Page 8 of 18
IM27.{7,9-11} | Tuberculosis Diagnostic Testing — SDL Guide
Learning Objectives
- Interpret a Mantoux (TST/PPD) test result — technique, grading, thresholds, pitfalls including anergy and BCG effect
- Order and interpret diagnostic tests for presumptive TB including CBNAAT, sputum smear with AFB grading, culture and DST, CXR, pleural fluid analysis, and HIV serology
- Interpret a sputum AFB smear and antibiotic sensitivity test report, identifying species limitations and drug resistance implications
- Enumerate indications for CBNAAT, LPA, IGRA, special cultures, PCR, and anti-TB DST; explain why TB serology is not recommended
INSTRUCTIONS
This module covers the full diagnostic toolkit for tuberculosis — from the Mantoux test to CBNAAT, LPA, and pleural fluid ADA. Competencies IM27.7, IM27.9, IM27.10, and IM27.11 are all addressed. The central theme is that each test answers a specific clinical question; understanding what each test can and cannot tell you is the key to ordering investigations rationally. Pay particular attention to the NTEP shift to upfront CBNAAT as first-line testing, and the explicit rejection of serology.
References
- NTEP Technical and Operational Guidelines for Tuberculosis Control in India, 2016 (updated 2020) (guideline)
- Harrison's Principles of Internal Medicine, 21st ed. — Diagnosis of Tuberculosis (textbook)
- WHO Consolidated Guidelines on Tuberculosis — Module 3: Diagnosis, 2021 (guideline)
- API Textbook of Medicine, 10th ed. — Investigations in TB (textbook)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
The laboratory report in front of you reads: 'Sputum AFB smear: 1+ (5–9 AFB per 100 fields).' The patient is a 35-year-old man with six weeks of productive cough and weight loss. You could write the prescription immediately — but should you? Three questions matter urgently before you do: Is this M. tuberculosis or a non-tuberculous mycobacterium? Is this strain drug-sensitive or drug-resistant? And is this patient enrolled on the Nikshay portal, notified to NTEP, and assigned a treatment supporter? Each of these questions requires a different investigation. The sputum smear alone answers none of them. The diagnostic revolution in TB medicine over the past decade — driven by CBNAAT (Xpert MTB/RIF), line probe assays, and liquid culture systems — has transformed what is possible at the point of care. In the hands of a physician who knows what each test measures, what its limitations are, and when to order the next step, these tools can achieve a diagnosis and detect drug resistance within hours. In the hands of a physician who relies on the smear alone, they remain underused while the patient waits for a correct prescription.
WHY THIS MATTERS
The NMC competencies IM27.7 (interpret a Mantoux test — PPD), IM27.9 (order and interpret diagnostic tests based on clinical presentation, including CBC, CXR PA view, Mantoux, sputum smear, culture and sensitivity, pleural fluid examination, and HIV testing), IM27.10 (interpret a sputum gram stain and AFB with antibiotic sensitivity test from a given report), and IM27.11 (enumerate and describe indications for serology, special cultures, PCR, and anti-TB drug sensitivity testing) collectively cover the entire diagnostic toolkit for TB. These are assessed at the KH to KH/SH level, meaning you must be able to both describe the principles and apply them to clinical scenarios. In a country where TB diagnosis is the highest-volume infectious disease diagnostic workup performed — and where the gap between estimated and notified cases reflects diagnostic failures — mastery of this toolkit is not optional. The NTEP's shift to universal upfront CBNAAT means the diagnostic algorithm has changed; knowing the old thresholds without knowing the new ones will lead to ordering the wrong test at the wrong time.
RECALL
Before proceeding, activate your prior knowledge of the tests you already know. From microbiology: the Ziehl-Neelsen (ZN) stain exploits acid-fastness — mycobacteria retain carbol fuchsin after acid-alcohol decolourisation. You know that a sputum smear is a direct examination, not a culture; it cannot speciate the organism or test drug sensitivity. From immunology: the tuberculin skin test (TST/Mantoux) measures delayed-type hypersensitivity — it detects prior sensitisation to purified protein derivative (PPD) of M. tuberculosis, which reflects either past infection, active disease, or BCG vaccination. From basic molecular biology: polymerase chain reaction (PCR) amplifies specific DNA sequences — the Xpert MTB/RIF assay amplifies the M. tuberculosis-specific rpoB region and simultaneously probes for mutations conferring rifampicin resistance, all within two hours. From clinical medicine: a pleural effusion in TB is exudative — adenosine deaminase (ADA) is an enzyme produced by lymphocytes; elevated ADA (>40 IU/L) in pleural fluid reflects the intense lymphocytic response of TB pleuritis and is one of the most practically useful bedside markers for pleural TB in India.
Indications and Principles of Diagnostic Testing for TB
The clinical indication for TB diagnostic testing is any patient meeting the NTEP definition of presumptive TB: one or more of cough ≥2 weeks, fever ≥2 weeks, significant weight loss, or drenching night sweats in a high-burden country context. Additional indications include: household contact of a confirmed TB case, HIV-positive patient (at every clinic visit), patient with other high-risk comorbidities (diabetes, CKD, immunosuppressive therapy), or any patient with a radiological abnormality consistent with TB. The NTEP 2020 guidelines fundamentally changed the diagnostic entry point: whereas the previous RNTCP framework relied heavily on sputum smear microscopy as the first test, the NTEP now mandates CBNAAT (Xpert MTB/RIF) as the first-line diagnostic test for all presumptive TB cases wherever the facility is available (which now includes all designated microscopy centres under NTEP). This shift was driven by the superior sensitivity of CBNAAT over smear alone (approximately 90% vs 55–65% sensitivity for smear in all presumptive TB cases), its simultaneous detection of rifampicin resistance, and its rapid turnaround time of approximately 2 hours.
The governing principle of TB diagnostics is that each test in the hierarchy addresses a different clinical question. The diagnostic cascade should be thought of as a sequence of decisions, not a shotgun panel:
- Is TB present? — answered by CBNAAT/NAAT first; smear for rapid bacillary load assessment; culture (gold standard) for confirmation and drug sensitivity.
- Is the TB drug-sensitive or drug-resistant? — answered by CBNAAT (rifampicin resistance only), line probe assay (LPA — first-line and second-line DST), and phenotypic liquid/solid culture DST.
- What is the extent and form of disease? — answered by CXR (pulmonary TB), CT chest (complex disease), CSF analysis (CNS TB), pleural fluid examination (pleural TB), lymph node FNAC/biopsy (lymphadenitis).
- Are there comorbidities that modify management? — answered by HIV serology, fasting blood glucose/HbA1c, liver function tests (baseline before hepatotoxic ATT), renal function tests.
The ordering sequence matters: in a patient presenting with presumptive pulmonary TB, the correct sequence under NTEP is: CBNAAT (first) → if positive for MTB and rifampicin-susceptible, commence treatment and send for LPA → if negative by CBNAAT but high clinical suspicion persists, consider clinical diagnosis + CXR + culture. Do not default to sputum smear alone when CBNAAT is available; this is now a quality-of-care issue, not merely a guideline preference.
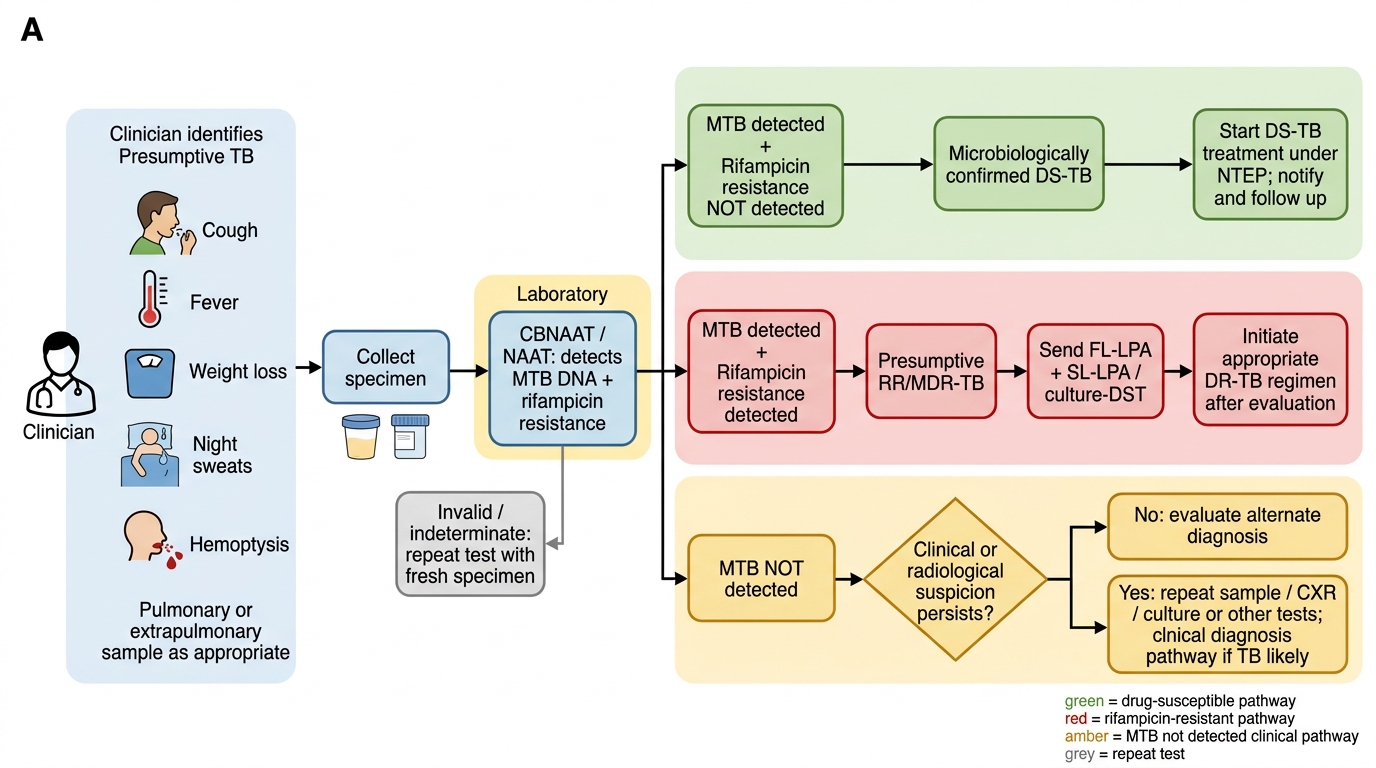
NTEP CBNAAT Diagnostic Algorithm for Tuberculosis
Tuberculin Skin Test (Mantoux/PPD) — Technique, Interpretation, and Pitfalls
The tuberculin skin test (TST), also called the Mantoux test or PPD test, remains a widely used tool for detecting prior sensitisation to M. tuberculosis in contact investigations, screening programmes, and high-risk population assessments. Despite the emergence of interferon-gamma release assays (IGRA), the TST is the predominant test used in India and most low- and middle-income countries, partly because of cost and availability. A thorough understanding of its principles, technique, reading, and interpretation — including its limitations — is essential for every physician.
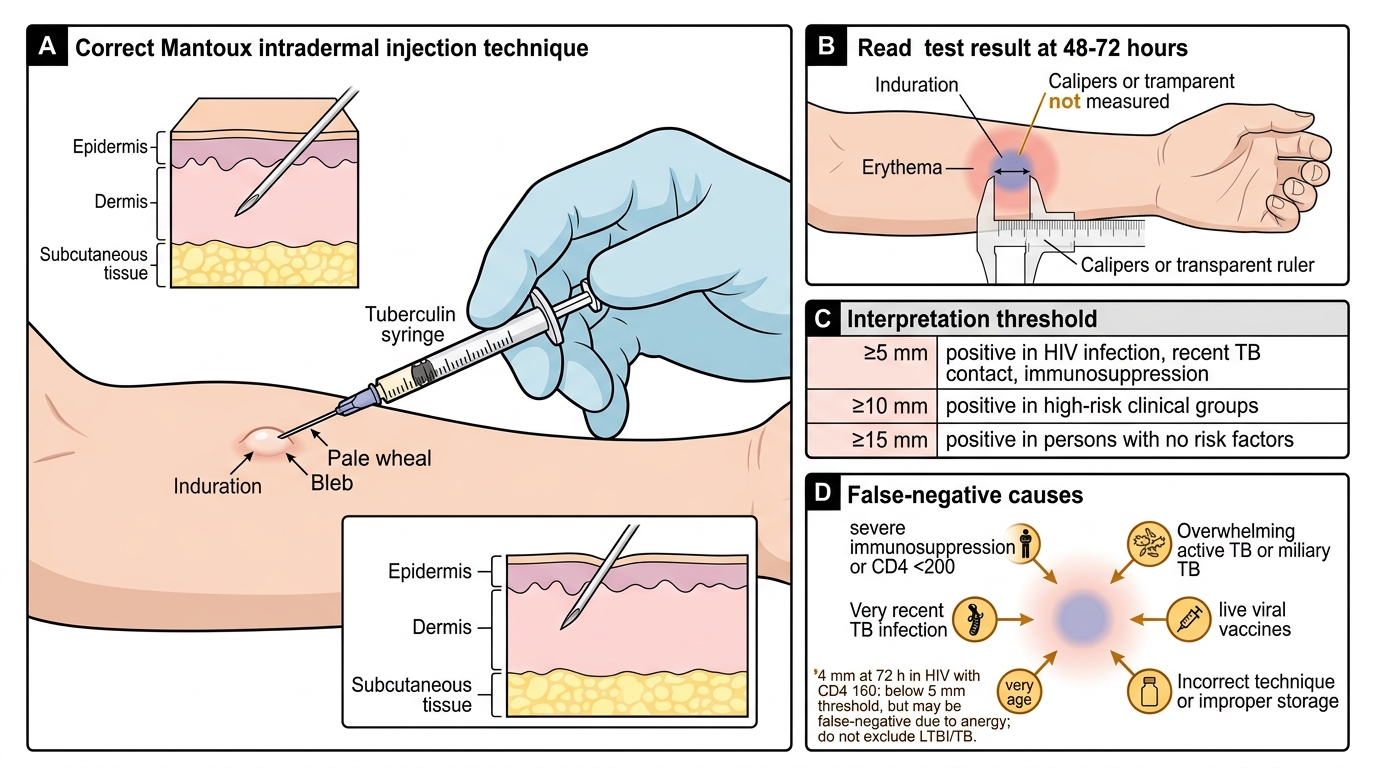
Principle: PPD (Purified Protein Derivative, standardised to 5 tuberculin units — 5 TU — for the standard Mantoux dose in India) is injected intradermally. In a sensitised individual (one who has been previously exposed to M. tuberculosis antigens — either through infection or BCG vaccination), memory CD4+ T lymphocytes recognise the tuberculin antigens and mount a type IV delayed hypersensitivity reaction: cytokine release causes local oedema and induration, peaking at 48–72 hours. The test is read by measuring the transverse diameter of the induration (not erythema) at 48–72 hours after injection.
Technique of administration:
- Site: Volar aspect of the forearm (anterior surface of the left forearm by convention), 4–6 cm below the antecubital fossa. Avoid areas with skin disease, prominent veins, or prior scars.
- Route: Strictly intradermal (not subcutaneous) — the needle (26–27 gauge) should be inserted bevel-up at a 5–15° angle; a correctly placed injection raises a pale bleb (raised wheal) of 6–10 mm immediately. If no bleb appears, the injection was subcutaneous — repeat at a different site.
- Volume: 0.1 mL (= 5 TU of PPD RT23 or equivalent), standardised by NTEP.
- Reading: At 48–72 hours (72 hours is standard in India), measure the diameter of induration using a ruler placed across the long axis of the arm. Measure induration only — erythema is irrelevant. Report in millimetres.
Interpretation thresholds:
The threshold for a positive TST is contextual — it varies by the probability of true infection, immunological status, and BCG vaccination history:
| Induration size | Context in which it is positive |
|---|---|
| ≥5 mm | HIV-positive; recent close contact of TB case; fibrotic changes on CXR consistent with prior TB; immunosuppressed (organ transplant, TNF-α blocker, high-dose corticosteroids) |
| ≥10 mm | High-risk groups in India (healthcare workers, recent immigrants from high-burden countries, children <5 years, DM, CKD, silicosis, malnourished) |
| ≥15 mm | Low-risk individuals with no known exposure (this threshold is rarely relevant in India given the high background prevalence) |
In India's NTEP guidelines, for contact investigation and LTBI assessment, ≥10 mm is the standard threshold for adults regardless of BCG status (acknowledging that BCG effect wanes significantly by adulthood and that the 10 mm threshold minimises false positives in the Indian context).
Critical limitations and pitfalls:
False-positive TST (TST positive but no TB infection):
- BCG vaccination — particularly within 5–10 years of vaccination, especially if given after infancy; BCG given at birth produces smaller and more transient reactions than later childhood vaccination. In India, BCG is given at birth and the TST reaction at adult age is usually less pronounced — most experts treat ≥10 mm in a vaccinated adult as a true positive in a high-burden setting.
- Non-tuberculous mycobacteria (NTM) — cross-reactive antigens in environmental NTM (particularly in humid tropical areas) can produce TST reactions, usually <10 mm.
False-negative TST (TST negative but true TB infection present):
- Anergy — the most clinically critical pitfall. Severe immunosuppression abolishes the delayed hypersensitivity response. A negative TST does NOT exclude active TB or LTBI in: HIV with CD4 <200 cells/μL (up to 50% false-negative rate), severe malnutrition, miliary TB (the disease itself overwhelms and exhausts the cellular immune response), infants <6 months, patients on high-dose corticosteroids.
- Very early infection — conversion takes 3–8 weeks after infection; TST may be negative in the window period.
- Technical error — subcutaneous injection, delayed reading, improper storage of tuberculin.
- Booster phenomenon — in elderly individuals with waned sensitisation, the first TST may be negative (loss of recall). A second TST 1–4 weeks later may become positive (the first test "boosted" the immune memory). This is not a true conversion (new infection) and can be misinterpreted.
The TST does NOT diagnose active TB — it detects sensitisation, which may reflect LTBI or past healed infection or BCG vaccination. Only bacteriological or molecular confirmation can diagnose active TB. The TST is a tool for LTBI detection and contact investigation, not a diagnostic test for active disease.
Mantoux Test: Technique, Reading, and Interpretation
SELF-CHECK
A 45-year-old HIV-positive patient (CD4 count 160 cells/μL) is a household contact of a smear-positive TB case. His Mantoux test shows 4 mm of induration at 72 hours. How should this result be interpreted?
A. Negative — no TB infection, no further action required
B. Indeterminate — repeat the test in 4 weeks
C. Possibly false-negative due to anergy; TST result should not be used to exclude LTBI in this patient
D. Positive — 4 mm exceeds the threshold for HIV-positive patients
Reveal Answer
Answer: C. Possibly false-negative due to anergy; TST result should not be used to exclude LTBI in this patient
In an HIV-positive patient with CD4 <200 cells/μL, the TST threshold for positivity is ≥5 mm — so 4 mm is technically below the threshold. However, the critical issue is that this patient cannot be reliably tested with TST because severe immunosuppression (CD4 <200) causes anergy — the T-cell memory response is inadequate to mount the delayed hypersensitivity reaction. A negative TST in this setting does NOT exclude LTBI or active TB. The correct clinical action is: (1) evaluate this patient for active TB clinically and radiologically regardless of TST result; (2) if active TB is excluded, offer TB preventive therapy (isoniazid-based TPT) based on the close household contact exposure and HIV status — not contingent on TST positivity. IGRA is also affected by severe immunosuppression, though generally less so than TST.
Sputum Smear Microscopy and AFB Reporting
Sputum smear microscopy for acid-fast bacilli (AFB) was the cornerstone of TB diagnosis for over a century and remains the most widely available rapid test in peripheral health centres. Despite being superseded as the first-line test by CBNAAT under the NTEP 2020 guidelines, proficiency in smear interpretation — reading, grading, and reporting — remains a mandatory clinical skill because smear results are still generated widely and must be correctly interpreted and communicated to clinical teams. The physician who cannot read an AFB grade or explain its meaning to a patient or junior colleague has an incomplete clinical skill set, regardless of how thoroughly CBNAAT is now used as the primary diagnostic platform. Furthermore, smear positivity grade carries independent information about bacillary burden that informs infectiousness assessment, treatment monitoring at 2 months (smear conversion is a key NTEP endpoint), and the urgency of isolation precautions. Understanding what the smear can and cannot tell you is therefore not historical knowledge — it is the interpretive framework that prevents both underuse and overinterpretation of this bedside test.
Sputum specimen collection — technique and quality:
The quality of sputum microscopy is determined primarily by specimen quality. A poorly collected specimen yields false-negative results. Correct technique:
- Collect early morning sputum (first expectoration on waking) — bacillary concentration is highest after overnight pooling of secretions.
- Instruct the patient to take a deep breath, hold for a moment, then cough deeply from the chest — not throat-clearing or salivation.
- Collect 3–5 mL of sputum into a wide-mouthed, screw-capped container. Mucoid or mucopurulent sputum is acceptable; watery saliva is unacceptable.
- A minimum of two specimens is recommended: early morning (collected at home) and spot (collected at the facility).
- Under NTEP: CBNAAT is now done on the first spot specimen; the second (early morning) is sent to microscopy if CBNAAT is negative but clinical suspicion remains.
ZN staining and reading:
The Ziehl-Neelsen (ZN) stain method: heat-fixed smear → carbol fuchsin (primary stain, heated) → acid-alcohol decolourisation → methylene blue counterstain. Result: AFB = bright red; background = blue. The Auramine-O fluorescent stain (same principle, but fluorescent dye) is more sensitive and faster for high-volume laboratories.
WHO/NTEP grading scale for AFB smear results:
The smear is reported quantitatively using the internationally standardised IUATLD scale:
| Result | Interpretation |
|---|---|
| No AFB seen (0) | Negative — no AFB in 100 fields |
| Scanty (1–9 AFB per 100 fields) | Positive — low bacillary load; report exact count |
| 1+ (10–99 AFB per 100 fields) | Positive — moderate bacillary load |
| 2+ (1–10 AFB per field in ≥50 fields) | Positive — high bacillary load |
| 3+ (>10 AFB per field in ≥20 fields) | Positive — very high bacillary load |
Higher smear grades correlate with: greater infectiousness, higher pre-treatment culture positivity, and (paradoxically) better initial smear-based treatment monitoring. A scanty positive requires the exact count (e.g., "3 AFB per 100 fields") to be reported.
Critical interpretive limitations of sputum smear:
- Cannot speciate: ZN stain identifies acid-fast bacilli generically. Non-tuberculous mycobacteria (NTM), M. leprae, Nocardia, and Actinomyces may also appear acid-fast. A positive smear does NOT confirm M. tuberculosis — it confirms acid-fast bacilli. Culture or CBNAAT is required for species identification.
- Sensitivity varies with disease form: Smear sensitivity is approximately 45–75% for pulmonary TB (higher for cavitary disease, lower for non-cavitary and smear-negative TB). Sensitivity for extrapulmonary TB is far lower — smear of CSF, pleural fluid, or urine is rarely positive.
- Cannot detect drug resistance: A smear-positive result gives no information about drug sensitivity. CBNAAT or DST is required.
- Requires adequate specimen: Saliva does not yield AFB; bronchial wash or BAL is used when spontaneous sputum is unproductive.
Interpreting a sputum culture and sensitivity (C&S) report:
If culture is performed (on LJ medium or liquid MGIT — mycobacteria growth indicator tube), a positive result takes 4–8 weeks on solid medium but 10–14 days on MGIT. The report includes: organism speciation (M. tuberculosis complex vs NTM), drug sensitivity testing (DST) results for first-line drugs (isoniazid, rifampicin, pyrazinamide, ethambutol, streptomycin). DST is reported as sensitive (S), intermediate (I), or resistant (R) for each drug. When reading a DST report: check the MIC (minimum inhibitory concentration) against published EUCAST/WHO breakpoints; resistance to isoniazid alone is concerning; resistance to rifampicin (alone or with isoniazid) = RR/MDR-TB → requires second-line DST before prescribing.
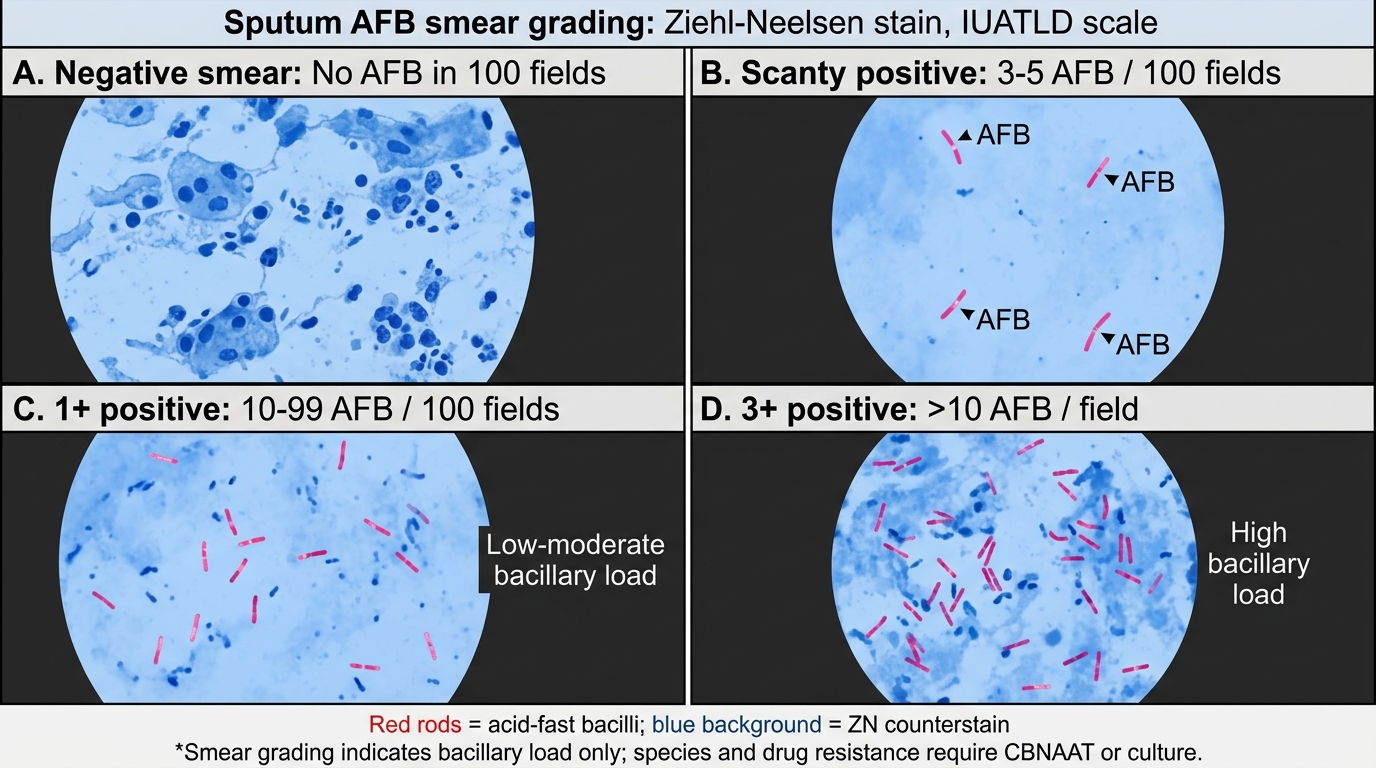
IUATLD Sputum AFB Smear Grading
SELF-CHECK
A sputum AFB smear report returns as 'Scanty (4 AFB per 100 fields).' Which of the following statements about this result is CORRECT?
A. This confirms active M. tuberculosis infection and drug-sensitive TB
B. This is a positive result indicating low bacillary load; species identity and drug sensitivity require CBNAAT or culture
C. A scanty result is a negative smear and requires no further action
D. This result means the patient is non-infectious
Reveal Answer
Answer: B. This is a positive result indicating low bacillary load; species identity and drug sensitivity require CBNAAT or culture
A scanty result (1–9 AFB per 100 fields) is classified as positive — acid-fast bacilli are present. The exact count (4 AFB per 100 fields) must be reported. However, a smear result tells you only that AFB are present — it cannot identify the species (M. tuberculosis vs NTM vs other), and it cannot test drug sensitivity. CBNAAT (Xpert MTB/RIF) or culture is essential for species confirmation and rifampicin resistance detection. A scanty positive patient with pulmonary TB symptoms should not be started on ATT without CBNAAT confirmation under NTEP guidelines, unless CBNAAT is unavailable and clinical judgment is applied. Infectiousness correlates with smear grade — scanty = low bacillary load, but the patient is still potentially infectious.