Page 9 of 18
IM27.{7,9-11} | Tuberculosis Diagnostic Testing — SDL Guide (Part 2)
CBNAAT, Molecular Tests, and Advanced Diagnostics — Indications and Interpretation
The development of rapid molecular diagnostics represents the most significant advance in TB diagnosis in the past three decades, transforming what was a multi-week diagnostic journey into a two-hour answer at the point of care. Understanding the indications, principles, and interpretive limits of CBNAAT, line probe assays (LPA), PCR-based platforms, and serology is now a core clinical competency for any physician treating TB in India. The shift to molecular diagnostics is not merely a technological upgrade — it is a patient-safety advance that prevents the single most dangerous diagnostic error in TB care: starting a drug-resistant TB patient on a drug-sensitive regimen. When a patient with undetected MDR-TB is treated with 2HRZE/4HRE, they receive effective monotherapy with the drugs to which their strain is sensitive while the resistant strains proliferate unchecked, generating an even more resistant bacterial population. Molecular diagnostics, used correctly and first, are the barrier against this cascade.
CBNAAT — Xpert MTB/RIF and Xpert MTB/RIF Ultra:
The Xpert MTB/RIF assay (manufactured by Cepheid; also marketed as CBNAAT — Cartridge-Based Nucleic Acid Amplification Test) is a fully automated, real-time PCR platform. A single cartridge containing the patient's unprocessed or minimally processed sputum (or other specimen) runs a complete DNA extraction, PCR amplification, and probe hybridisation cycle in approximately 90–120 minutes, with minimal operator input. The system simultaneously:
- Detects M. tuberculosis complex DNA (rpoB gene region — exclusive to MTBC, not NTM) — confirming TB vs non-TB.
- Probes five overlapping regions of rpoB for mutations conferring rifampicin resistance (>95% specificity for RIF resistance when the rpoB probe pattern matches known resistance mutations).
The result is reported as:
- MTB NOT DETECTED (negative) — with a semi-quantitative cycle threshold (Ct) value indicating specimen adequacy.
- MTB DETECTED + RIF SUSCEPTIBLE — proceed with DS-TB treatment (2HRZE/4HRE).
- MTB DETECTED + RIF RESISTANCE DETECTED — this is RR-TB/MDR-TB until proven otherwise; initiate second-line DST (LPA) before prescribing the MDR-TB regimen.
- MTB DETECTED + RIF INDETERMINATE — repeat the test; if still indeterminate, treat as RR-TB while awaiting culture DST.
Sensitivity and specificity: CBNAAT has approximately 88% sensitivity for smear-positive TB and approximately 67% for smear-negative TB (versus 45–60% for smear alone in the smear-negative group). Specificity is >98% for M. tuberculosis detection. The Ultra version (newer cartridge) has improved sensitivity for smear-negative and paucibacillary TB.
Specimens for CBNAAT: Sputum (standard); bronchial wash/BAL (for smear-negative with pulmonary infiltrates); CSF (for TB meningitis — sensitivity ~62%, but higher than smear); pleural fluid (lower sensitivity than other specimens — send pleural biopsy if possible); lymph node aspirate (FNAC material); urine (for renal TB); gastric aspirate (for young children who cannot expectorate).
Line Probe Assay (LPA — Hain MTBDRplus and MTBDRsl):
LPA is a PCR-based strip assay that detects resistance mutations simultaneously for multiple drugs. The two standard assays:
- MTBDRplus (first-line LPA): Detects mutations in rpoB (rifampicin resistance), katG and inhA (isoniazid resistance). Identifies whether INH resistance is high-level (katG) or low-level (inhA promoter) — clinically important because inhA mutants may retain susceptibility to higher-dose INH in some protocols.
- MTBDRsl (second-line LPA): Detects resistance to fluoroquinolones (gyrA/gyrB) and injectable agents (aminoglycosides — rrs gene; capreomycin — tlyA gene); used to diagnose pre-XDR and XDR-TB.
Indications for LPA: All RR-TB (RIF-resistant) patients detected by CBNAAT must have LPA performed to characterise full first- and second-line resistance pattern before prescribing the MDR-TB regimen; patients failing first-line treatment; re-treatment cases.
PCR-based culture confirmation and DST:
Beyond CBNAAT and LPA, phenotypic liquid culture (MGIT) with DST remains the reference standard for: cases with CBNAAT-negative but high clinical suspicion (grow organism to confirm), NTM identification (distinguishing M. tuberculosis from M. avium, M. kansasii etc.), comprehensive second-line DST for XDR-TB workup, and treatment-failure cases requiring full genotypic+phenotypic correlation.
Serology — the pitfall:
Commercially available TB serological tests (detecting antibodies to TB antigens) are explicitly NOT recommended by WHO and NTEP for TB diagnosis. These tests have unacceptably variable sensitivity (0–100%) and specificity (0–100%) across studies, are not standardised, and have led to overdiagnosis and unnecessary treatment in private-sector settings. The NTEP has banned TB serology kits from the programme. Any physician relying on a positive TB serology to make a diagnosis without microbiological or molecular confirmation is making an error.
Interferon-gamma release assays (IGRA — QuantiFERON-TB Gold, T-SPOT.TB):
IGRAs measure IFN-γ release by sensitised T lymphocytes in response to TB-specific antigens (ESAT-6 and CFP-10 — absent from BCG strains and most NTM). Advantages over TST: not affected by BCG vaccination (higher specificity in BCG-vaccinated populations); single blood draw (no need for return visit); slightly better specificity for M. tuberculosis infection. Disadvantages: expensive (not available in NTEP free-of-cost programme), affected by severe immunosuppression (CD4 <100), and like TST, cannot distinguish LTBI from active TB. IGRA is used in India primarily in the private sector for LTBI screening before immunosuppressive therapy and in BCG-vaccinated contacts where TST interpretation is ambiguous.
Special diagnostic tests for extrapulmonary TB:
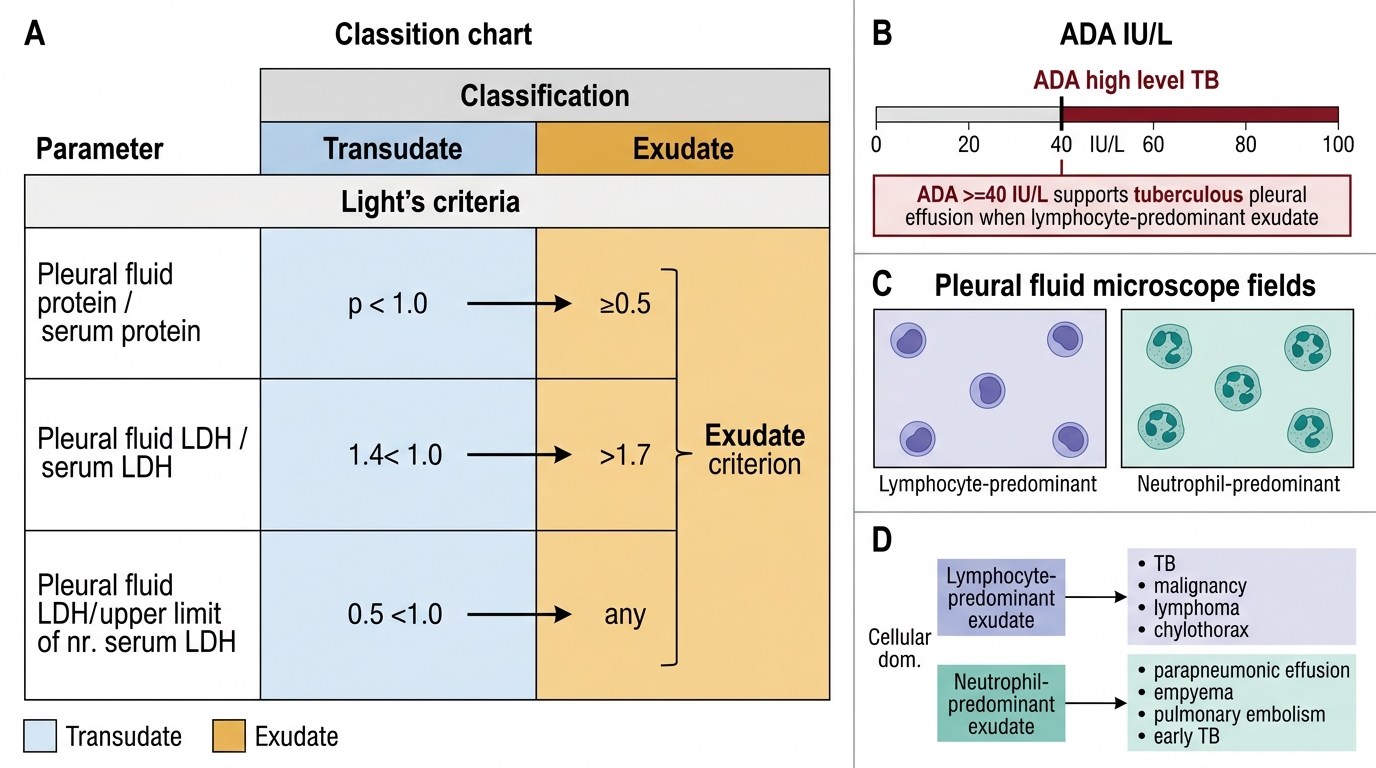
- Pleural fluid: LDH (>200 IU/L), protein (>30 g/L), pH (<7.3) — all confirm exudate. ADA (adenosine deaminase) >40 IU/L in pleural fluid has sensitivity ~92% and specificity ~90% for TB pleuritis in India and is the most practically useful bedside marker. Pleural fluid AFB smear sensitivity is <10%; culture is 25–55%. Pleural biopsy (by image-guided or thoracoscopic method) provides the highest yield for histological confirmation.
- CSF in TB meningitis: Appearance — clear/xanthochromic; cells — 50–500 lymphocytes/μL (early in meningitis may have PMN-predominance); protein — elevated (100–500 mg/dL); glucose — low (CSF:serum glucose ratio <0.5); AFB smear on CSF — low sensitivity (20–40%); ADA in CSF — raised in TB meningitis; CBNAAT on CSF — approximately 62% sensitivity (best rapid test for CSF TB).
- Lymph node FNAC: Smear for AFB + histology (caseating granuloma) is the standard diagnostic approach; sensitivity ~80% for TB lymphadenitis when both are performed.
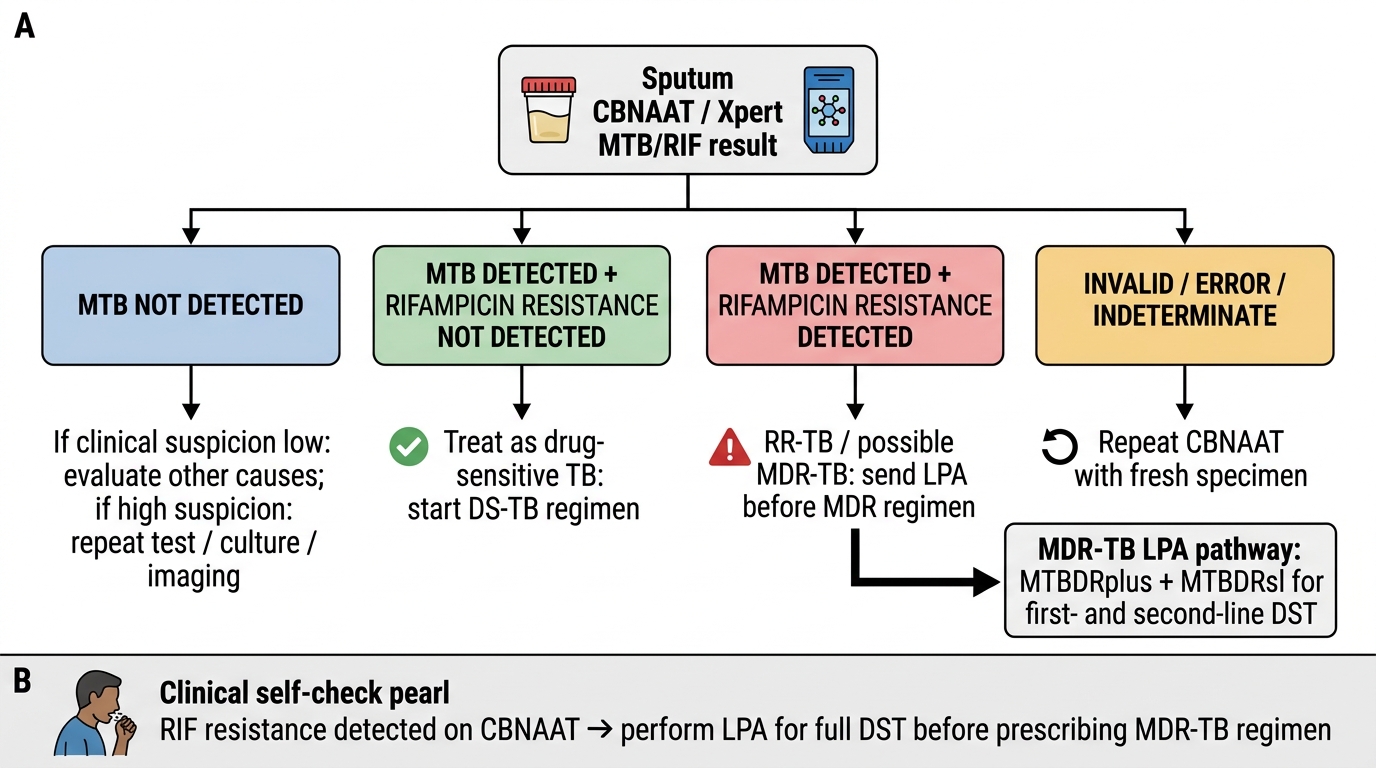
CBNAAT Interpretation Matrix for Tuberculosis
SELF-CHECK
A 40-year-old man with 8 weeks of cough, night sweats, and weight loss has a sputum CBNAAT result of 'MTB DETECTED — Rifampicin resistance DETECTED.' What is the SINGLE most important next investigation BEFORE prescribing the MDR-TB regimen?
A. Repeat sputum smear for AFB
B. Chest X-ray to confirm cavitation
C. Line probe assay (LPA — MTBDRplus and MTBDRsl) for full first- and second-line DST
D. Serum LDH and ESR
Reveal Answer
Answer: C. Line probe assay (LPA — MTBDRplus and MTBDRsl) for full first- and second-line DST
When CBNAAT detects rifampicin resistance, this indicates RR-TB/MDR-TB and mandates LPA testing before initiating the MDR-TB regimen. LPA (specifically MTBDRplus for first-line and MTBDRsl for second-line resistance) characterises the full drug resistance profile: is there also isoniazid resistance? Is it katG (high-level, must avoid INH in regimen) or inhA (low-level, INH may still be usable at high dose in some protocols)? Are there fluoroquinolone mutations that would indicate pre-XDR-TB? These results directly determine which second-line regimen to prescribe — prescribing the wrong MDR regimen without knowing the full resistance profile could result in virtual monotherapy on one or more drugs. Repeat smear and CXR do not determine drug resistance. Serum LDH and ESR are non-specific markers with no role in resistance characterisation.
Applied Practice — Ordering and Interpreting a Diagnostic Workup for TB
Clinical competence in TB diagnostics requires not just knowledge of individual tests but the ability to construct an appropriate, sequenced diagnostic plan for a real patient — selecting the right tests for the right specimen at the right time, and interpreting the results in the context of the clinical picture. The following framework describes how to build this plan systematically. A diagnostic workup is not a checklist that is applied identically to every patient; it is a tailored reasoning sequence that begins with the clinical scenario and ends with the information required to prescribe safely and monitor correctly. The physician who orders every possible TB test simultaneously wastes resources and generates conflicting results without a framework for resolution; the physician who orders too few tests risks missing drug resistance, missing extrapulmonary disease, or missing a comorbidity that modifies the treatment. The four-step framework below is applicable to any clinical scenario involving presumptive TB and provides a structured mental model that can be used at the bedside, in a referral letter, and in a case presentation.
Building the diagnostic workup — four-step framework:
Step 1 — Classify the clinical scenario:
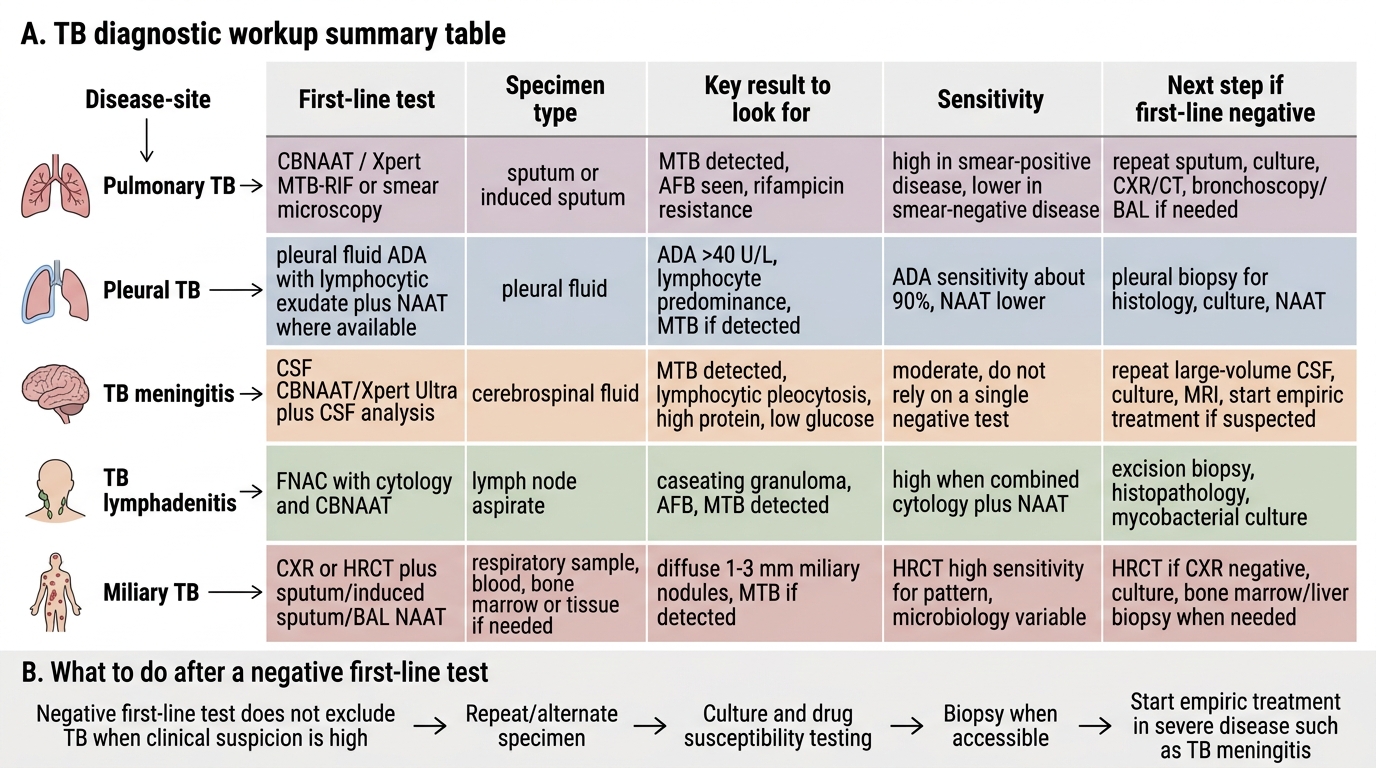
Is this presumptive pulmonary TB (cough + systemic symptoms)? Presumptive extrapulmonary TB (lymphadenopathy, back pain, meningism, pleural effusion, renal symptoms)? A contact investigation (exposure to known TB, asymptomatic)? Each scenario has a different entry point test.
Step 2 — Select the first-line test by scenario:
- Presumptive pulmonary TB: CBNAAT on two sputum specimens (spot + early morning) = first choice. If CBNAAT unavailable: two smear microscopy specimens + CXR, then escalate to CBNAAT.
- Smear-negative, CXR-suspicious TB (bilateral infiltrates, cavitation, hilar adenopathy): Bronchoscopy with BAL for CBNAAT + culture; consider empirical trial only if the above are negative with high clinical suspicion (supported by senior clinician).
- Pleural TB (unilateral effusion): Pleural fluid analysis (protein, LDH, cells, ADA); CBNAAT on pleural fluid (lower yield but specific); pleural biopsy if facilities available.
- TB meningitis: Urgent CSF examination (cell count, protein, glucose, ADA, AFB smear, CBNAAT).
- TB lymphadenitis: FNAC with AFB smear + cytology + culture; if FNAC inconclusive, core biopsy for histology.
- Miliary TB: CXR (millet-seed pattern), blood culture for MTB (BACTEC), urine AFB culture, CBNAAT on induced sputum, lumbar puncture if CNS involvement suspected; fundoscopy (choroidal tubercles).
- Contact investigation / LTBI screening: TST ± IGRA; if positive, CXR to exclude active disease; if CXR negative and active TB excluded, offer TPT.
Step 3 — Interpret results in context:
Never interpret a result in isolation. A negative CBNAAT does not exclude TB when clinical suspicion is high — proceed to culture and clinical assessment. A positive TST in an HIV-positive patient with CD4 <200 may be falsely negative; treat based on contact history. ADA >40 IU/L in pleural fluid strongly supports TB pleuritis even with negative fluid AFB smear.
Step 4 — Mandatory baseline tests before ATT commencement:
Before starting anti-TB treatment: complete blood count (anaemia, baseline WBC), liver function tests (ALT, AST, bilirubin — rifampicin, isoniazid, and pyrazinamide are all hepatotoxic; a baseline is essential for monitoring), serum creatinine (ethambutol and pyrazinamide renal clearance), HIV serology (if status unknown — mandatory under NTEP), fasting glucose or HbA1c (DM screening), visual acuity and colour vision baseline (ethambutol optic neuropathy monitoring), uric acid (pyrazinamide raises uric acid — relevant in patients with gout).
Case worked example:
Patient: 38-year-old male, 6-week cough, weight loss, evening fever. Known household contact of smear-positive pulmonary TB 3 months ago. CBNAAT result: MTB detected, RIF susceptible.
Interpretation: Active pulmonary TB, drug-sensitive. The CBNAAT confirms M. tuberculosis and confirms rifampicin susceptibility. A full LPA is not urgently needed (RIF susceptible) but should follow as per NTEP protocol.
Next steps: (1) Nikshay notification within 24 hours. (2) HIV serology, fasting glucose, LFTs, creatinine, visual acuity. (3) Commence 2HRZE/4HRE at appropriate weight-band FDC dose. (4) Assign treatment supporter. (5) Ni-kshay Poshan Yojana enrolment. (6) Contact-tracing for his household contacts (including all children <5 years who are priority contacts for TST and TPT).
TB Diagnostic Workup Summary
Self-Assessment: Interpreting TB Diagnostic Reports
The following scenarios test your ability to interpret TB diagnostic results and take the correct clinical action. For each, read the report data carefully before reading the analysis — the clinical reasoning sequence is the skill being assessed.
Scenario A — Mantoux interpretation in a contact:
A 6-year-old child, household contact of a father with smear-positive pulmonary TB, has a Mantoux test showing 12 mm of induration at 72 hours. She has no cough, fever, or weight loss. CXR is normal. How do you classify this result, and what is the correct action?
Analysis: In a child <5 years (or ≤15 years in a high-risk contact), a TST ≥10 mm is positive. At 12 mm with known close household contact to a smear-positive case, this is a positive TST indicating LTBI. The normal CXR and absent symptoms confirm no active disease. The correct action: offer TB preventive therapy (TPT) — 6 months of daily isoniazid (6H) — which reduces the lifetime risk of progression from LTBI to active TB by approximately 60–90% in children. Also: monitor with repeat TST in 6 months if the first test had been negative (two-step contact investigation).
Scenario B — Interpreting an AFB smear report:
Sputum smear report: 'ZN stain — 2+ (approximately 3 AFB per field in 60 fields observed).' The patient is a 32-year-old with 5-week cough and HIV (CD4 = 320). CBNAAT result is pending. What do you know from the smear result alone, and what must you wait for CBNAAT to tell you?
Analysis: The smear tells you: acid-fast bacilli are present in high load (2+), the patient is highly infectious, and empirical isolation precautions should be applied immediately. What the smear does NOT tell you: species (is this M. tuberculosis or an NTM?), drug sensitivity (no information about resistance). With an HIV-positive patient, NTM pulmonary disease is in the differential alongside pulmonary TB. CBNAAT will confirm: (a) MTB or not, and (b) RIF resistance status — both of which determine the treatment regimen. Do not start ATT without CBNAAT confirmation unless CBNAAT is unavailable and clinical urgency is extreme.
Scenario C — Pleural fluid interpretation:
Pleural fluid analysis report: protein 52 g/L, LDH 380 IU/L, glucose 2.8 mmol/L (serum glucose 5.1 mmol/L, ratio = 0.55), cells 650 cells/μL (90% lymphocytes), AFB smear negative, ADA 58 IU/L. How do you classify this effusion and what is the most likely diagnosis?
Analysis: This is an exudative effusion: protein >30 g/L (Light's criteria — also confirmed by high LDH). The cellular pattern is lymphocyte-predominant — consistent with TB, lymphoma, or malignancy. ADA of 58 IU/L is well above the >40 IU/L threshold for TB pleuritis (sensitivity ~92%, specificity ~90% in the Indian context). The combination of lymphocyte-predominant exudate + ADA >40 = TB pleuritis until proven otherwise. AFB smear negativity is expected (sensitivity <10% in pleural fluid) and does not refute the diagnosis. Correct action: start anti-TB treatment based on high-probability clinical + ADA diagnosis; send pleural fluid for CBNAAT; consider image-guided pleural biopsy if any atypical features or non-response to empirical ATT.
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
Pleural Fluid Interpretation in Suspected Tuberculous Effusion
CLINICAL PEARL
The most clinically important principle in TB diagnostics in modern India is this: CBNAAT is the first-line test, not a confirmatory test for smear-positive cases. Many physicians — trained in the RNTCP era — still order smear first and send for CBNAAT only if the smear is negative or if drug resistance is suspected. Under the current NTEP guidelines, CBNAAT should be the first test ordered for every presumptive TB patient, regardless of smear result. The reason is simple: CBNAAT simultaneously confirms M. tuberculosis (excluding NTM) and screens for rifampicin resistance — two pieces of information that fundamentally change management decisions and that smear cannot provide. A smear-positive patient with RIF resistance diagnosed only after 2 months of DS-TB treatment has been on virtual monotherapy for 8 weeks.
A second pearl: TB serology (antibody tests) is not recommended by WHO or NTEP and should never be used to diagnose TB. Commercial TB antibody kits are widely sold in India and frequently used in private practice. Their sensitivity and specificity are unacceptably variable. A positive TB serology without microbiological confirmation is not a TB diagnosis — it is an indication to perform CBNAAT or culture.