objectives
- Describe the common causes, clinical features, and management of skin, muscle, and soft-tissue infections including cellulitis, necrotising fasciitis, and pyomyositis
- Describe the common causes, clinical features, and management of liver and other visceral abscesses
- Describe the common causes, clinical features, and management of acute infectious diarrhoeal diseases and bacterial food poisoning
- Describe the common causes, clinical features, and management of urinary tract infections, pyelonephritis, and prostatitis
- Describe the common causes, clinical features, and management of diseases caused by Gram-negative enteric bacilli
- Describe the etiopathogenesis, clinical features, complications, and management of enteric fever
INSTRUCTIONS
This module covers the most commonly encountered bacterial infections in Indian internal medicine practice, grouped by organ system. The emphasis is on pattern recognition — identifying the syndrome from clinical features — and selecting the correct empirical antibiotic regimen guided by the likely organism and local resistance patterns. Each organ-system section follows the arc: causative organisms → pathogenesis → clinical features → investigations → management.
References
- Harrison's Principles of Internal Medicine, 21st ed., Chapters 121–136 — Bacterial Infections (textbook)
- API Textbook of Medicine, 10th ed., Section 7 — Infectious Diseases (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 13 — Infectious Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 48-year-old diabetic man presents to the emergency department with a swollen, erythematous right leg that has worsened rapidly over 18 hours. He has fever (39.2°C), tachycardia (114/min), and the skin over the calf has a dark, blistered discolouration with a 'wooden' texture on palpation — the skin feels hard rather than fluctuant. In the adjacent bed, a 32-year-old woman has had 5 days of dysuria, left flank pain, and fever with rigors; her urine dipstick shows 3+ leucocytes and nitrite-positive. In the outpatient department, a 22-year-old food vendor's assistant describes 8 hours of profuse watery diarrhoea and vomiting after a communal meal — 12 others from the same meal are similarly affected. Three patients, three organ systems, three bacterial syndromes — each demanding a different approach, different investigations, and different antibiotics with strikingly different urgency. The diabetic man's necrotising fasciitis demands surgical consultation in the next hour; delay means limb loss or death. The woman's pyelonephritis needs blood and urine cultures and IV antibiotics within hours. The food poisoning likely needs only oral rehydration. Recognising the syndrome and calibrating the urgency — that is the skill this module builds.
WHY THIS MATTERS
Bacterial infections of the skin and soft tissues, the urinary tract, the gastrointestinal system, and the liver are among the five most common causes of emergency medical admissions in India. Enteric fever alone accounts for an estimated 11–14 million cases annually in India, predominantly in children and young adults. Community-acquired UTI is the most common bacterial infection requiring antibiotic prescription in general practice. Necrotising fasciitis carries a mortality of 20–40% and requires early surgical recognition — making it one of the few infectious emergencies where the physician's decision to call the surgeon (not the microbiologist first) is the most important clinical action. The NMC competencies IM26.8–IM26.17 cover these high-frequency, high-stakes bacterial syndromes. Mastery here directly translates to daily clinical practice.
RECALL
Before proceeding, recall the relevant microbiology. Gram-positive cocci (Staphylococcus aureus, Streptococcus pyogenes) are the dominant pathogens in skin and soft-tissue infections; S. aureus produces a range of toxins (protein A, PVL toxin in community-MRSA, TSST-1 in toxic shock syndrome) and can produce both superficial and invasive disease. Gram-negative bacilli — particularly the Enterobacteriaceae family (E. coli, Klebsiella, Proteus, Serratia) — dominate urinary tract and enteric infections; their outer membrane LPS triggers the host inflammatory cascade. Salmonella species are intracellular pathogens that survive within macrophages, explaining the systemic nature and chronicity of enteric fever. Entamoeba histolytica and Staphylococcus aureus are the most common causes of liver abscess in India, producing clinically distinct syndromes. The concept of colonisation vs invasion is critical: the normal flora of the GI tract includes E. coli, but only specific virulent strains with pathogenicity islands cause diarrhoea or systemic infection.
Skin, Muscle, and Soft-Tissue Infections
Skin and soft-tissue infections (SSTIs) span a spectrum from superficial, self-limiting conditions to life-threatening surgical emergencies. The clinical priority is to identify the depth of involvement and the presence of tissue necrosis — because necrotising infections require immediate surgical debridement, not just antibiotics, and hours matter in that diagnosis.
Impetigo is the most superficial bacterial skin infection, caused by Staphylococcus aureus (non-bullous and bullous forms) or Streptococcus pyogenes (non-bullous form). It presents as honey-coloured crusted lesions around the mouth and nares in children, or as flaccid bullae in bullous impetigo (S. aureus exfoliative toxin A or B cleaves desmoglein-1). Treatment: topical mupirocin for localised disease; oral cloxacillin or dicloxacillin for widespread or recurrent cases.
Cellulitis is a non-purulent, spreading infection of the dermis and subcutaneous tissues. The commonest causative organisms are S. pyogenes (Group A Streptococcus) and S. aureus. Clinically: spreading erythema, warmth, tenderness, and swelling — typically affecting the lower limb, often with a portal of entry (interdigital tinea, wound, insect bite). Systemic features (fever, tachycardia, raised CRP/WBC) indicate severity. Treatment: oral cefalexin or cloxacillin for mild cases; IV benzylpenicillin + cloxacillin for hospitalised patients; add cover for MRSA (vancomycin or linezolid) if risk factors (healthcare exposure, prior MRSA, immunocompromised).
Erysipelas is a superficial form of cellulitis with sharp, raised, well-demarcated borders — indicating that the infection is confined to the dermis and superficial lymphatics rather than extending to the subcutaneous tissue. Exclusively caused by Group A (or occasionally Group B/C/G) Streptococcus. Facial (butterfly distribution involving the cheeks and nose) or lower-limb presentation. Treatment: penicillin V orally or IV benzylpenicillin.
Abscess (furuncle/carbuncle): S. aureus accounts for >80% of abscesses. A furuncle is a deep-seated infection of a single hair follicle with central suppuration; a carbuncle is a coalescence of multiple furuncles with multiple draining sinuses, typically on the nape of the neck or back, seen in diabetics and immunocompromised patients. Management: incision and drainage is the definitive treatment; antibiotics are indicated if there is surrounding cellulitis, systemic features, or the patient is immunocompromised.
Necrotising fasciitis is the most devastating SSTI and constitutes a surgical emergency. It is defined by infection of the deep fascia with rapidly spreading necrosis of the fascia and overlying subcutaneous tissue, with relative sparing of the skin until late in the disease course — a feature that leads to diagnostic delay. Type I is polymicrobial (aerobic + anaerobic, including Streptococcus, Staphylococcus, E. coli, Bacteroides, and Clostridium) and occurs typically in diabetics, the immunocompromised, and post-surgical patients. Type II is mononicrobial, caused by S. pyogenes (Group A Streptococcus) alone, and can occur in previously healthy individuals.
The key clinical features that distinguish necrotising fasciitis from cellulitis are:
- Pain disproportionate to skin appearance in the early phase (before the skin shows obvious change)
- Skin findings: erythema progressing to grey-blue discolouration, haemorrhagic bullae, skin necrosis
- Woody induration on palpation — the subcutaneous tissues feel fixed to deep fascia, unlike the soft fluctuance of an abscess
- Crepitus (subcutaneous gas) — present in gas-forming infections (Type I, clostridial) but NOT always present
- Systemic toxicity out of proportion to local findings: high fever, tachycardia, hypotension, altered mentation
- The finger test: intraoperative insertion of a finger through a 2 cm incision — if the tissues dissect easily with no bleeding and there is no resistance (the tissue planes separate without cutting), necrotising fasciitis is confirmed
Management: IMMEDIATE surgical debridement is life-saving; no amount of antibiotics can substitute for surgical removal of necrotic tissue because the avascular necrotic fascia creates an antibiotic dead zone. IV antibiotic combination: meropenem (or imipenem) + clindamycin + IV immunoglobulin (IVIG) in severe streptococcal cases. Hyperbaric oxygen is adjunctive where available. ICU support for septic shock.
Pyomyositis is primary bacterial infection of skeletal muscle producing an intramuscular abscess. Rare in temperate countries but relatively common in tropical climates (including India) — hence formerly called 'tropical pyomyositis.' Predominantly caused by S. aureus. Typically affects the large muscles of the thigh, buttock, or calf. Presents with localised muscle pain and tenderness, indurated swelling, fever, and leucocytosis. MRI confirms the diagnosis and delineates the abscess. Treatment: drainage + IV cloxacillin (or vancomycin if MRSA suspected) for 4–6 weeks.
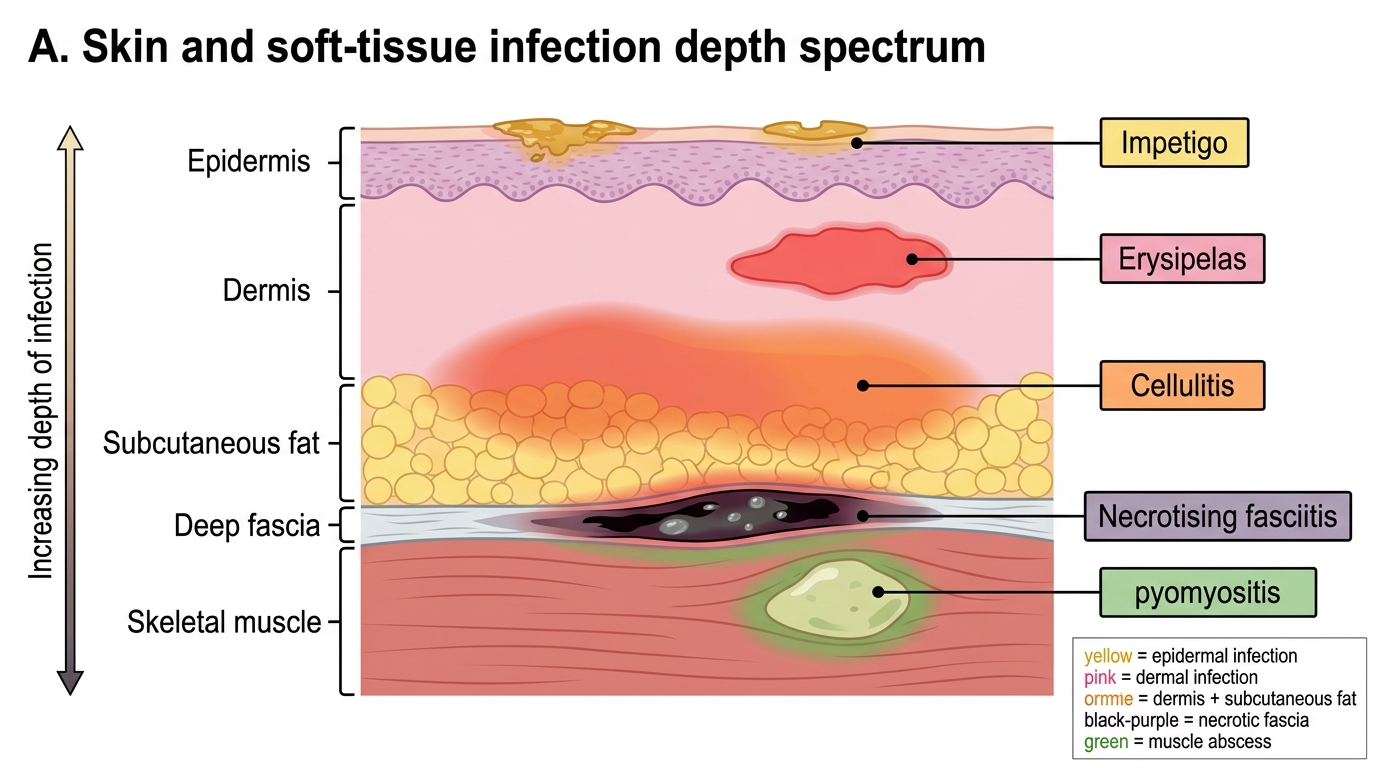
Skin and Soft-Tissue Infection Depth Spectrum
Liver and Visceral Abscesses
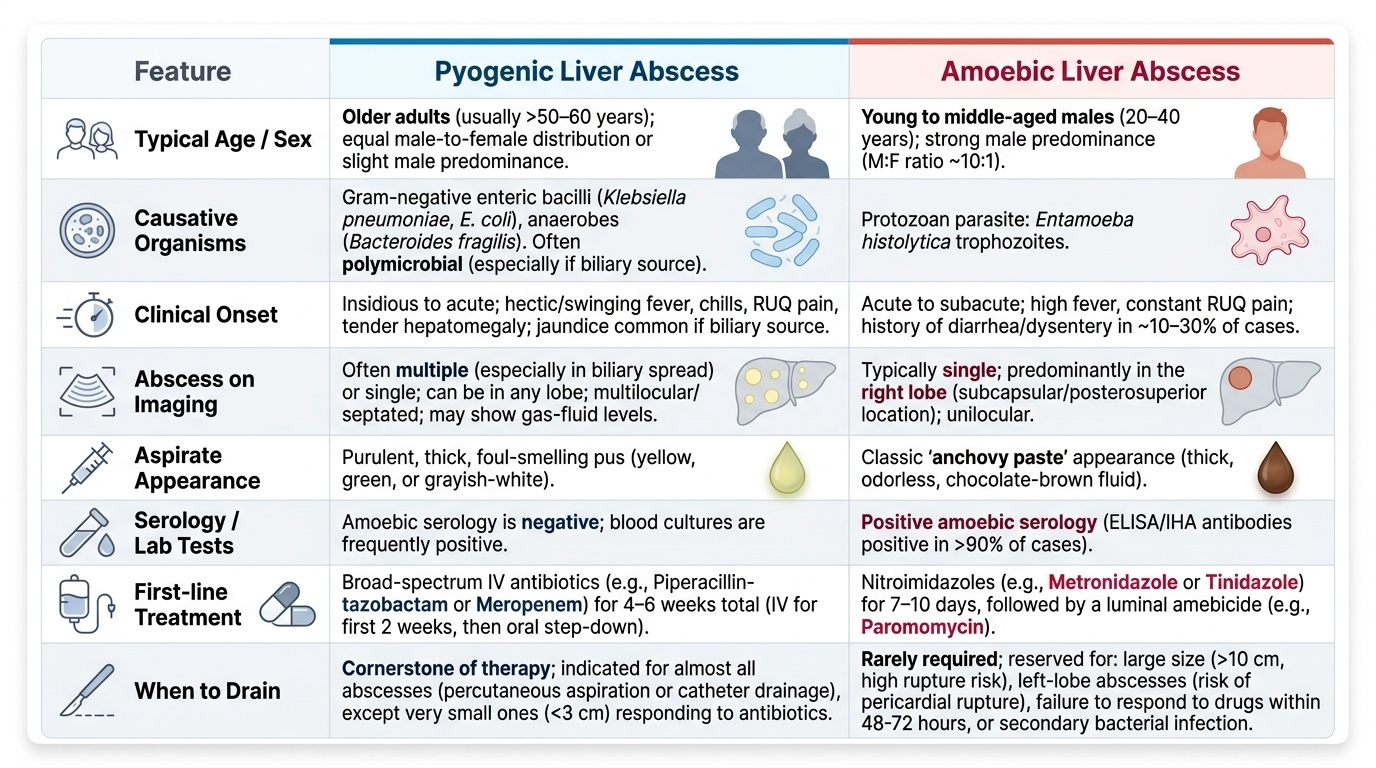
Liver abscess is the most common visceral abscess in India and presents an important diagnostic challenge because its two commonest forms — pyogenic and amoebic — have overlapping clinical features but require entirely different treatments. Distinguishing them is a fundamental clinical skill that has direct therapeutic consequences.
Provided image
Pyogenic (bacterial) liver abscess results from haematogenous spread of bacteria from a portal vein source (appendicitis, diverticulitis, perforated viscus, inflammatory bowel disease — portal pyaemia), from biliary obstruction with superimposed infection (ascending cholangitis — the most common source in India), or from direct extension of a neighbouring infection. The dominant organisms are Gram-negative enteric bacilli: Klebsiella pneumoniae (increasingly the dominant pathogen, especially in diabetics — associated with a syndrome of primary liver abscess with haematogenous spread to eye, brain, and lung), E. coli, and anaerobes (Bacteroides fragilis). Polymicrobial infections are common in biliary sources.
Clinical features: insidious onset of fever (often hectic, swinging), right upper quadrant pain, tender hepatomegaly, and anorexia/weight loss. Jaundice indicates biliary source or extensive hepatic involvement. Diaphragmatic irritation produces referred right shoulder pain and right-sided pleural effusion. Investigations: ultrasound (preferred first-line — single or multiple hypoechoic lesions, avascular on Doppler), CT with contrast (delineates lesion, biliary anatomy, and source), CBC (leucocytosis with neutrophilia), LFTs (elevated ALP most consistently), blood cultures. Serology: amoebic serology (ELISA for E. histolytica antibodies) is critical to distinguish pyogenic from amoebic abscess.
Management of pyogenic liver abscess: percutaneous ultrasound-guided or CT-guided aspiration or drainage is the cornerstone of treatment (both diagnostic — sends pus for culture — and therapeutic). Small abscesses (<3 cm) may respond to antibiotics alone. IV antibiotics: piperacillin-tazobactam or meropenem (covering both Gram-negative aerobes and anaerobes) for 4–6 weeks total (IV for 2 weeks then oral).
Amoebic liver abscess is caused by Entamoeba histolytica trophozoites that invade the intestinal epithelium, enter the portal circulation, and lodge in the liver (predominantly the right lobe) where they cause liquefactive necrosis of hepatocytes — producing the characteristic 'anchovy sauce' or 'chocolate brown' pus (lysed hepatocytes, not true pus). It is the most common form of invasive amoebiasis in India. Important epidemiological context: E. histolytica infection is primarily enteric; only ~1% of intestinal infections progress to invasive liver disease, and up to 20% of amoebic liver abscess patients have no preceding diarrhoeal history.
Clinical features: acute onset of high fever, severe right upper quadrant pain (may radiate to right shoulder), tender hepatomegaly, and systemic toxicity. Unlike pyogenic abscess, the leucocytosis is marked (WBC 15,000–25,000) but the patient often looks more toxic for the size of the abscess. Key discriminating features from pyogenic: younger age (20–50 years), male predominance (male:female ~10:1), single abscess in the right lobe, no biliary source, positive amoebic serology (IHA titre ≥1:512 or ELISA IgG positive — sensitivity >95%), and aspirate is sterile on bacterial culture.
Management: Metronidazole 800 mg three times daily × 10 days is highly effective (>90% response without drainage). Needle aspiration is indicated only for: (a) impending rupture (abscess >10 cm or left-lobe abscess threatening the pericardium), (b) failure to respond to metronidazole in 72 hours, (c) diagnostic uncertainty. Follow with diloxanide furoate 500 mg three times daily × 10 days to eradicate intestinal cysts and prevent recurrence and spread.
SELF-CHECK
A 35-year-old male labourer presents with 5 days of high fever, severe right upper quadrant pain, and tender hepatomegaly. WBC 22,000/µL. Ultrasound shows a single 8 cm hypoechoic lesion in the right lobe. Amoebic ELISA (IgG) is positive. Bacterial culture of the aspirate is sterile. The MOST appropriate management is:
A. Percutaneous drainage only — metronidazole is not effective for amoebic liver abscess
B. IV piperacillin-tazobactam for pyogenic cover plus percutaneous drainage
C. Oral metronidazole 800 mg three times daily for 10 days, with aspiration reserved for impending rupture or non-response
D. IV metronidazole 500 mg three times daily for 10 days with immediate surgical drainage
Reveal Answer
Answer: C. Oral metronidazole 800 mg three times daily for 10 days, with aspiration reserved for impending rupture or non-response
This is a classic presentation of amoebic liver abscess — young male, acute onset, right lobe single abscess, positive amoebic serology, sterile culture. The first-line treatment is oral metronidazole 800 mg TID for 10 days; drainage is NOT routinely needed. Aspiration is indicated if the abscess is >10 cm (risk of rupture), in left lobe (pericardial rupture risk), or if there is no improvement in 72 hours on metronidazole. This abscess is 8 cm — close to the threshold but not yet an absolute indication; a trial of metronidazole first is appropriate. Pyogenic antibiotics are unnecessary given positive amoebic serology and sterile culture.
Acute Infectious Diarrhoea and Bacterial Food Poisoning
Acute infectious diarrhoea — defined as ≥3 loose or watery stools in 24 hours for <14 days — is one of the leading causes of morbidity and mortality worldwide, and in India it is responsible for over 300,000 deaths annually, predominantly in children under 5 years. However, adult general medicine also encounters infectious diarrhoea frequently, particularly in food poisoning outbreaks, travellers' diarrhoea, and immunocompromised patients. The clinical approach distinguishes three major pathophysiological categories: secretory (watery, large-volume, painless), invasive (dysenteric — bloody, mucoid, small-volume, with tenesmus and fever), and toxin-mediated food poisoning (typically rapid onset after a communal meal). Each category has a distinct microbial aetiology and a distinct management approach.
Secretory (non-inflammatory) diarrhoea is caused by organisms that produce enterotoxins stimulating fluid secretion without invading or destroying intestinal epithelium. Key examples:
- Vibrio cholerae (O1 and O139 serotypes): the toxin (cholera toxin — CT-B binds to GM1 ganglioside; CT-A activates adenylate cyclase) causes massive secretion of isotonic fluid — up to 20 L/day — without blood or pus. Characteristic rice-water stool: copious, colourless, watery, with a faint sweet smell. Rapidly fatal without rehydration (death within hours from hypovolumic shock). Treatment: oral rehydration solution (ORS) — the single most important treatment in cholera; IV fluids (Ringer's lactate) for severe dehydration; doxycycline 300 mg single dose or tetracycline shortens illness duration and reduces infectivity.
- Enterotoxigenic E. coli (ETEC): major cause of traveller's diarrhoea and endemic infantile diarrhoea; LT and ST toxins mimic and synergise with cholera toxin. Self-limited; ORS is primary treatment.
- Giardia lamblia: a protozoan but produces watery, malabsorptive diarrhoea; important in immunocompromised patients and travellers; treated with metronidazole or tinidazole.
Invasive (inflammatory) diarrhoea (dysentery) occurs when the pathogen invades or destroys colonic epithelium, producing bloody, mucoid stool with tenesmus and fever. Key examples:
- Shigella spp. (bacillary dysentery): most virulent enteric pathogen — infectious dose as low as 10–100 organisms; invades colonic epithelium via M cells and spreads laterally; causes severe dysentery with fever, crampy abdominal pain, tenesmus, and blood/mucus in stool. Complications: HUS (Shiga toxin of S. dysenteriae type 1), toxic megacolon, seizures in children (Ekiri syndrome). Treatment: ciprofloxacin 500 mg twice daily × 3 days (check local resistance); ceftriaxone for severe/resistant cases; avoid antidiarrhoeal agents (loperamide) which prolong illness.
- Campylobacter jejuni: most common bacterial cause of diarrhoea in developed countries; frequent in India in children and travellers; watery diarrhoea progressing to bloody; self-limited in most cases; azithromycin for severe/persistent cases; important: can trigger Guillain-Barré syndrome post-infection (molecular mimicry).
- Salmonella enteritidis/typhimurium (non-typhoidal salmonellosis, NTS): food-borne via poultry, eggs; watery diarrhoea ± blood; self-limited in immunocompetent; bacteraemia and extraintestinal seeding in sickle-cell disease and immunocompromised. Antibiotics (ciprofloxacin or ceftriaxone) only for severe or bacteraemic disease — not for uncomplicated NTS.
- Entamoeba histolytica (amoebic dysentery): see parasitic SDL for detail; flask-shaped ulcers in colon; bloody mucoid stool; metronidazole.
Bacterial food poisoning is distinct from infectious diarrhoea in that illness is caused by pre-formed toxin ingested with the food, producing rapid-onset symptoms (typically 1–6 hours) in a group of people who shared the same meal:
- Staphylococcus aureus enterotoxin: onset 1–6 hours after ingestion of contaminated dairy, cream, or meat products; nausea, vomiting, and watery diarrhoea; usually self-limited in <24 hours; no antibiotic needed.
- Bacillus cereus: two syndromes — emetic form (short incubation 1–5 hours, preformed toxin in reheated rice; nausea/vomiting predominant) and diarrhoeal form (longer incubation 8–16 hours, enterotoxin; diarrhoea predominant). Self-limited; no antibiotics.
- Clostridium perfringens: onset 8–16 hours after consumption of reheated meat; watery diarrhoea without vomiting; spores germinate in reheated food, produce enterotoxin. Self-limited; no antibiotics.
Management principles for all acute infectious diarrhoea: (1) Oral rehydration is the cornerstone — WHO standard ORS (glucose 75 mmol/L, sodium 75 mmol/L, potassium 20 mmol/L) or home-made solutions; IV Ringer's lactate for severe dehydration; (2) Antibiotics are not needed for most acute infectious diarrhoea (self-limited), except in severe dysentery, cholera (shortens illness), immunocompromised patients, and travellers with severe symptoms; (3) Anti-motility agents (loperamide) are contraindicated in bloody diarrhoea/dysentery — they promote systemic absorption of toxins and increase the risk of toxic megacolon.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
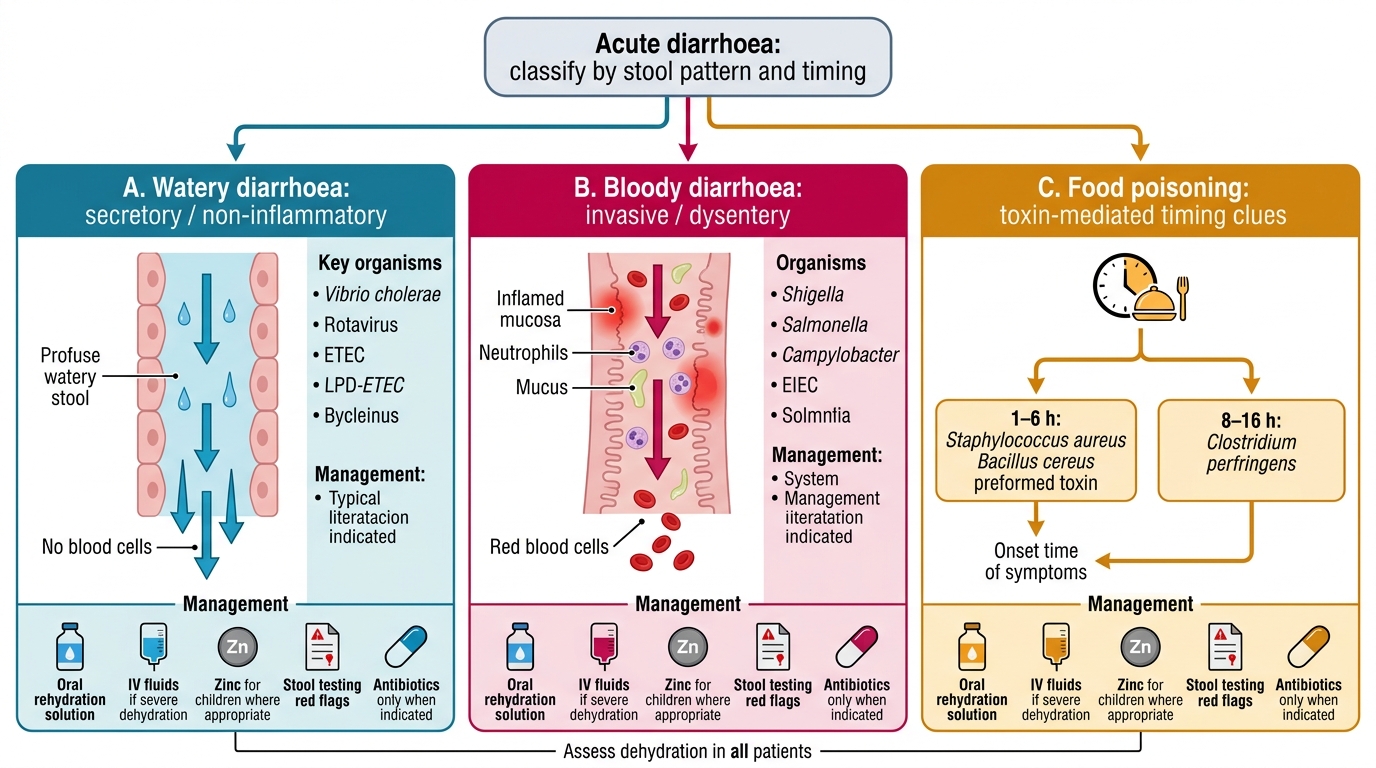
Acute Diarrhoea Classification and Management Algorithm