Page 25 of 35
IM26.28-33 | Parasitic Infections: Amoebiasis, Malaria, Leishmaniasis, Filariasis, and Cysticercosis — SDL Guide
Learning Objectives
- Describe the pathogenesis, clinical features, diagnosis, and management of amoebiasis including intestinal and extraintestinal (hepatic) amoebiasis
- Describe the pathogenesis, clinical features (species-specific), diagnosis, and management of malaria caused by P. falciparum, P. vivax, P. malariae, and P. ovale, including severe malaria
- Describe the pathogenesis, clinical features, diagnosis, and management of leishmaniasis — kala-azar (visceral), cutaneous, and mucosal forms
- Describe the pathogenesis, clinical features, diagnosis, and management of filariasis including lymphatic filariasis (Wuchereria bancrofti) and tropical pulmonary eosinophilia
- Describe the pathogenesis, clinical features, diagnosis, and management of cysticercosis and neurocysticercosis
INSTRUCTIONS
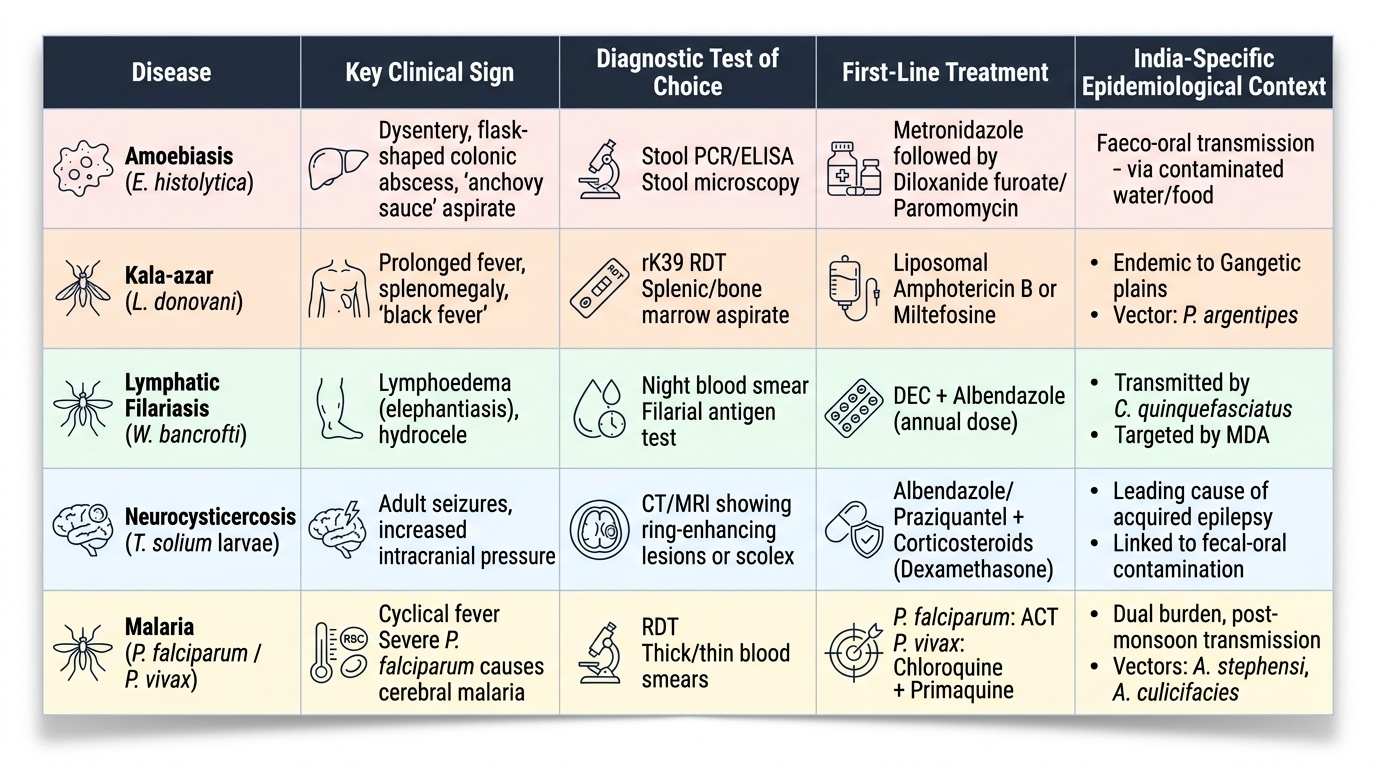
Parasitic infections remain a major public health and clinical challenge in India. This SDL covers the five most clinically important parasitic diseases in the Indian context, with emphasis on species-specific malaria treatment (the most examinable aspect of this topic), the distinction between intestinal and hepatic amoebiasis, and the diagnosis and treatment of kala-azar (now targeted for elimination in India). Malaria treatment has changed significantly with the shift to artemisinin-based combination therapy (ACT) as the first-line for all malaria in India since 2013 — know the current NVBDCP regimens. Neurocysticercosis is the most common cause of acquired epilepsy in adults in India.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 224 — Amoebiasis; Ch. 219 — Malaria; Ch. 222 — Leishmaniasis; Ch. 227 — Filariasis; Ch. 225 — Cysticercosis (textbook)
- API Textbook of Medicine, 10th ed., Section 7 — Infectious Diseases (Malaria, Kala-azar, Filariasis chapters) (textbook)
- NVBDCP Malaria Treatment Guidelines 2013 (updated); WHO Guidelines for Treatment of Malaria, 3rd ed. 2015; WHO Guidelines for Leishmaniasis (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Four clinical presentations arrive in a general medicine setting across different states of India. In Odisha: a 28-year-old tribal agricultural worker presents with 3 days of high fever with rigors, severe headache, and confusion — peripheral blood smear shows ring forms in red cells with multiple infections per RBC and occasional banana-shaped gametocytes. In Bihar: a 35-year-old farmer with 3 months of low-grade fever, progressive weight loss, massive splenomegaly, anaemia, and darkening of the skin. In Chennai during the monsoon: a 42-year-old fisherworker with 2 years of progressively swollen left leg that becomes hard and woody — he passes no visible filaria in his blood. In Delhi: a 30-year-old teacher with a first seizure and a CT brain showing a 1.5 cm cystic lesion with a central scolex in the right temporal lobe — he had been eating in roadside stalls that used improperly washed vegetables. These four patients represent the four major parasitic diseases of Indian internal medicine — falciparum malaria, kala-azar (visceral leishmaniasis), lymphatic filariasis, and neurocysticercosis — each requiring fundamentally different treatment, each with a clear epidemiological and geographical context, and each potentially fatal or permanently disabling without correct management. Recognising the disease from its ecological fingerprint — place, exposure, and time course — is the first clinical skill; selecting the correct treatment is the second.
WHY THIS MATTERS
Parasitic diseases collectively represent the most substantial infectious disease burden in India after respiratory infections. Malaria causes approximately 1–1.5 million cases annually in India (official notification; true burden estimated 3–10× higher), with Odisha, Jharkhand, Chhattisgarh, and Madhya Pradesh accounting for over 50% of falciparum malaria cases. Visceral leishmaniasis (kala-azar) is targeted for elimination in India (<1 case/10,000 population in endemic districts by 2025) but remains concentrated in Bihar, Jharkhand, and West Bengal, where it carries mortality of 90–100% if untreated. Lymphatic filariasis affects an estimated 40 million Indians with active infection, and chronic lymphoedema/elephantiasis disables millions more. Neurocysticercosis (Taenia solium larval infection of the brain) is the most common cause of adult-onset epilepsy in India, responsible for an estimated 30% of all new epilepsy in neurology departments. Amoebiasis (Entamoeba histolytica) is endemic throughout India, with amoebic liver abscess being one of the most common causes of liver abscess in tropical medicine. A physician practising in India will encounter all five diseases in regular clinical practice.
RECALL
Recall the essential parasitology. Plasmodium species are intracellular parasites of red blood cells; the four species infecting humans — P. falciparum, P. vivax, P. malariae, P. ovale — differ in erythrocyte tropism, periodicity of fever, ability to cause severe disease, and response to treatment. Entamoeba histolytica is the only pathogenic species of Entamoeba (distinguished from non-pathogenic E. dispar and E. moshkovskii only by antigen testing or PCR); it invades the colonic mucosa and can disseminate via the portal circulation to the liver. Leishmania species are obligate intracellular parasites of macrophages, transmitted by female sandfly (Phlebotomus in India) bites — the amastigote form survives and replicates within macrophage lysosomes. Wuchereria bancrofti is a filarial nematode transmitted by Culex quinquefasciatus in India; the adult worms live in lymphatics, causing lymphatic obstruction. Taenia solium (pork tapeworm) causes two distinct syndromes: intestinal taeniasis (adult worm in the gut, from eating undercooked pork) and cysticercosis (larval cysts in tissues, from ingestion of T. solium eggs from contaminated food or water — humans become the accidental intermediate host).
Malaria: Species-Specific Features, Severe Malaria, and Current Treatment
Malaria is caused by Plasmodium species transmitted by the bite of the female Anopheles mosquito. In India, P. falciparum and P. vivax account for virtually all cases (95%+); P. malariae and P. ovale are rare. P. falciparum is the most clinically dangerous — responsible for essentially all malaria deaths. Understanding the species-specific biology is essential for correct diagnosis, treatment selection, and prognostication.
Life cycle and fever periodicity: After the mosquito bite, sporozoites enter the liver (exo-erythrocytic stage), mature into merozoites, then enter red blood cells (erythrocytic stage). Merozoites rupture RBCs synchronously, releasing pyrogens — the classic febrile paroxysm (rigors → fever → sweating) follows the timing of RBC rupture: tertian fever (every 48 hours, days 1 and 3 = tertian, for P. vivax and P. falciparum) or quartan fever (every 72 hours, days 1 and 4, for P. malariae). In practice, especially with P. falciparum, daily fever without the classic periodicity is common — do not exclude falciparum malaria because fever is daily rather than tertian.
Species-distinguishing features:
| Feature | P. falciparum | P. vivax | P. malariae | P. ovale |
|---|---|---|---|---|
| RBC preference | All stages, predominantly young RBCs | Young, enlarged RBCs | Old RBCs | Old, oval RBCs |
| Merozoites/schizont | 8–24 | 12–24 | 6–12 | 6–12 |
| Smear appearance | Ring forms only (no mature trophozoites/schizonts in peripheral blood); banana-shaped gametocytes | Schüffner's dots; enlarged RBCs; banana-shaped? No — ameboid trophozoites; mature schizonts in peripheral blood | Rosette/daisy-head schizont; band-form trophozoites | Schüffner's dots; oval RBCs; fimbriated (James's dots) |
| Max parasitaemia | Up to 50% | <2% | <1% | <1% |
| Relapse (hypnozoites) | NO | YES (hypnozoites in liver) | NO (recrudescence, not relapse) | YES |
| Severe disease | YES (most severe) | Less common (severe vivax malaria does occur) | NO | NO |
| Fever periodicity | Daily or irregular (tertian in some) | Tertian (48h) | Quartan (72h) | Tertian (48h) |
Severe malaria (P. falciparum): P. falciparum-infected RBCs express PfEMP1 (P. falciparum erythrocyte membrane protein 1) on their surface, causing cytoadherence to vascular endothelium (including brain vasculature) and rosetting with uninfected RBCs. This microvascular obstruction + immune-mediated endothelial damage produces the multi-organ dysfunction of severe malaria. WHO criteria for severe falciparum malaria (any one feature):
- Cerebral malaria: altered consciousness, seizures, coma (GCS <11 in adults or Blantyre score ≤2 in children); pathognomonic: no other cause + P. falciparum positive
- Severe anaemia: Hb <7 g/dL + parasitaemia
- Respiratory distress / ARDS
- Hypoglycaemia (<2.2 mmol/L): particularly in children and pregnant women; also caused by quinine (stimulates insulin release)
- Acute kidney injury
- Abnormal bleeding / DIC
- Hyperparasitaemia (>5% parasitised RBCs)
- Circulatory collapse / algid malaria (shock)
- Haemoglobinuria / blackwater fever: massive intravascular haemolysis → haemoglobinuria (black/brown urine); associated with G6PD deficiency + quinine use (historically) or with severe falciparum malaria independently
Treatment of malaria — NVBDCP 2013 guidelines (India):
Uncomplicated P. falciparum:
- Artemisinin-based Combination Therapy (ACT) is now the mandatory first-line treatment in India for all P. falciparum.
- Artesunate + sulphadoxine-pyrimethamine (AS+SP): artesunate 4 mg/kg/day × 3 days PLUS SP single dose on day 1 — this is the WHO-recommended and NVBDCP-approved regimen for uncomplicated falciparum malaria in India.
- Artemether-lumefantrine (AL): alternative ACT; artemether 20 mg + lumefantrine 120 mg (6 doses over 3 days with fatty food for bioavailability).
- Primaquine 0.75 mg/kg as a single dose on day 2 — to kill gametocytes (reducing transmission); NOT for radical cure (falciparum has no liver hypnozoites). Check G6PD status — primaquine causes haemolysis in G6PD deficiency.
Uncomplicated P. vivax:
- Chloroquine remains first-line for P. vivax in India (total dose 25 mg/kg over 3 days: 10 mg/kg day 1, 10 mg/kg day 2, 5 mg/kg day 3) — resistance is low in India.
- Primaquine 0.25 mg/kg/day × 14 days for radical cure (eliminating liver hypnozoites to prevent relapse). G6PD testing is mandatory before primaquine — G6PD-deficient patients receive weekly primaquine 0.75 mg/kg × 8 weeks (safer schedule). Primaquine is contraindicated in pregnancy (use chloroquine suppression alone during pregnancy, then give primaquine post-delivery).
Severe malaria (any species): IV artesunate 2.4 mg/kg IV stat, then 2.4 mg/kg at 12h, then 2.4 mg/kg at 24h, then daily — superior to quinine in multiple trials; reduces mortality. Adjunct: parenteral dextrose (hypoglycaemia), antipyretics, blood transfusion (severe anaemia), dialysis (AKI), ICU (cerebral malaria, ARDS). Quinine is now reserved for areas/situations where IV artesunate is unavailable. Corticosteroids are CONTRAINDICATED in cerebral malaria (increase mortality — landmark trial).
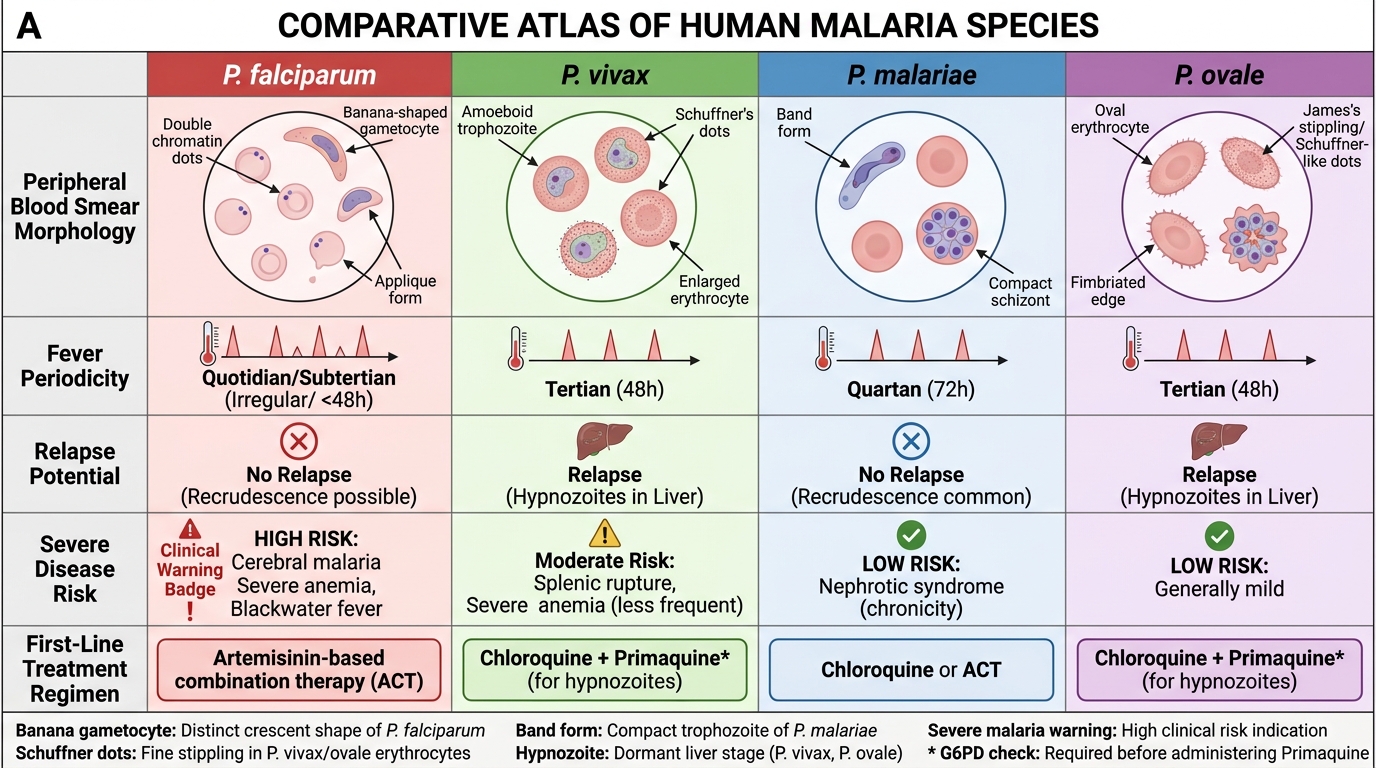
Malaria Species Comparison
Amoebiasis, Leishmaniasis, Filariasis, and Cysticercosis
Amoebiasis is caused by Entamoeba histolytica, a protozoan parasite that infects the large bowel and can disseminate to extraintestinal sites — principally the liver. India has one of the highest global burdens of amoebiasis; transmission is faeco-oral, through contaminated water and food. The distinction between non-pathogenic E. dispar (morphologically identical to E. histolytica on microscopy) and true pathogenic E. histolytica is clinically important: only E. histolytica requires treatment.
Provided image
Intestinal amoebiasis: E. histolytica trophozoites invade the colonic epithelium, producing characteristic flask-shaped ulcers (undermined at the base, with normal intervening mucosa — distinguishing amoebic colitis from the continuous mucosal involvement of IBD). Clinical spectrum: asymptomatic cyst passage (most common — no treatment needed) → mild diarrhoea → amoebic dysentery (acute onset of bloody diarrhoea, crampy abdominal pain, tenesmus; 10–20 loose stools per day, mixed blood and mucus; no fever or mild fever — unlike bacillary dysentery where fever is typically high); fulminant amoebic colitis (rare, <1% — extensive transmural necrosis, peritonitis, colonic perforation; mortality >40%).
Diagnosis: stool microscopy (trophozoites with engulfed RBCs = E. histolytica confirmed; cysts = Entamoeba sp., PCR or antigen test needed to distinguish E. histolytica from E. dispar); stool antigen test (ELISA) for E. histolytica — specific, detects active infection; serology (anti-amoebic antibodies) — more useful for amoebic liver abscess.
Treatment of intestinal amoebiasis: metronidazole 400–800 mg three times daily × 5–10 days (kills invasive trophozoites in tissue); always follow with luminal agent (diloxanide furoate 500 mg TDS × 10 days or paromomycin) to eradicate intestinal cysts (metronidazole alone leaves cysts in the gut, risking relapse).
Amoebic liver abscess (ALA): the most common extraintestinal manifestation — trophozoites travel via the portal vein to the liver, producing a liquefied cavity ('anchovy sauce' brown pus — due to liquefied hepatocytes, NOT pus with neutrophils). Usually single, in the right lobe. Clinical features: high fever, right hypochondrial pain (dull, aching), tender hepatomegaly; elevated ALP and transaminases; no jaundice usually (unless large abscess compresses bile duct). Importantly, only 10–15% of ALA patients have concurrent intestinal symptoms — the absence of diarrhoea does NOT exclude ALA. Diagnosis: ultrasound (hypoechoic cavity, right lobe); anti-amoebic serology (IgG antibody) — positive in >95% at presentation; stool examination often negative in ALA. Treatment: metronidazole 400–800 mg TDS × 10 days (first-line); aspiration is NOT routine — reserved for: very large abscess (>10 cm), left lobe ALA (risk of rupture into pericardium), failure to respond to metronidazole at 48–72 hours, or threatened rupture.
Visceral Leishmaniasis (Kala-azar): caused by Leishmania donovani in India (anthroponotic — humans are the only reservoir; transmitted by the female sandfly Phlebotomus argentipes). The parasite is an obligate intracellular parasite of macrophages, disseminating to the reticuloendothelial system (spleen, liver, bone marrow, lymph nodes). The visceral form is universally fatal if untreated.
Clinical features: insidious onset of prolonged fever (low-grade, irregular, often in spikes) + massive splenomegaly (the spleen can fill the entire abdomen — the most striking physical finding) + anaemia (from bone marrow infiltration and hypersplenism) + wasting and weight loss + darkening of the skin (hyperpigmentation — the name 'kala-azar' means 'black fever' in Hindi/Assamese, though this sign is less prominent than classical descriptions suggest). Hepatomegaly is present but less prominent than splenomegaly. Pancytopenia from bone marrow infiltration + hypersplenism. Hypergammaglobulinaemia (polyclonal IgG elevation) + hypoalbuminaemia.
Diagnosis: rK39 rapid diagnostic test (RDT) — dipstick test using recombinant Leishmania antigen; sensitivity 96–98% for Indian kala-azar; the preferred initial test in India for point-of-care diagnosis. Bone marrow/splenic aspirate — demonstration of amastigotes (Leishman-Donovan bodies within macrophages) is the gold standard; splenic aspirate has >95% sensitivity but carries risk of haemorrhage. Serology (DAT — Direct Agglutination Test): title ≥1:3200 = highly suggestive.
Treatment in India:
- Liposomal amphotericin B (L-AmB) is now the first-line treatment for kala-azar in India (under the national elimination programme): single-dose 10 mg/kg IV infusion; or 3-dose regimen 5 mg/kg on days 1, 3, and 5. Cure rate >95% with minimal toxicity compared to conventional AmB.
- Miltefosine (oral): 2.5 mg/kg/day × 28 days; the only oral drug for kala-azar; first-line in some WHO contexts; increasing resistance being reported in India (relapse rate rising).
- Meglumine antimoniate / sodium stibogluconate (pentavalent antimonials): previously first-line, now largely replaced due to high resistance in Bihar (>60%) and significant toxicity (cardiotoxicity, hepatotoxicity, pancreatitis); still used in some regions.
- PKDL (Post-Kala-azar Dermal Leishmaniasis): hypopigmented or nodular skin lesions appearing 6 months to 3 years after successful kala-azar treatment; a reservoir for transmission; treated with miltefosine × 12 weeks.
Lymphatic Filariasis: caused by Wuchereria bancrofti (transmitted by Culex quinquefasciatus mosquitoes in India); adult worms live in lymphatic vessels, causing lymphatic inflammation → obstruction → lymphoedema → elephantiasis (massive limb/genital swelling with skin thickening). Microfilariae are released into blood at night (nocturnal periodicity — blood sampling for microfilariae must be done at night, 10 PM–2 AM). Clinical stages: acute adenolymphangitis (fever + retrograde lymphangitis — distinctive: starts distally and moves proximally, unlike bacterial lymphangitis) → chronic lymphoedema → elephantiasis. Hydrocele in males is the most common chronic manifestation in endemic areas. Tropical Pulmonary Eosinophilia (TPE): a hyperimmune response to microfilariae trapped in pulmonary capillaries — presents with nocturnal cough, wheeze, bilateral infiltrates on CXR, and marked eosinophilia (>3,000/µL) + elevated IgE; microfilariae absent from peripheral blood (sequestered in lungs). Diagnosis: filarial serology (ELISA); ICT card test (rapid antigen test for W. bancrofti). Treatment: diethylcarbamazine (DEC) 6 mg/kg/day × 12 days (kills microfilariae and some adult worms); ivermectin (alternative or combination). For TPE: DEC 6 mg/kg/day × 21 days. For established elephantiasis: morbidity management (limb hygiene, compression, surgery for hydrocele).
Cysticercosis and Neurocysticercosis: caused by Taenia solium larval cysts (cysticerci) in tissues; the most common cause of acquired epilepsy in India. Humans become the intermediate host when they ingest T. solium eggs (not cysticerci) from food contaminated with infected human faeces (auto-infection or person-to-person transmission — NOT from eating pork). Cysts form in muscle, subcutaneous tissue, eyes, and CNS — the last being neurocysticercosis (NCC), the most dangerous form. Clinical features of NCC: new-onset seizures (most common; focal or generalised); raised intracranial pressure (obstructive hydrocephalus when cysts block CSF flow in the ventricles); cranial nerve palsies; focal deficits; spinal cord compression. Notably, many NCC cases are clinically silent until the cyst degenerates (triggers inflammatory response → perilesional oedema → seizures).
Diagnosis of NCC: CT/MRI brain — the imaging appearance varies by stage of cyst: (1) living cyst = well-defined hypodense cyst with a bright scolex (the 'dot-within-cyst' sign — pathognomonic); (2) degenerating cyst = ring-enhancing lesion with surrounding oedema (mimics TB tuberculoma or brain abscess); (3) calcified cyst = granular calcification. CT is the standard for NCC in India; MRI is superior for posterior fossa and spinal NCC.
Treatment of NCC: albendazole 15 mg/kg/day × 28 days (oral; with fatty food for absorption) with adjunct dexamethasone (4 mg TDS) during treatment to suppress the inflammatory oedema triggered by dying cysts. Praziquantel is an alternative cysticidal agent. Anti-epileptics are required for seizure control; choice and duration guided by CT findings. Contraindication: cysticidal drugs are CONTRAINDICATED in patients with large subarachnoid racemose cysticercosis (risk of triggering fatal cerebral oedema) or ocular NCC (risk of retinal detachment) — neurosurgical input required.
SELF-CHECK
A 22-year-old student from Bihar presents with 4 months of low-grade fever, progressive weight loss, and massive splenomegaly reaching the pelvis. Haemoglobin 7.2 g/dL, WBC 2,800/µL, platelets 68,000/µL. rK39 rapid diagnostic test: POSITIVE. He is started on treatment. What is the CURRENT FIRST-LINE treatment for visceral leishmaniasis (kala-azar) in India?
A. Sodium stibogluconate 20 mg/kg/day IM × 28 days — the first-line WHO antimonial regimen
B. Liposomal amphotericin B (L-AmB) — single dose 10 mg/kg IV, as recommended under the Indian national elimination programme
C. Miltefosine 2.5 mg/kg/day oral × 28 days — the only oral drug for kala-azar, now first-line in India
D. Conventional amphotericin B deoxycholate 0.75–1 mg/kg daily × 30 doses — the most cost-effective option
Reveal Answer
Answer: B. Liposomal amphotericin B (L-AmB) — single dose 10 mg/kg IV, as recommended under the Indian national elimination programme
In India under the national kala-azar elimination programme, liposomal amphotericin B (L-AmB) is the current first-line treatment — either as a single-dose 10 mg/kg IV infusion or as a 3-dose regimen (days 1, 3, 5), with cure rates >95% and minimal toxicity. Sodium stibogluconate (pentavalent antimonial) is no longer first-line in India because of >60% resistance in Bihar (the most heavily affected state) and significant cardiotoxicity and hepatotoxicity. Miltefosine is an important oral alternative, but increasing resistance is being reported in India and it is teratogenic (contraindicated in pregnancy). Conventional amphotericin B deoxycholate has been replaced by the liposomal formulation due to substantially lower nephrotoxicity.
SELF-CHECK
A 30-year-old woman from Odisha with no known medical history presents with 5 days of fever, rigors, and confusion. Peripheral blood smear: multiple ring forms per RBC, banana-shaped gametocytes. She is 12 weeks pregnant. The MOST appropriate treatment for severe falciparum malaria in pregnancy is:
A. Oral artemether-lumefantrine — the standard ACT for uncomplicated falciparum malaria, safe in all trimesters
B. IV quinine 10 mg salt/kg over 4 hours, every 8 hours — first-line for severe malaria in first-trimester pregnancy where IV artesunate data is limited
C. IV artesunate 2.4 mg/kg at 0, 12, 24 hours then daily — first-line for severe malaria in all patients including pregnant women in 2nd and 3rd trimester
D. Withhold treatment until delivery — antimalarials are teratogenic and delivery is preferable to drug exposure
Reveal Answer
Answer: C. IV artesunate 2.4 mg/kg at 0, 12, 24 hours then daily — first-line for severe malaria in all patients including pregnant women in 2nd and 3rd trimester
For severe malaria in pregnancy (2nd and 3rd trimester — as at 12 weeks, this is early 2nd trimester approaching: note 12 weeks is the end of 1st trimester), IV artesunate is the first-line treatment in all patients with severe malaria including pregnancy. The WHO 2015 guidelines support IV artesunate for severe malaria in all trimesters; the older preference for quinine in the first trimester was based on limited artesunate data, but recent evidence supports artesunate safety across all trimesters. The risk of untreated severe malaria to the mother and fetus (fetal loss >30%, maternal mortality) vastly outweighs any theoretical drug risk. Withholding treatment is never appropriate for severe malaria. Oral ACT is for uncomplicated malaria only — severe malaria requires parenteral treatment.
Diagnosis of Parasitic Infections: Laboratory and Imaging Approach
The diagnostic approach to parasitic infections requires integration of the epidemiological exposure, clinical syndrome, and targeted laboratory testing. Parasitological diagnosis has traditionally relied on microscopy — and for malaria especially, thick and thin blood smear examination remains a critical skill that every physician must be able to perform and interpret. However, rapid diagnostic tests (RDTs) and serological methods have transformed point-of-care diagnosis for several parasitic diseases. For each parasitic disease covered in this SDL, knowing the sensitivity, specificity, and practical constraints of each diagnostic method determines both the timeliness and accuracy of diagnosis. In high-burden settings like rural Bihar, Odisha, or Northeast India, the diagnostic choice must balance laboratory capability, specimen requirements, and turnaround time — a peripheral health centre blood smear or an rK39 strip test at the bedside may be the only feasible option, and the physician must know its value and limitations.
Malaria diagnosis — the most time-sensitive:
- Thick blood smear (TBS): the gold standard for malaria diagnosis; a large-volume blood film stained with Giemsa; allows detection of parasites at low parasitaemia (sensitivity threshold: ~5–10 parasites/µL); differentiates species by morphology. Mandatory skill for every physician working in endemic India.
- Thin blood smear (TBS): a monolayer film; better species identification (preserved RBC morphology); less sensitive than thick smear but essential for species-level identification and parasitaemia quantification.
- Rapid Diagnostic Test (RDT): detects P. falciparum HRP-2 antigen (or P. vivax pLDH) in blood; highly sensitive (~95%); results in 15 minutes; does not require microscopy expertise; widely deployed under the NVBDCP in peripheral health facilities. Limitation: HRP-2-deleted falciparum strains (pfhrp2 gene deletion) give false-negative HRP-2-based RDTs — an emerging resistance mechanism documented in India (Odisha).
- Haematological findings in malaria: anaemia (haemolytic), thrombocytopenia, leucocytosis (bacterial secondary infection) or leucopenia, elevated LDH and bilirubin (haemolysis).
Amoebiasis — diagnostic tests:
- Stool microscopy: trophozoites containing ingested RBCs = E. histolytica (pathognomonic of invasive disease); cysts seen on microscopy require antigen test/PCR to distinguish E. histolytica from non-pathogenic E. dispar.
- E. histolytica stool antigen ELISA: high sensitivity and specificity; differentiates pathogenic from non-pathogenic species.
- Ultrasound abdomen: for amoebic liver abscess — hypoechoic cavity typically in the right lobe; aspiration not routinely required but diagnostic if performed (anchovy sauce pus; trophozoites in wall biopsy, rarely in aspirate itself).
- Anti-amoebic serology (indirect haemagglutination test, ELISA): positive in >95% of ALA; useful when USS shows a liver abscess and stool examination is negative.
Leishmaniasis — diagnostic tests:
- rK39 RDT: dipstick immunochromatographic test; sensitivity 96–98% for visceral leishmaniasis in South Asia; the primary diagnostic tool in India for kala-azar.
- Bone marrow aspirate: demonstration of Leishman-Donovan bodies (amastigotes within macrophages) on Giemsa stain; 60–70% sensitivity.
- Splenic aspirate: >95% sensitivity; faster culture/microscopy; risk of haemorrhage in thrombocytopenic patients — only in experienced centres.
- Direct Agglutination Test (DAT): titre ≥1:3200 = positive; used as a confirmatory serological test.
Filariasis — diagnostic tests:
- Night blood smear (10 PM–2 AM): Giemsa-stained thick smear; demonstrates sheathed microfilariae of W. bancrofti (nocturnal periodicity); sensitivity higher at peak microfilaraemia.
- ICT card test (Immunochromatographic test): rapid antigen test for W. bancrofti filarial antigen; can be done at any time (not night-restricted); high sensitivity and specificity; used in WHO elimination programmes.
- Ultrasound of scrotal vessels: can visualise living adult worms as a wriggling, mobile structure in lymphatics — the filarial dance sign (pathognomonic when visualised).
Cysticercosis — diagnostic tests:
- CT brain (non-contrast): detects calcified granulomas (old cysts); contrast CT/MRI shows ring-enhancing lesions (degenerating cysts) or cystic lesions with scolex (active NCC).
- MRI brain: superior for posterior fossa, brainstem, and spinal cord NCC; better characterisation of cyst stage.
- Serology (EITB — Enzyme-linked Immunoelectrotransfer Blot): highly specific for NCC; sensitivity lower for single calcified lesions; useful when CT/MRI is equivocal.
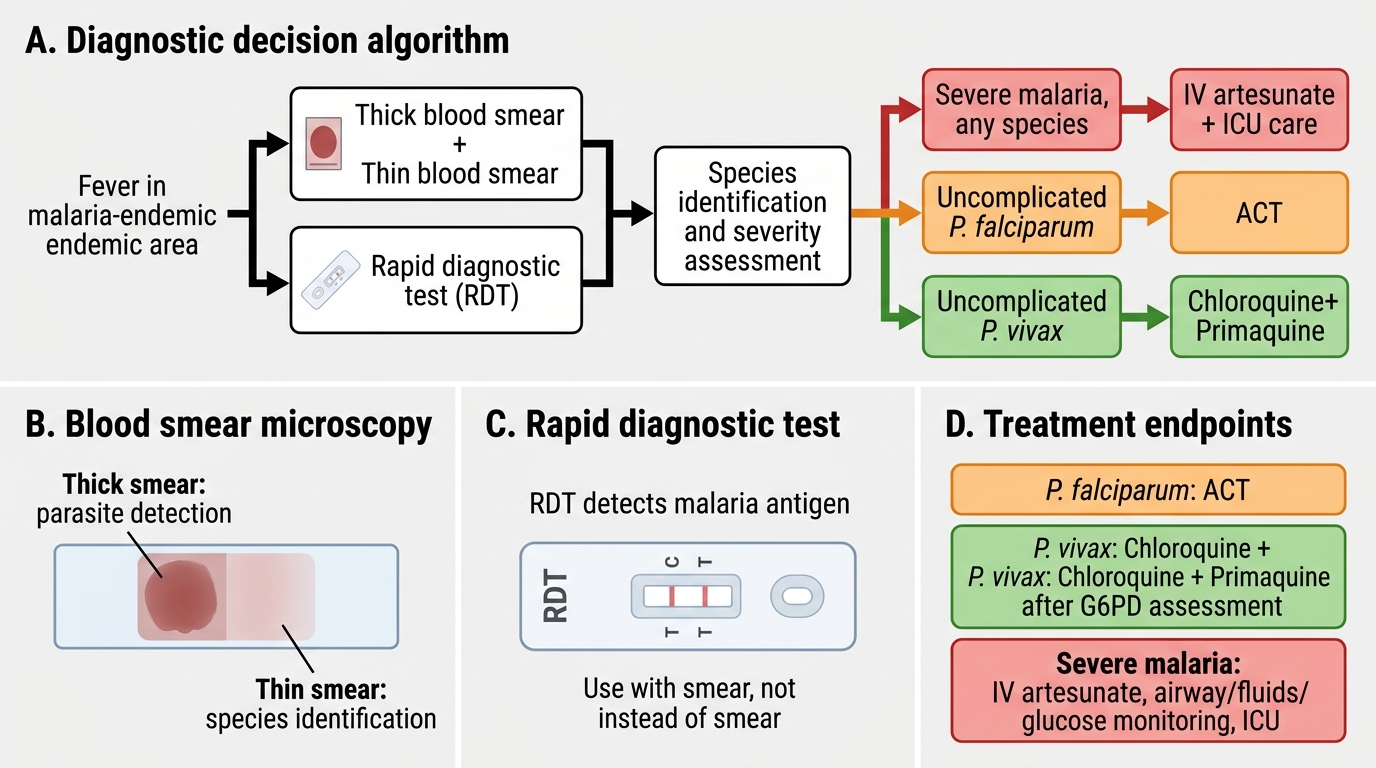
Malaria Diagnosis and Treatment Decision Algorithm