Page 1 of 18
IM27.{1-4,12} | Tuberculosis Foundations — SDL Guide
Learning Objectives
- Describe the epidemiology of tuberculosis and its socioeconomic impact on India, including NTEP goals and burden statistics
- Explain the microbiology of M. tuberculosis — acid-fastness, cell wall structure, growth characteristics, and mode of transmission
- Describe the pathogenesis and natural history of pulmonary and extrapulmonary TB, including granuloma formation and the role of cell-mediated immunity
- Discuss the impact of HIV co-infection, diabetes, and malnutrition on TB presentation, diagnosis, and management
- Explain the mechanisms and determinants of drug resistance in M. tuberculosis, including the classification MDR-TB, pre-XDR-TB, and XDR-TB
- Describe the BCG vaccine — origins, indications, technique, efficacy, and complications
INSTRUCTIONS
This module covers the foundational science of tuberculosis — the organism, its transmission, its immunological standoff with the host, its interaction with comorbidities, the mechanisms driving drug resistance, and the BCG vaccine. These concepts are the indispensable substrate for all subsequent clinical TB competencies: history-taking, examination, diagnostic testing, and prescribing. Master the granuloma, understand the mutation-based resistance mechanism, and learn the distinction between NTEP and the obsolete RNTCP. All five competencies (IM27.1–4 and IM27.12) are covered in this module.
References
- Harrison's Principles of Internal Medicine, 21st ed. — Tuberculosis and Other Mycobacterial Infections (textbook)
- API Textbook of Medicine, 10th ed. — Tuberculosis (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed. — Tuberculosis (textbook)
- WHO Global TB Report 2023 (guideline)
- NTEP Technical and Operational Guidelines for Tuberculosis Control in India, 2016 (updated 2020) (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
Ramesh is a 32-year-old construction worker from Bihar who has been coughing for eight weeks. He dismisses it as "dust from the site." His wife noticed he has been losing weight and sweating at night. His six-year-old daughter has started coughing too. At the NTEP microscopy centre, Ramesh's sputum is smear-positive for acid-fast bacilli. The diagnosis is pulmonary tuberculosis. The ripple is immediate and personal: a young breadwinner faces weeks off work, the family's nutrition and income threatened, and a young child now requires TB preventive therapy. Multiply Ramesh's story by 2.8 million — India's estimated annual TB incidence — and you begin to grasp why tuberculosis is not just a clinical diagnosis but a socioeconomic catastrophe. Understanding TB from first principles — the organism, its transmission, its evolution inside a human body, and the forces that drive drug resistance — is not optional knowledge for the Indian physician: it is the foundation of every prescribing decision, every contact-tracing conversation, and every contribution to the national goal of TB elimination by 2025.
WHY THIS MATTERS
India carries the highest tuberculosis burden in the world, accounting for approximately 26% of global TB cases according to the WHO Global TB Report 2023. TB is simultaneously the leading infectious cause of death in India and one of the chief drivers of household poverty, lost productivity, and catastrophic health expenditure. For the NMC IM27 competency cluster, you are expected to describe and discuss TB epidemiology, microbiology, transmission, pathogenesis, drug resistance, and the BCG vaccine at the KH (Knowledge applied in clinical scenarios) level. These competencies underpin every subsequent clinical skill — history-taking, clinical examination, investigation ordering, and prescribing — for all forms of TB. They are also the knowledge base required for rational participation in the National Tuberculosis Elimination Programme (NTEP), India's primary public health response to this epidemic. Without these foundations, the anti-TB regimen is memorised rather than understood, and the rational basis for choosing between drug-sensitive and drug-resistant treatment protocols is lost.
RECALL
Before proceeding, activate your prior knowledge of mycobacteria and the immune system. Mycobacterium tuberculosis belongs to the order Actinomycetales, characterised by a waxy, lipid-rich cell wall containing mycolic acids — the basis of acid-fastness. You studied the Ziehl-Neelsen (ZN) stain in microbiology: the cell wall resists decolourisation with acid-alcohol, which is why TB bacilli stain bright red against a blue background. From immunology, recall the T-helper 1 (Th1) response: macrophages engulf TB bacilli but cannot kill them efficiently; CD4+ T cells release interferon-gamma (IFN-γ) and tumour necrosis factor-alpha (TNF-α) to activate macrophages for intracellular killing. The hallmark immunological structure — the granuloma — is a tightly organised aggregate of activated macrophages and epithelioid cells surrounded by lymphocytes, the body's attempt to contain bacilli it cannot destroy. Central caseous necrosis (cheese-like coagulative necrosis) is characteristic of TB and distinguishes it from the non-caseating granulomas of sarcoidosis. These building blocks — acid-fast organism, cell-mediated immunity, granuloma — are the armature on which this SDL builds.
Epidemiology of Tuberculosis and Its Impact on India
Tuberculosis (TB) remains the most consequential infectious disease by mortality burden in India, even after decades of national programme intervention. Understanding its epidemiology is clinically essential: it determines pre-test probability in every suspected case, shapes contact-tracing obligations, and contextualises drug-resistance patterns encountered at the bedside.
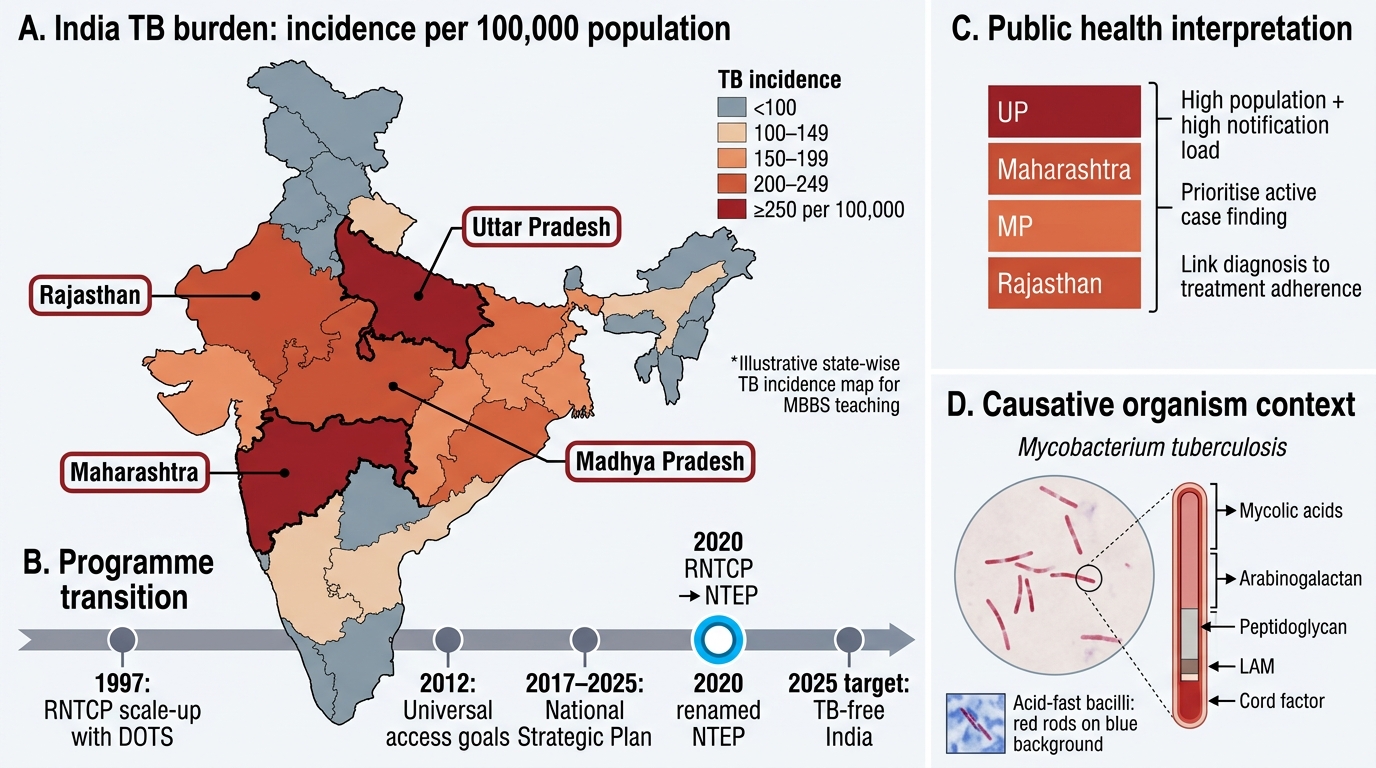
India is classified as a high-burden country under the WHO End TB Strategy. According to the WHO Global TB Report 2023, India has an estimated 2.8 million new TB cases per year, representing approximately 26% of the global burden. The incidence rate is approximately 199 per 100,000 population, though estimates carry uncertainty due to significant under-notification. The mortality from TB in India is approximately 3.5 lakh deaths per year, inclusive of TB-HIV deaths. This places TB above most non-communicable diseases in terms of years of life lost in working-age adults. In absolute numbers, India has more TB deaths annually than all road traffic accidents combined.
The demographic and social pattern is deeply informative for clinical practice. TB disproportionately affects men aged 15–49 years — the economically productive age group — because of greater occupational exposure, higher rates of smoking and alcohol use (both immunosuppressive), and patterns of male migration. Urban slums, overcrowded prisons, tea estates, brick kilns, and stone-quarrying communities carry far higher burdens than the general population. A patient's occupation, dwelling density, and recent migration history are therefore not social niceties in the TB history — they are direct epidemiological risk-stratification data. The household contact attack rate for smear-positive pulmonary TB is approximately 5–10%, meaning roughly 1 in 10 household contacts of an untreated smear-positive case will develop TB in their lifetime.
Economic impact extends beyond the individual: the cost of a TB episode to a household — including direct medical costs, transport to health facilities, and lost wages — frequently exceeds 20% of household annual income, meeting the WHO threshold for catastrophic costs. This financial toxicity explains delayed care-seeking (when working is economically existential), non-adherence to prolonged treatment, and the catastrophic poverty-TB cycle in which TB deepens poverty and poverty in turn amplifies TB transmission.
The NTEP (National Tuberculosis Elimination Programme) — formerly the Revised National Tuberculosis Control Programme (RNTCP), renamed in 2020 to reflect the national goal of eliminating TB by 2025 (incidence <1/million population) and ending it by 2030 — is the government infrastructure through which TB care is delivered. Key NTEP features include: universal access to free diagnosis and treatment, Nikshay (the national digital TB notification and patient management portal), Ni-kshay Poshan Yojana (nutritional support of ₹500/month to all TB patients during treatment), and integration of private-sector TB notifications. As of 2022, approximately 2.4 million TB patients were notified under NTEP, but the gap between estimated and notified cases remains a programme priority.
India TB Burden and RNTCP to NTEP Transition
Microbiology of Mycobacterium tuberculosis
Mycobacterium tuberculosis is an obligate aerobic, non-spore-forming, non-motile, rod-shaped bacillus. It belongs to the Mycobacterium tuberculosis complex (MTBC), which includes M. tuberculosis (human TB, by far the predominant cause), M. bovis (bovine TB, acquired through unpasteurised milk), M. africanum, M. microti, and M. canetti — all of which cause human TB albeit with different epidemiological patterns. In India, M. tuberculosis is responsible for more than 99% of human TB.
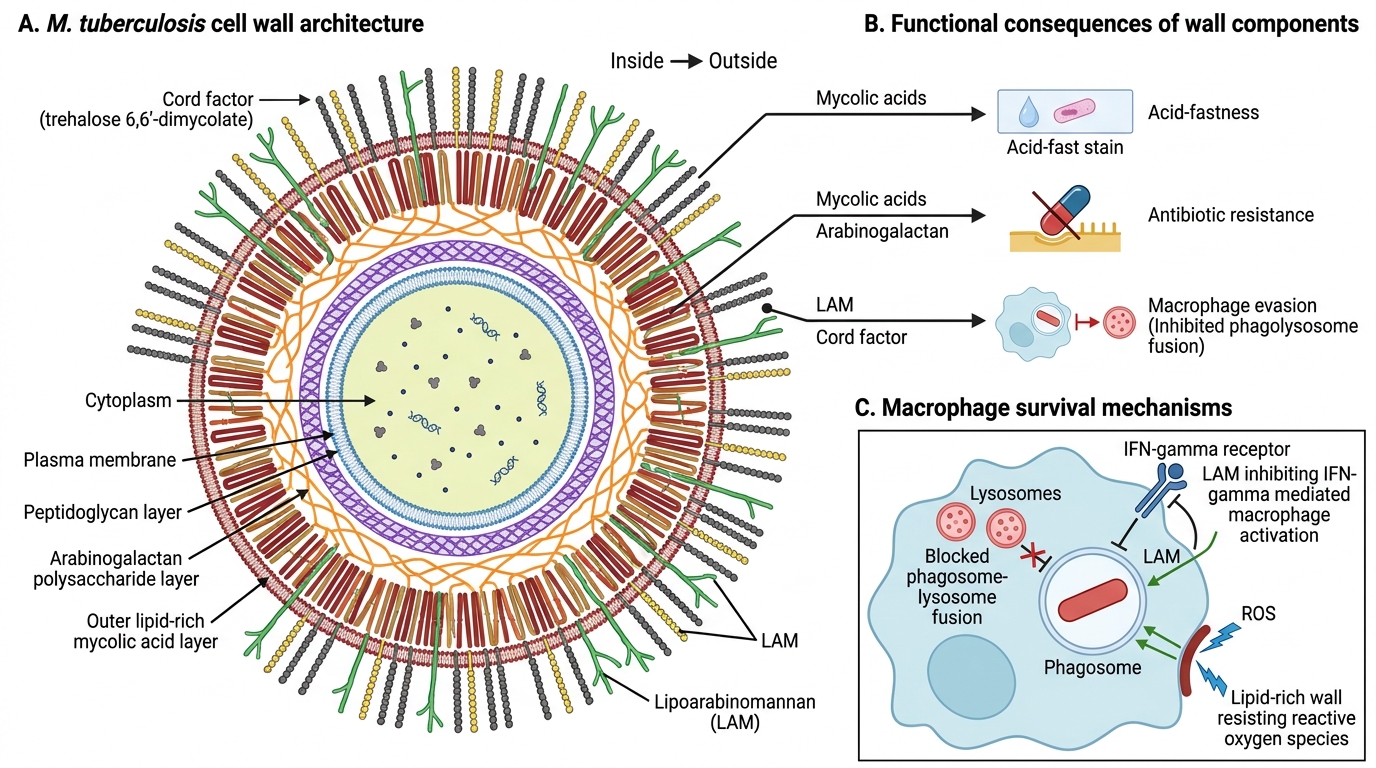
The hallmark microbiological property is acid-fastness — the inability to be decolourised by acid-alcohol after primary staining with carbol fuchsin. This property arises from the extraordinarily thick, lipid-rich cell wall composed of several unique components: mycolic acids (very-long-chain fatty acids, C60–C90), arabinogalactan (a complex polysaccharide linking mycolic acids to the peptidoglycan layer), lipoarabinomannan (LAM) (a surface glycolipid with potent immunomodulatory properties — it inhibits macrophage activation and interferon-gamma signalling), and various surface lipids such as cord factor (trehalose dimycolate) — responsible for the serpentine cording pattern seen on culture — and sulpholipids. These wall components collectively explain TB's exceptional chronicity: they resist digestion by macrophage lysosomes, insulate the bacillus from many antibiotics (contributing to intrinsic resistance to many commonly used drugs), and create the immunological milieu for granuloma formation.
Growth characteristics: M. tuberculosis is a slow-growing organism with a doubling time of approximately 18–24 hours (compare with E. coli at 20 minutes). This slow growth has profound clinical implications: clinical disease evolves over weeks to months, laboratory culture takes 4–8 weeks on solid Lowenstein-Jensen (LJ) medium, and anti-TB drug regimens must be maintained for months to kill both rapidly dividing extracellular bacilli and slowly dividing intracellular and dormant populations. On LJ medium, colonies appear as buff-coloured, rough, raised, warty colonies (described as "breadcrumb-like").
Mode of transmission: TB is almost exclusively transmitted by airborne inhalation of droplet nuclei — tiny particles (1–5 μm) containing 1–3 bacilli that remain suspended in air for hours and penetrate to the alveoli when inhaled. Droplet nuclei are generated by smear-positive pulmonary TB cases when they cough, sneeze, speak, sing, or spit. A single untreated smear-positive patient in a closed, poorly ventilated room can expose dozens of contacts. Sputum smear-negative but culture-positive cases are infectious but approximately 10-fold less so than smear-positive cases. Extrapulmonary TB (lymph nodes, bone, kidney, meningitis) is generally not directly transmissible unless there is a respiratory component (laryngeal TB, miliary TB with pulmonary lesions). Non-respiratory routes (unpasteurised milk → bovine TB; inoculation via skin/mucosa; vertical transmission) are rare but recognisable.
Niacin test and nitrate reductase test traditionally distinguished M. tuberculosis from other mycobacteria: M. tuberculosis is niacin-positive and nitrate-positive. These biochemical tests have been largely superseded by molecular methods in modern laboratory practice.
M. tuberculosis Cell Wall and Virulence Functions
Pathogenesis and Natural History of Tuberculosis
The pathogenesis of tuberculosis is the story of a prolonged stand-off between a pathogen that has evolved exquisite mechanisms to persist within macrophages and an adaptive immune system that contains but rarely eliminates the organism. Understanding this immunological dynamic is essential to understanding every clinical manifestation of TB — why primary infection is usually silent, why reactivation occurs decades later, why children and immunocompromised patients are at greater risk, and why TB can affect virtually any organ.
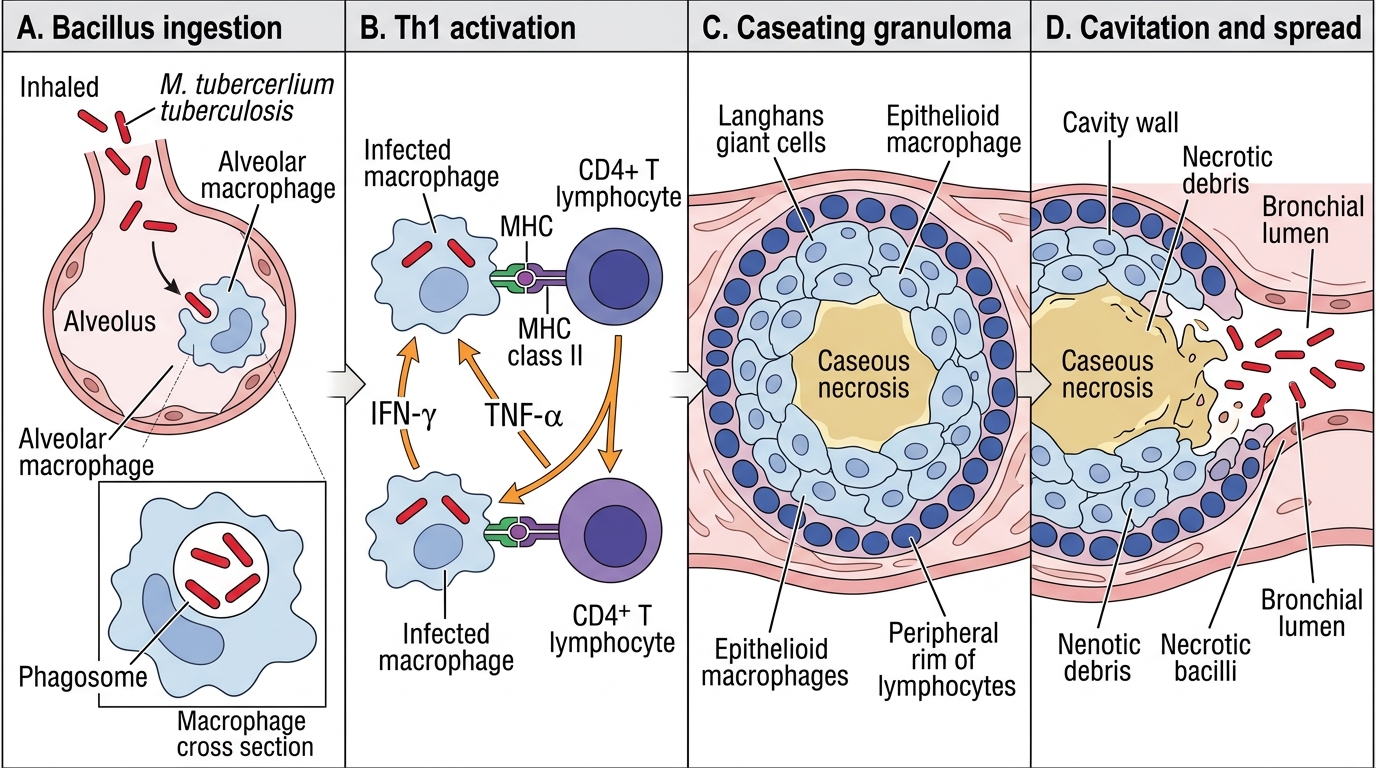
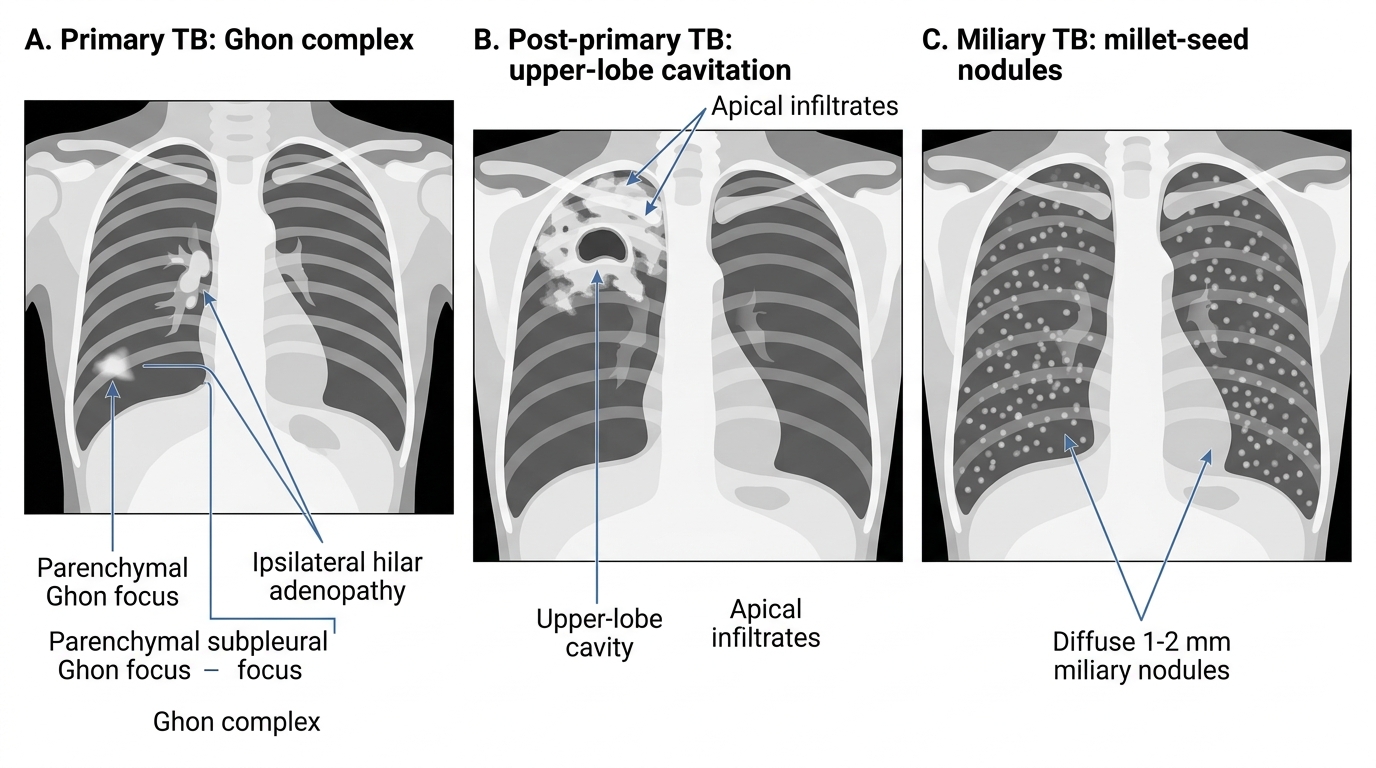
Stage 1 — Inhalation and initial alveolar response: Droplet nuclei carrying 1–3 bacilli are inhaled and deposited in the alveoli of the middle and lower lung zones (where airflow and therefore deposition are highest). Alveolar macrophages engulf the bacilli via surface receptors including the mannose receptor and complement receptors. M. tuberculosis evades intracellular killing through several mechanisms: it blocks phagosome-lysosome fusion (preventing exposure to lysosomal enzymes), resists reactive oxygen species via its lipid-rich wall, and uses LAM to inhibit macrophage activation by IFN-γ. During this initial phase (the first 1–3 weeks), bacilli multiply unchecked within macrophages, which carry them via lymphatics to regional hilar lymph nodes — forming the Ghon focus (primary lung lesion) and the primary (Ghon) complex (Ghon focus + ipsilateral hilar lymphadenopathy).
Stage 2 — Cell-mediated immunity activation (3–8 weeks): Macrophages that have engulfed TB bacilli present mycobacterial antigens via MHC class II molecules to CD4+ T lymphocytes in regional lymph nodes. Activated Th1 cells produce interferon-gamma (IFN-γ), which dramatically upregulates macrophage killing capacity. The adaptive immune response arrives at the site of infection and organises macrophages into the granuloma: a central zone of infected macrophages and epithelioid cells (fused macrophages), surrounded by a cuff of CD4+ and CD8+ T lymphocytes and a rim of fibrous tissue. The centre of the granuloma undergoes caseous necrosis — a solid, cheese-like material composed of dead macrophages, necrotic debris, and small numbers of bacilli that survive in this hypoxic, acidic environment. Tuberculin skin test (TST) and IGRA convert at this stage (3–8 weeks after infection), marking the onset of acquired immunity.
In 90–95% of immunocompetent adults, the granuloma successfully contains the infection. The Ghon focus heals with fibrosis and may calcify (the Ranke complex). This asymptomatic state is called latent TB infection (LTBI): no disease, positive TST/IGRA, viable dormant bacilli within granulomas. The lifetime risk of reactivation from LTBI is approximately 5–10% in immunocompetent adults, concentrated in the first 2 years after infection.
Stage 3 — Progressive primary TB or reactivation TB: In a minority — the immunocompromised, the malnourished, young children, those with comorbidities — the primary infection progresses without adequate containment. The granuloma liquefies, bacilli are released into airways (the origin of infectious sputum), and cavitation develops in the upper lobes (where oxygen tension is highest, favouring aerobic growth). Reactivation TB years or decades later follows the same pathology: an aged granuloma breaks down due to waning immunity, bacilli proliferate, and the upper-lobe cavitary disease we recognise as "typical" pulmonary TB appears.
Clinical natural history of pulmonary TB: The classic presentation — persistent productive cough (≥2–3 weeks), haemoptysis, fever (especially evening pyrexia), drenching night sweats, and significant weight loss — reflects weeks to months of untreated bacillary multiplication and systemic inflammation. Untreated smear-positive TB has a 5-year fatality rate of approximately 50%.
Extrapulmonary TB: M. tuberculosis can disseminate haematogenously from the primary focus to virtually any site. The most common extrapulmonary forms in India are:
- TB lymphadenitis (most common EPTB overall): cervical nodes are most affected; nodes mat together, become fluctuant, form cold abscesses (without warmth or redness), and may discharge chronically. Diagnosis: fine-needle aspiration cytology (FNAC) showing caseating granuloma + AFB smear/culture.
- Skeletal TB (Pott's disease): haematogenous seeding of the thoracolumbar vertebrae (D10–L2 most common); disc space loss precedes vertebral collapse; the hallmark complication is Pott's paraplegia from cord compression by caseous material or gibbus deformity. On X-ray: disc space narrowing with adjacent end-plate destruction and a paraspinal cold abscess (fusiform paravertebral shadow).
- CNS TB (tuberculous meningitis and tuberculoma): TB meningitis presents with subacute onset of fever, headache, meningism, and cranial nerve palsies; CSF shows elevated protein, low glucose, lymphocytic pleocytosis; adenosine deaminase (ADA) is elevated. Hydrocephalus and vasculitic strokes are feared complications.
- Miliary TB: haematogenous dissemination producing the classic chest X-ray of uniform 1–2 mm nodules throughout both lung fields (resembling millet seeds), often with simultaneous organ involvement (liver, spleen, bone marrow, meninges). Miliary TB can occur in primary TB (young children, severe immunosuppression) or as a complication of reactivation.
- Other sites: pleural TB (most common cause of exudative unilateral pleural effusion in India — raised ADA >40 IU/L in pleural fluid is highly sensitive), renal TB (sterile pyuria — white cells without bacteria on routine culture), pericardial TB, adrenal TB (rare cause of Addison disease).
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Tuberculosis Granuloma Formation and Cavitation
Chest X-ray Patterns of Pulmonary Tuberculosis
SELF-CHECK
A 35-year-old man is found to be TST-positive (18 mm) during a routine contact investigation after his colleague was diagnosed with smear-positive pulmonary TB. His chest X-ray is normal and he has no symptoms. What is the correct interpretation of this finding?
A. He has active pulmonary TB and requires immediate treatment
B. He has latent TB infection (LTBI) — acquired immunity without active disease
C. The positive TST indicates BCG vaccination effect only
D. He requires a CT chest to confirm the diagnosis before any action
Reveal Answer
Answer: B. He has latent TB infection (LTBI) — acquired immunity without active disease
A positive TST in an asymptomatic individual with a normal chest X-ray and a clear epidemiological exposure represents latent TB infection (LTBI) — the state of immune sensitisation without clinical disease, resulting from earlier infection with M. tuberculosis. In an adult with documented recent contact (high-risk exposure within 2 years), this is the most clinically significant finding. BCG effect is a consideration for interpretation, but in a 35-year-old Indian adult the BCG wanes and the TST threshold for significant reaction remains 10 mm or greater in high-burden settings; an 18 mm reading with a known smear-positive contact is highly likely to represent true infection. CT chest is not the next step — the clinical decision is whether to offer TB preventive therapy (TPT) under NTEP guidelines, not to escalate imaging.