Page 26 of 35
IM26.28-33 | Parasitic Infections: Amoebiasis, Malaria, Leishmaniasis, Filariasis, and Cysticercosis — SDL Guide (Part 2)
Management of Parasitic Infections: Drug Regimens and Monitoring
The management of parasitic infections requires knowledge of the specific drug regimens for each disease, the key drug-specific precautions (G6PD deficiency and primaquine, pregnancy and antimonials, pregnancy and albendazole), and the clinical monitoring parameters that indicate treatment success or failure. These precautions are not merely academic — primaquine-induced haemolysis in a G6PD-deficient patient can be life-threatening, antimonial cardiotoxicity in kala-azar carries significant mortality, and albendazole-induced cerebral oedema in neurocysticercosis can be fatal without concurrent dexamethasone. Getting the drug choice and precautions right is the difference between a safe treatment course and a serious iatrogenic complication. The following table consolidates the treatment knowledge from this SDL into a practical bedside reference framework, followed by detailed discussion of the most important precautions.
Treatment regimens — consolidated:
| Parasitic infection | First-line treatment | Duration | Key precaution |
|---|---|---|---|
| Uncomplicated P. falciparum | Artesunate + SP (AS+SP) | 3 days (AS) + single-dose SP | G6PD check before primaquine single dose (gametocyte kill) |
| Uncomplicated P. vivax | Chloroquine + primaquine | CQ 3 days; primaquine 14 days | G6PD mandatory before primaquine; contraindicated in pregnancy |
| Severe malaria | IV artesunate | Until oral tolerated, then ACT | ICU management; hypoglycaemia monitoring; avoid steroids |
| Amoebic dysentery/ALA | Metronidazole 400–800 mg TDS | 5–10 days (dysentery); 10 days (ALA) | Always follow with luminal agent (diloxanide/paromomycin) |
| Kala-azar (India, 1st line) | Liposomal AmB (L-AmB) | Single dose 10 mg/kg IV | Monitor renal function; anaphylaxis risk (test dose) |
| Lymphatic filariasis | Diethylcarbamazine (DEC) 6 mg/kg/day | 12 days | Mazzotti reaction (exacerbation of systemic symptoms from dying microfilariae — manage with antihistamines, steroids for severe cases) |
| Tropical pulmonary eosinophilia | DEC 6 mg/kg/day | 21 days | Longer course than filariasis |
| Neurocysticercosis | Albendazole 15 mg/kg/day + dexamethasone | 28 days | Dexamethasone essential — dying cysts → cerebral oedema; contraindicated in ocular/subarachnoid racemose NCC |
Key drug-specific precautions:
Primaquine and G6PD deficiency: Primaquine is an 8-aminoquinoline that undergoes metabolic activation to reactive oxygen species — in G6PD-deficient red cells (lacking the enzyme to neutralise oxidative stress), this causes acute haemolytic anaemia. Severity depends on the degree of G6PD deficiency. Management: (a) Screen all patients with G6PD point-of-care test or quantitative assay before primaquine; (b) In G6PD-deficient patients with P. vivax, give weekly primaquine 0.75 mg/kg × 8 weeks (less oxidative stress per dose) with haemoglobin monitoring; (c) Pregnant women: defer primaquine until after delivery (G6PD status of fetus unknown). Primaquine is the ONLY drug that eliminates liver hypnozoites of P. vivax — without it, relapse (not recrudescence) will occur at 3-week to 12-month intervals.
Albendazole and pregnancy: Albendazole is teratogenic in animal studies — avoid in the first trimester; can be used with caution in 2nd and 3rd trimester when benefit outweighs risk. For NCC during pregnancy, the seizure management and corticosteroids are prioritised; cysticidal therapy timing is individualised.
Corticosteroids in NCC: Dexamethasone is given concurrently with albendazole to suppress the perilesional cerebral oedema triggered when cysts die. In patients with heavy NCC burden (multiple cysts) or intraventricular NCC, there is a risk of cerebral herniation from the inflammatory response — albendazole dose is sometimes reduced and steroids increased. The decision to treat with cysticidal drugs requires imaging characterisation of cyst stage, number, and location.
Follow-up and treatment response monitoring:
- Malaria: repeat smear at 48 and 72 hours after starting treatment — parasite clearance rate; if parasitaemia persists at 72 hours despite ACT, consider artemisinin partial resistance (emerging in Southeast Asia, now detected in some parts of India — Odisha/Northeast). Smear at day 28 to confirm sustained cure.
- Kala-azar: splenic/bone marrow aspirate or clinical assessment at 6 months to confirm cure; relapse occurs in 5–10% even after adequate L-AmB therapy (especially in patients with HIV co-infection — HIV-VL co-infection requires more prolonged treatment and secondary prophylaxis).
- NCC: CT/MRI brain at 6 months to document cyst resolution or calcification; seizure recurrence in first 6 months during treatment is expected (as cysts degenerate) and managed with anti-epileptics.
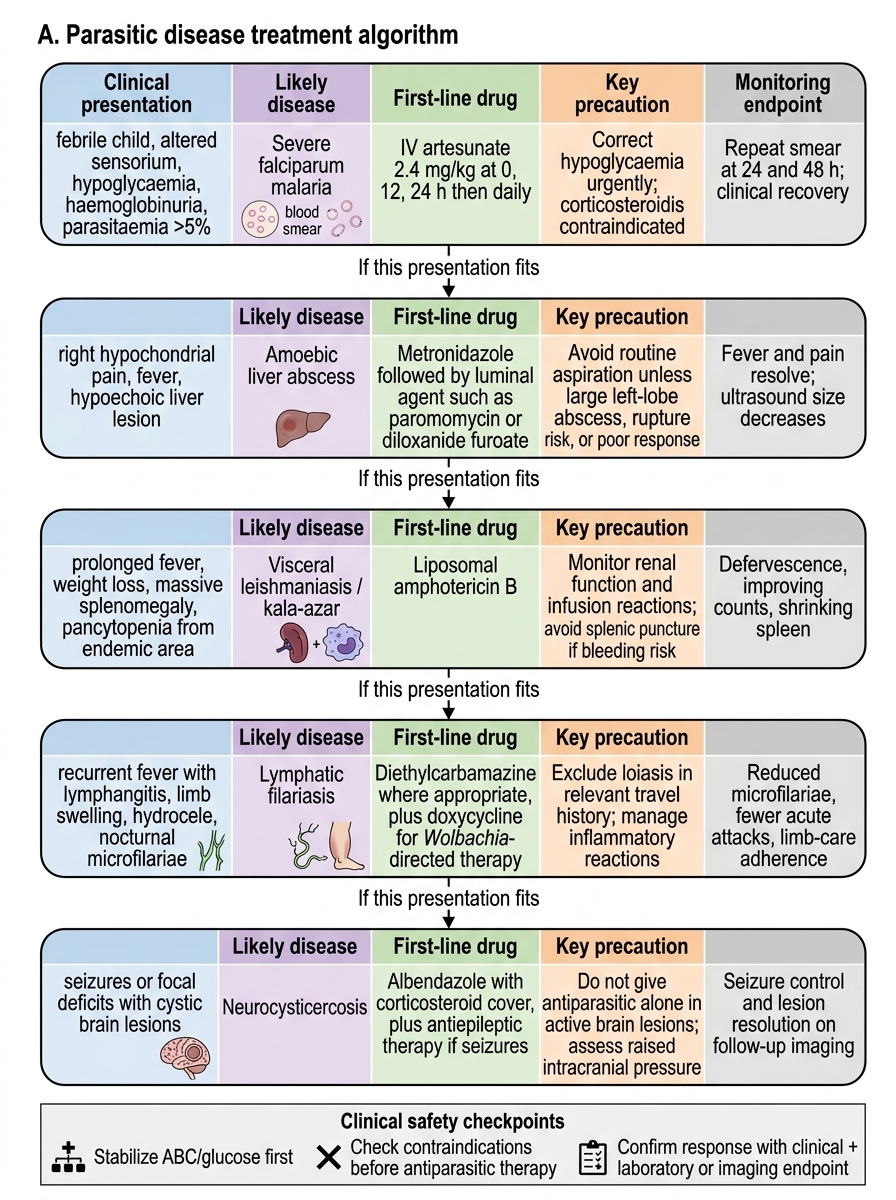
Parasitic Disease Treatment Algorithm
Self-Assessment: Parasitic Infections
You have now covered the five major parasitic diseases in this SDL. The following cases apply the diagnostic and management principles across these conditions. Work through each before reading the analysis.
Scenario A: A 5-year-old child from Jharkhand is brought with 8 days of fever, inability to stand, and passage of dark brown urine. Peripheral blood smear: multiple ring forms per RBC, parasitaemia 6%. Blood glucose: 1.8 mmol/L. He is semi-conscious (GCS 9).
Analysis: Multiple criteria for severe falciparum malaria are present simultaneously: cerebral malaria (GCS 9), hypoglycaemia (1.8 mmol/L), hyperparasitaemia (6%), and haemoglobinuria (dark urine = blackwater fever). Management: (1) IV artesunate 2.4 mg/kg immediately (stat dose); (2) IV 10% dextrose for hypoglycaemia — urgent, life-threatening; (3) ICU care — maintain airway, oxygen, IV fluids, temperature control; (4) Second dose artesunate at 12 hours, then 24 hours, then daily until oral tolerated. Corticosteroids are CONTRAINDICATED. Anti-epileptics for seizures if present. Repeat blood smear at 24 and 48 hours.
Scenario B: A 45-year-old returning from rural Tamil Nadu presents with right hypochondrial pain and fever. USS abdomen shows a 7 cm hypoechoic lesion in the right lobe of the liver. He denies diarrhoea. rK39 RDT for Leishmania: negative. Anti-amoebic serology (IHA): positive at 1:1024.
Analysis: Liver abscess + right lobe + no diarrhoea (present in only 10–15% of ALA) + positive anti-amoebic serology = amoebic liver abscess. The rK39 negative result correctly excludes kala-azar (and kala-azar does not cause liver abscesses as its main presentation). Start metronidazole 800 mg TDS × 10 days immediately; follow with luminal agent (diloxanide furoate 500 mg TDS × 10 days). Aspiration is NOT required for a 7 cm right lobe ALA in a stable patient — reserve for failure to respond at 48–72 hours, left lobe abscess, or signs of imminent rupture. Repeat USS at 10–14 days to confirm resolution.
Scenario C: A 28-year-old student from Bihar with no history of kala-azar presents with a 3-month history of multiple hypopigmented macular lesions on his face and trunk, some with nodular central areas. There is no ulceration. He is afebrile, with normal spleen. rK39 RDT: positive.
Analysis: This is Post-Kala-azar Dermal Leishmaniasis (PKDL) — hypopigmented macules and nodules appearing after kala-azar treatment (or even without a clear history in some cases). The positive rK39 confirms Leishmania infection. PKDL is an important public health issue as these patients are a major human reservoir for kala-azar transmission (high skin parasite density). Treatment: miltefosine 2.5 mg/kg/day × 12 weeks (longer course than for kala-azar itself). Important: this patient must be counselled about the public health implications of PKDL and the importance of completing the full 12-week course.
Scenario D: A 32-year-old construction worker from Uttar Pradesh presents with a first seizure (generalised tonic-clonic, 2 minutes). CT brain shows a single 1.2 cm ring-enhancing lesion in the right parietal region with perilesional oedema and a tiny central calcified focus (the scolex). There is no fever, no lymphadenopathy, no HIV risk factors.
Analysis: Single ring-enhancing lesion + scolex on CT + no fever + young adult from an endemic state = neurocysticercosis (single viable/degenerating cyst). The differential is tuberculoma (TB endemic in India), primary CNS tumour, or pyogenic abscess — but the imaging appearance with a visible scolex is highly specific for NCC. Start albendazole 15 mg/kg/day × 28 days + dexamethasone 4 mg TDS (to suppress perilesional oedema). Anti-epileptic drug (e.g., levetiracetam or carbamazepine) for seizure control. Advise driving restriction until seizure-free for 1 year (standard epilepsy driving rules). Follow-up CT at 6 months to confirm cyst resolution/calcification.
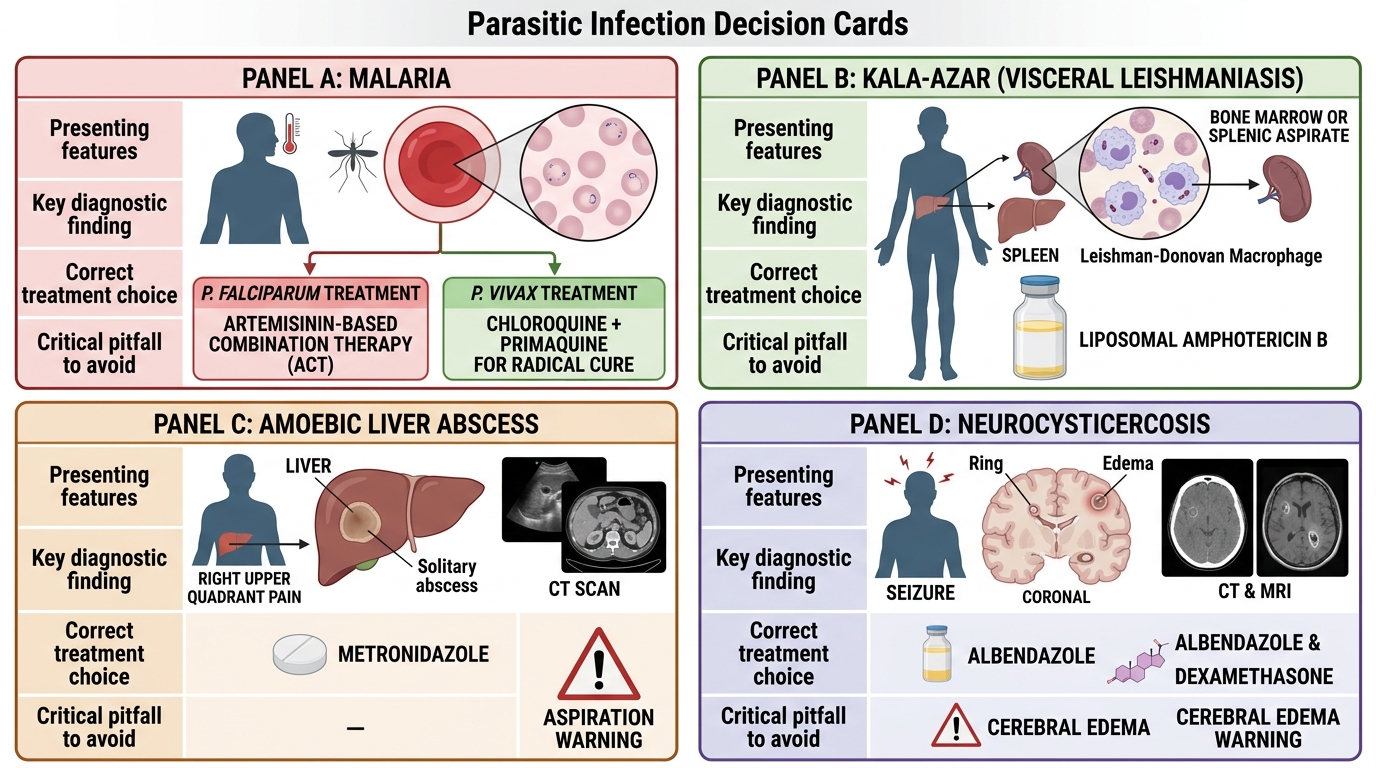
High-Yield Parasitic Infection Decision Cards
CLINICAL PEARL
Four high-yield clinical pearls for this SDL: (1) Malaria treatment India 2025: P. falciparum = ACT (artesunate + SP, or artemether-lumefantrine); P. vivax = chloroquine + primaquine 14 days. Severe malaria = IV artesunate FIRST-LINE, not quinine. Primaquine requires G6PD check FIRST. (2) Kala-azar first-line in India = liposomal amphotericin B (L-AmB), NOT antimonials (>60% resistance in Bihar). (3) Amoebic liver abscess: aspiration is NOT routine — reserve for large abscesses >10 cm, left lobe, failure of metronidazole at 48–72 hours. (4) Neurocysticercosis treatment: albendazole + dexamethasone concurrently — the steroid is NOT optional; dying cysts trigger perilesional cerebral oedema, and dexamethasone prevents seizure worsening during cysticidal therapy.