Page 6 of 35
IM26.{8-11,14,17} | Bacterial Skin Visceral Urinary and Enteric Infections — SDL Guide (Part 2)
Urinary Tract Infections and Pyelonephritis
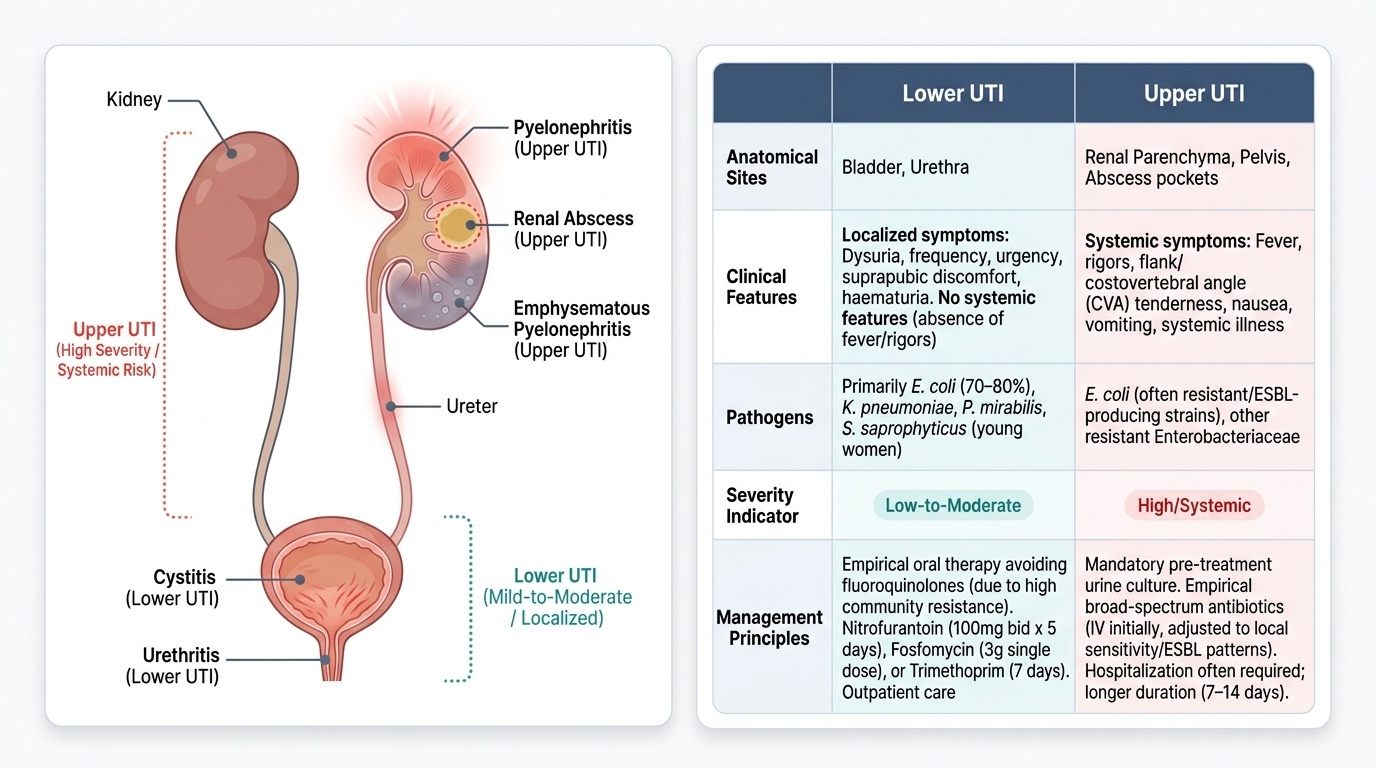
Urinary tract infections (UTIs) are the most common bacterial infections encountered in general practice and represent a major driver of antibiotic prescriptions worldwide. In India, the high prevalence of ESBL-producing Enterobacteriaceae in community-acquired UTI means that empirical antibiotic selection must account for local resistance patterns rather than applying global guidelines uncritically. The anatomical distinction between lower UTI (cystitis, urethritis) and upper UTI (pyelonephritis, renal abscess) is critical because it determines route of antibiotic administration, duration, and the need for hospitalisation.
Provided image
Uncomplicated lower UTI (cystitis) affects predominantly women (50–70% of women experience at least one UTI in their lifetime) due to the short female urethra and proximity to the bowel flora. The causative organism is E. coli in 70–80% of cases; other Enterobacteriaceae (Klebsiella pneumoniae, Proteus mirabilis, Enterobacter spp.) account for most of the remainder. Staphylococcus saprophyticus is an important cause in sexually active young women. Clinical features: dysuria, urinary frequency, urgency, suprapubic discomfort, and haematuria; no systemic features (fever, rigors, flank pain). Investigations: dipstick (leucocyte esterase + nitrite has >80% sensitivity/specificity); urine culture confirms the diagnosis and guides de-escalation but is not mandatory for uncomplicated cystitis in otherwise healthy women. Treatment: India-specific empirical choice — avoid fluoroquinolones (resistance >40–60% in community E. coli in many Indian states); options: nitrofurantoin 100 mg modified-release twice daily × 5 days (if eGFR >45), fosfomycin 3g single dose, or trimethoprim × 7 days if local resistance <20%. Duration: 3–5 days for uncomplicated premenopausal women; 7 days for postmenopausal women.
Complicated UTI is defined by any factor that increases the risk of treatment failure or ascent to the upper tract: urological abnormality (obstruction, calculi, vesicoureteral reflux, stent, catheter, ileal conduit), functional abnormality (neurogenic bladder), immunocompromise (diabetes, HIV, transplant), pregnancy, or the male sex (any UTI in a male is by definition complicated because it implies a structural or functional abnormality). Treatment requires urine culture before antibiotics, broader-spectrum coverage, longer duration (7–14 days), and treatment of the underlying structural abnormality.
Pyelonephritis (upper UTI) results from ascent of bacteria from the bladder to the renal pelvis and parenchyma. Clinically: fever (often high, with rigors), flank pain, and costovertebral angle (CVA) tenderness on percussion — plus the lower urinary symptoms of cystitis. Nausea and vomiting are common. Investigations: urine microscopy (pyuria ≥5 WBC/HPF, bacteriuria), urine culture (mandatory — guides antibiotic choice), blood cultures (positive in 10–20% of patients admitted with pyelonephritis), renal ultrasound (to exclude obstruction, hydronephrosis, or renal abscess). Management: mild cases can be managed with oral fluoroquinolone (if local susceptibility allows); hospitalised patients require IV ceftriaxone 2g daily, IV ciprofloxacin, or (in ESBL-risk patients) IV ertapenem or meropenem. Duration: 10–14 days. Failure to respond in 72 hours mandates ultrasound/CT to exclude renal abscess or obstruction.
Emphysematous pyelonephritis is a severe, necrotising infection of the renal parenchyma with gas formation — almost exclusively in diabetics (gas produced by fermentation of glucose by Klebsiella pneumoniae or E. coli). CT abdomen is diagnostic (gas within renal parenchyma or perinephric space). High mortality (~20%) without prompt treatment. Management: IV carbapenem + percutaneous drainage or nephrectomy for severe cases.
Prostatitis occurs in a significant proportion of men presenting with UTI symptoms. Acute bacterial prostatitis presents with fever, dysuria, frequency, perineal pain, and a tender, swollen, warm prostate on rectal examination (DO NOT vigorously massage — risks bacteraemia). The causative organisms mirror those of UTI (E. coli most common). Treatment: IV ciprofloxacin or ceftriaxone for severe cases; oral fluoroquinolone for 4 weeks for uncomplicated acute prostatitis (fluoroquinolones penetrate prostatic tissue well). Chronic bacterial prostatitis requires 6–12 weeks of fluoroquinolone.
SELF-CHECK
A 28-year-old woman presents with 2 days of fever (38.9°C), right flank pain, and dysuria. Urine dipstick shows 3+ leucocytes, 2+ nitrite. Blood cultures are drawn. She is not allergic to any antibiotics. Her urine culture grows E. coli with sensitivity to ceftriaxone but resistance to ciprofloxacin, trimethoprim, and co-amoxiclav. What is the most appropriate treatment?
A. Oral ciprofloxacin 500 mg twice daily for 7 days — ciprofloxacin penetrates the kidney well
B. IV ceftriaxone 2g daily, with oral step-down when the patient is clinically improving and afebrile
C. Nitrofurantoin 100 mg twice daily for 5 days — adequate for most UTI presentations
D. IV co-amoxiclav 1.2g three times daily for 10 days
Reveal Answer
Answer: B. IV ceftriaxone 2g daily, with oral step-down when the patient is clinically improving and afebrile
This is acute pyelonephritis with systemic features (fever, flank pain) requiring hospitalisation and IV antibiotics. The urine culture shows ciprofloxacin resistance, making oral fluoroquinolone (option A) inappropriate. Nitrofurantoin achieves therapeutic concentrations only in urine — not in renal parenchyma — making it unsuitable for pyelonephritis (it is used only for uncomplicated cystitis). Co-amoxiclav is resistant per culture. IV ceftriaxone 2g daily, with oral step-down to a sensitive oral agent when the patient is clinically improving, is the correct approach. Always check local sensitivity before empirical fluoroquinolone in India.
Gram-Negative Enteric Bacilli Infections and Enteric Fever
Gram-negative enteric bacilli (Enterobacteriaceae) are the dominant bacterial pathogens in healthcare-associated infections worldwide, and in India they cause the majority of community-acquired bloodstream infections, urinary tract infections, and intra-abdominal infections. The Enterobacteriaceae family includes Escherichia coli, Klebsiella pneumoniae, Enterobacter spp., Proteus mirabilis, Serratia marcescens, and Salmonella species. Their shared outer-membrane LPS (endotoxin) is the fundamental trigger of the host septic response, but beyond this shared feature, different members of the family have distinct tropisms, virulence mechanisms, and resistance profiles that determine clinical syndrome and antibiotic choice. What makes the Enterobacteriaceae clinically significant as a group in the Indian context is their capacity to acquire and transmit resistance determinants — particularly ESBL enzymes and carbapenemases — through horizontal gene transfer on plasmids, meaning that a resistance gene that emerged in a hospital setting can spread within weeks to community organisms. This is why empirical antibiotic choices that were standard of care in India 15 years ago (ampicillin, cephalosporins, fluoroquinolones for community-acquired UTI and enteric fever) now fail in a substantial and growing proportion of cases. Understanding the individual organisms' clinical profiles, and the specific resistance threats each poses, is the foundation for rational empirical prescribing in modern Indian medicine.
Key Enterobacteriaceae clinical profiles:
- E. coli: the most common cause of community-acquired UTI, neonatal meningitis (K1 capsule), septicaemia of urinary or biliary source, and traveller's diarrhoea. ESBL-producing E. coli are endemic in India, requiring carbapenem therapy for serious infections.
- Klebsiella pneumoniae: causes primary pneumonia (typically in alcoholics and diabetics — characteristic 'currant jelly' haemorrhagic sputum), UTI, and liver abscess. Hypervirulent K. pneumoniae strains (hypermucoviscous, capsule types K1/K2) cause primary liver abscess with metastatic spread to the eye (endophthalmitis) and brain — a syndrome seen predominantly in Southeast Asian diabetics. Carbapenem-resistant Klebsiella (producing KPC, OXA-48, or NDM-1) is a major therapeutic challenge.
- Proteus mirabilis: urease-producing organism that alkalinises urine, predisposing to struvite renal calculi; important cause of complicated UTI and pyelonephritis, especially in catheterised patients.
- Serratia marcescens: important nosocomial pathogen; intrinsically resistant to ampicillin and first-generation cephalosporins; associated with ICU pneumonia and catheter-associated UTI.
Enteric fever (typhoid and paratyphoid fever) is caused by Salmonella typhi and Salmonella paratyphi A, B, and C. India is endemic for enteric fever, with an estimated annual burden exceeding 11 million cases — predominantly in areas with contaminated water supplies and poor sanitation.
Pathogenesis: S. typhi is ingested via contaminated food or water → survives gastric acid (infectious dose ~10³ organisms) → invades Peyer's patches in the terminal ileum via M cells → taken up by macrophages → replicates intracellularly within the reticuloendothelial system (liver, spleen, bone marrow) → second bacteraemic phase produces systemic illness → organisms shed in bile re-enter the intestinal lumen, and re-invasion of Peyer's patches with immune-mediated necrosis can cause intestinal perforation in the third week. Chronic gallbladder carrier state occurs in 1–4% of patients (facilitated by gallstones).
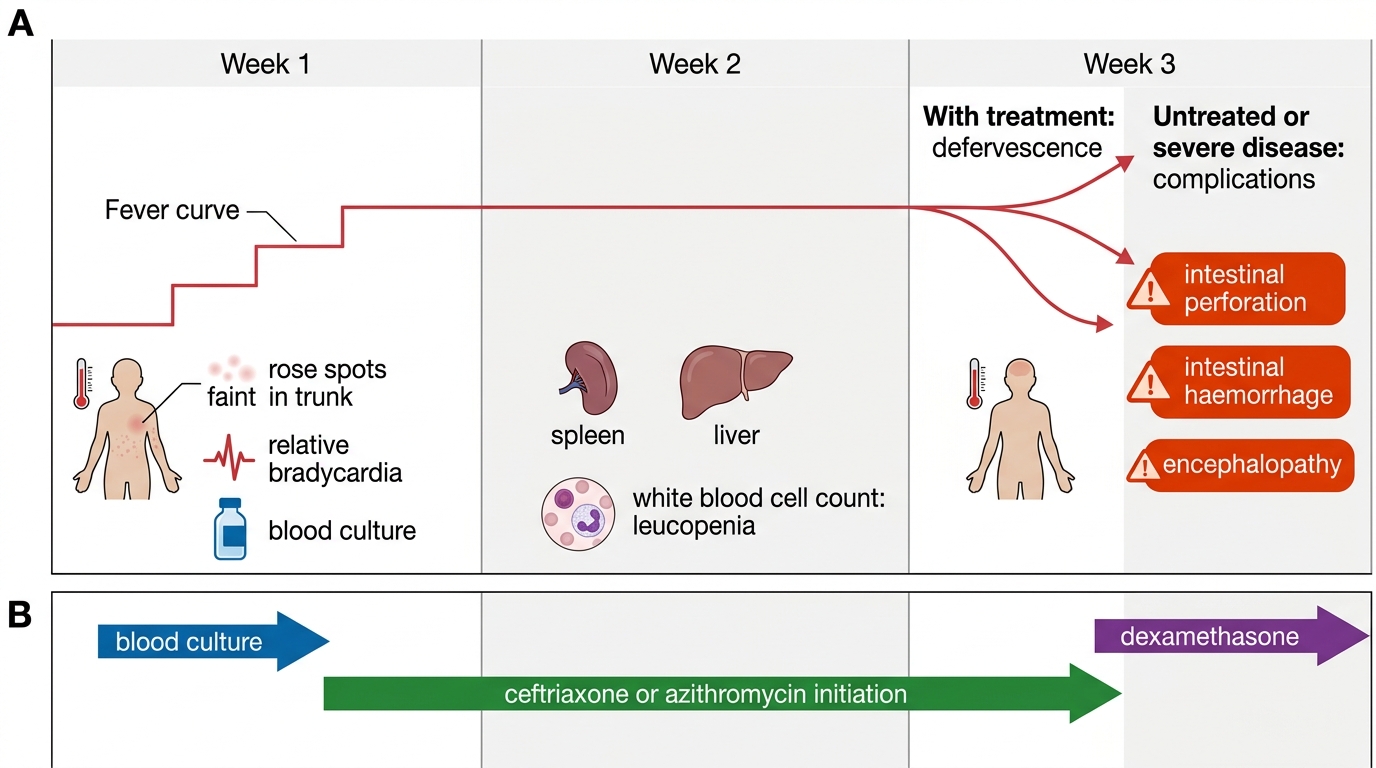
Clinical features evolve in a characteristic stepwise pattern:
- Week 1: insidious onset of fever that increases step-wise day by day ('stepladder pattern'), headache, malaise, dry cough, constipation (more common than diarrhoea in adults). Rose spots (faint salmon-coloured maculopapular lesions on the trunk, visible in fair-skinned patients) appear in the first week in ~20–30% — a classic but often missed finding. Relative bradycardia (heart rate lower than expected for the degree of fever).
- Week 2: fever plateau at 39–40°C, abdominal distension, tender abdomen, splenomegaly, and hepatomegaly. Rose spots may appear or become more visible. Leucopenia with relative lymphocytosis is characteristic. Complications begin to emerge.
- Week 3: defervescence in treated cases; untreated patients may develop complications: intestinal perforation (free air under diaphragm on erect CXR), intestinal haemorrhage, hepatitis, myocarditis, encephalopathy (typhoid toxaemia), haemolytic anaemia, and relapse.
Investigations: Blood culture in the first week (gold standard — sensitivity 60–80%); bone marrow culture (>90% sensitivity — useful when blood culture negative after antibiotics); stool and urine cultures (lower sensitivity). Widal test (serum agglutinins): unreliable as a single-point test in endemic India due to background seropositivity from past infection or vaccination; a four-fold rise in paired titres (2 weeks apart) is meaningful but rarely practical. Typhidot (dot-ELISA for IgM and IgG antibodies): better sensitivity and specificity than Widal in the acute phase.
Management:
- First-line: IV ceftriaxone 2g once daily for uncomplicated enteric fever in hospitalised patients; oral azithromycin 1g daily × 5 days for uncomplicated enteric fever in outpatients (excellent bioavailability, good intracellular penetration, preferred where fluoroquinolone resistance is confirmed).
- Fluoroquinolones (ciprofloxacin): resistance to nalidixic acid (surrogate for fluoroquinolone) is present in >50% of Indian Salmonella isolates — fluoroquinolones are no longer reliably effective; they should not be used empirically without culture-confirmed sensitivity.
- Dexamethasone (0.3 mg/kg IV then 0.1 mg/kg 6-hourly × 48 hours) is indicated for severe typhoid with encephalopathy, delirium, stupor, or coma — the Hoffman-Weber regimen; reduces mortality in severe typhoid by ~50%.
- Intestinal perforation: surgical management (primary repair or resection), antibiotics covering peritoneal flora (meropenem ± metronidazole), ICU care.
- Duration: 7–10 days IV for severe disease; continue oral to complete 14 days total.
- Chronic carrier state: prolonged ciprofloxacin 750 mg twice daily × 4 weeks (+ cholecystectomy if gallstones present).
Enteric Fever: Clinical Timeline and Management
SELF-CHECK
A 22-year-old man from a peri-urban area presents with 9 days of step-wise fever (now 40.2°C), headache, and constipation. He has relative bradycardia and mild splenomegaly. WBC 3,600/µL with lymphocytosis. Blood culture is drawn. Which antibiotic regimen is MOST appropriate for empirical treatment in India given current resistance patterns?
A. Oral ciprofloxacin 500 mg twice daily for 10 days — fluoroquinolones are first-line for Salmonella
B. IV ampicillin 2g four times daily for 14 days
C. IV ceftriaxone 2g once daily (or oral azithromycin 1g daily for uncomplicated outpatient cases) for 7–14 days
D. Oral co-trimoxazole (trimethoprim-sulfamethoxazole) 960 mg twice daily for 14 days
Reveal Answer
Answer: C. IV ceftriaxone 2g once daily (or oral azithromycin 1g daily for uncomplicated outpatient cases) for 7–14 days
This is a classic enteric fever presentation. In India, Salmonella typhi strains show >50% resistance to nalidixic acid (a marker for reduced fluoroquinolone susceptibility) — making empirical ciprofloxacin unreliable. Ampicillin and co-trimoxazole were first-line drugs until multi-drug-resistant strains emerged in the 1990s; resistance to both is now widespread in India. IV ceftriaxone 2g once daily is the current Indian standard of care for hospitalised enteric fever, with oral azithromycin (1g daily × 5 days) as the outpatient alternative for uncomplicated cases. Blood culture before antibiotics is always the priority in the first week.
Management Summary and Antibiotic Stewardship Principles
The bacterial infections covered in this SDL — SSTIs, visceral abscesses, diarrhoeal diseases, UTIs, and enteric fever — share several overarching management principles that reflect the integration of pathogen biology, local resistance patterns, and antimicrobial stewardship in the Indian clinical context. Reviewing these principles consolidates the organ-system-specific management described above into a coherent clinical approach.
Provided image
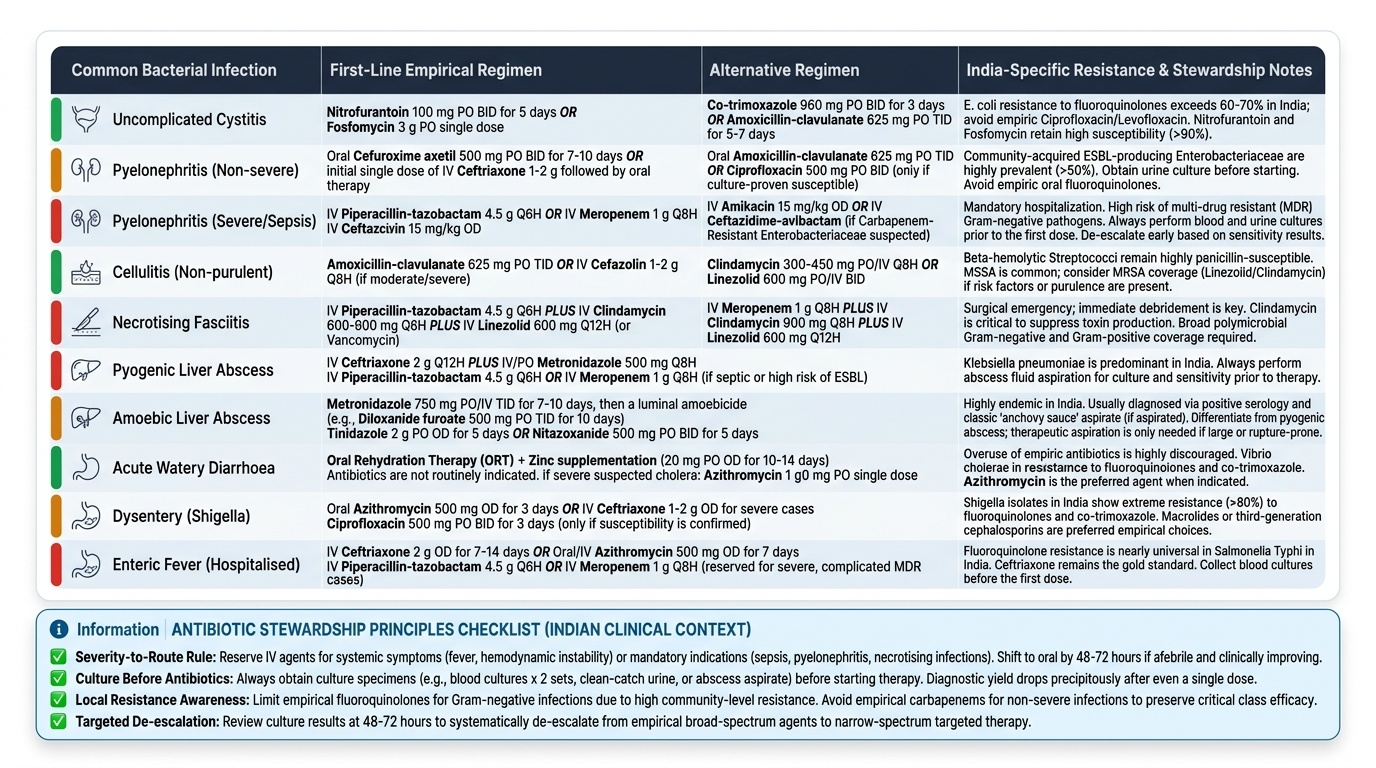
The severity-to-route principle: Mild to moderate infections without systemic features (uncomplicated cystitis, mild cellulitis, mild amoebic dysentery) can be managed with oral antibiotics in outpatients. Systemic features — fever, tachycardia, hypotension, organ dysfunction, or immunocompromise — mandate IV antibiotics and hospitalisation. The specific infections where IV initiation is non-negotiable regardless of patient preference: necrotising fasciitis, pyelonephritis with sepsis, pyogenic liver abscess, enteric fever with complications, and any bacteraemia. Early IV-to-oral switch is appropriate in most bacterial infections when the patient is improving and afebrile — typically at 48–72 hours — and drives down costs and line-related complications.
The culture-before-antibiotics principle: In all potentially serious bacterial infections — suspected bacteraemia, pyelonephritis admitted to hospital, liver abscess, enteric fever — obtain appropriate cultures before starting antibiotics. The yield drops dramatically with even one prior dose. Blood cultures × 2 sets from separate sites; urine culture by midstream clean catch; abscess aspirate for culture and sensitivity. The culture result guides de-escalation from broad-spectrum empirical therapy to a targeted, narrower regimen.
India-specific resistance considerations:
- For UTI/pyelonephritis: ESBL E. coli/Klebsiella prevalence in community UTI in India is 40–70% in many states; empirical cephalosporins will fail in a substantial proportion; for hospitalised pyelonephritis with sepsis or risk factors (prior UTI, prior antibiotics, healthcare exposure), empirical ertapenem or meropenem is justified pending culture. Nitrofurantoin and fosfomycin retain good activity against ESBL producers for uncomplicated cystitis.
- For enteric fever: fluoroquinolone resistance is >50% in India — ceftriaxone IV or azithromycin oral is the empirical regimen of choice.
- For skin and soft-tissue infections: community-acquired MRSA (CA-MRSA) is less prevalent in India than hospital-acquired MRSA (HA-MRSA), but diabetics, IV drug users, and those with prior antibiotic exposure should prompt MRSA cover (vancomycin IV, linezolid oral) for severe SSTIs.
- For Gram-negative bacilli (bacteraemia, pneumonia, intra-abdominal): carbapenem-resistant Enterobacteriaceae (CRE) producing NDM-1 are an emerging crisis; when CRE is confirmed, polymyxin B or colistin-based combinations are required — this situation demands infectious disease specialist input.
The surgical principle in infection: Not all infections respond to antibiotics alone. The following require drainage or debridement in addition to antibiotics: (a) necrotising fasciitis — surgical debridement is life-saving and non-negotiable; (b) pyogenic liver abscess — percutaneous drainage for lesions >5 cm or non-response to antibiotics; (c) empyema — tube thoracostomy; (d) abscess — incision and drainage; (e) prosthetic device infection — removal of the device is often required for cure. Antibiotics penetrate necrotic and avascular tissue poorly; surgery removes the nidus that antibiotics cannot reach.
Vaccine-preventable enteric infections: Typhoid (Vi capsular polysaccharide vaccine or live oral Ty21a vaccine) and cholera (oral killed whole-cell cholera vaccine) are vaccine-preventable. In the context of endemic enteric fever in India, vaccination of high-risk populations and healthcare workers is recommended. The conjugated typhoid vaccine (TCV) has now replaced the Vi polysaccharide vaccine in children under 2 years, offering longer-lasting protection.