Page 2 of 18
IM27.{1-4,12} | Tuberculosis Foundations — SDL Guide (Part 2)
Impact of HIV Co-infection and Comorbidities on TB
The interaction between tuberculosis and other medical conditions — particularly HIV/AIDS, diabetes mellitus, malnutrition, chronic kidney disease (CKD), and use of immunosuppressive therapy — profoundly modifies the natural history, clinical presentation, diagnostic yield, and treatment of TB. The Indian physician must be alert to these interactions because India carries a dual burden of TB and HIV, the world's largest burden of diabetes, and widespread undernutrition. Understanding how each comorbidity alters the clinical picture is not supplementary knowledge — it determines whether the clinician will recognise an atypical presentation and order the correct tests, or will miss a life-threatening diagnosis in a patient who cannot mount the classic immune response. The most important interaction, both globally and in India, is the synergy between HIV and TB, which has driven devastating mortality in sub-Saharan Africa and remains a significant cause of AIDS-related deaths in India's NACO programme data.
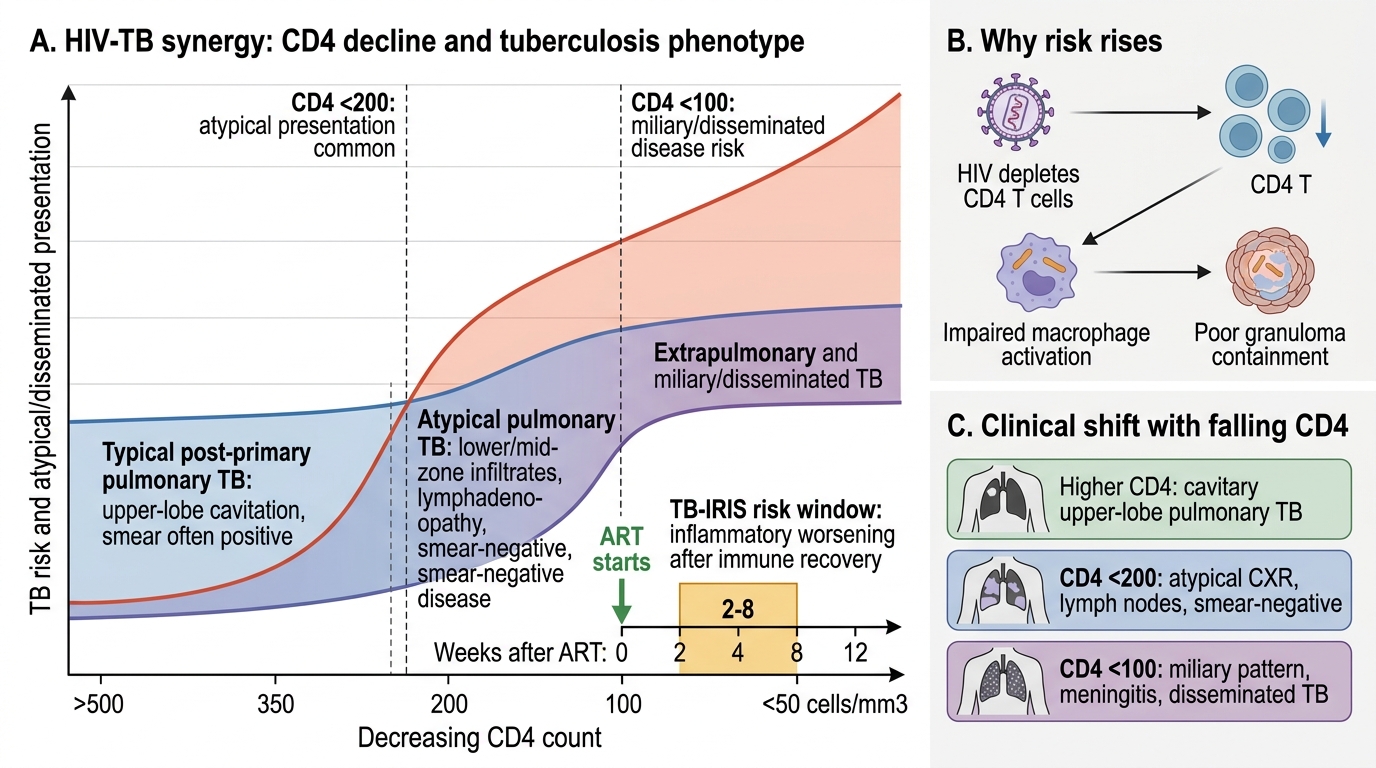
HIV-TB co-infection — the lethal synergy: HIV is the most potent known risk factor for progressing from LTBI to active TB. The mechanism is the depletion of CD4+ T lymphocytes — the effector cells of the Th1 anti-TB response. As CD4 count falls:
- At CD4 >350 cells/μL: TB risk is elevated 5–10-fold above HIV-negative individuals, but the clinical presentation resembles typical pulmonary TB with upper-lobe cavitation.
- At CD4 200–350 cells/μL: Risk is 20–30-fold elevated; atypical presentations increase — lower-lobe consolidation, less cavitation, more hilar lymphadenopathy.
- At CD4 <200 cells/μL: Risk is 50–100-fold elevated; extrapulmonary, disseminated, and miliary TB predominate; sputum smear is often negative despite active disease (fewer bacilli in secretions); skin test and IGRA are frequently negative (anergy from severe immunosuppression — a critical pitfall).
The clinical consequences of HIV-TB co-infection include: higher mortality, greater risk of drug interactions (rifampicin induces cytochrome P450 enzymes — accelerates metabolism of many antiretrovirals including protease inhibitors), immune reconstitution inflammatory syndrome (IRIS) when antiretroviral therapy (ART) is initiated during TB treatment (a paradoxical worsening as immune function recovers and mounts a stronger inflammatory reaction to TB antigens), and higher rates of relapse. According to NACO (National AIDS Control Organisation) guidelines, all HIV-positive patients must be screened for TB at every clinic visit using the four-symptom screen (cough, fever, night sweats, weight loss), and all TB patients must be tested for HIV.
NTEP–NACO integration: HIV-positive TB patients should start ART within 2–8 weeks of initiating anti-TB therapy regardless of CD4 count, with the timing modified only if CNS TB is present (delay ART to 8 weeks to reduce IRIS-related intracranial pressure). TB-preventive therapy (isoniazid preventive therapy, IPT — isoniazid 5 mg/kg daily for 6 months, or newer 3HP regimen: isoniazid + rifapentine once weekly for 3 months) is recommended for all HIV-positive individuals who have ruled out active TB.
Diabetes mellitus and TB — India's dual epidemic: India has the world's second-largest burden of both TB and type 2 diabetes. People with diabetes have a 2–3-fold higher risk of developing active TB and a significantly higher risk of drug-resistant TB. The mechanisms are multiple: impaired neutrophil and macrophage function due to chronic hyperglycaemia, reduced T-cell proliferation, and altered pulmonary microenvironment. Clinically, diabetes-associated TB more often presents with atypical lower-lobe involvement, greater severity at diagnosis, slower sputum conversion, and higher treatment failure rates. All TB patients should be screened for diabetes (fasting glucose or HbA1c at diagnosis), and diabetic patients should be screened for TB symptoms at each visit. Management of both conditions simultaneously improves outcomes for both.
Malnutrition: India's prevalence of undernutrition among TB patients is striking — studies show that 50–70% of TB patients are malnourished at diagnosis, with BMI often below 18.5 kg/m². Malnutrition impairs cell-mediated immunity, reduces the CD4:CD8 ratio, decreases macrophage function, and reduces drug absorption. The Ni-kshay Poshan Yojana (NTEP nutritional support) was designed explicitly to address this. Nutritional assessment and supplementation are integral to TB management.
Other comorbidities: CKD reduces immune function and requires dose adjustment of ethambutol and pyrazinamide (both renally cleared); liver disease complicates use of hepatotoxic agents (isoniazid, rifampicin, pyrazinamide); prolonged corticosteroid therapy increases TB risk and may mask signs of infection. TNF-α antagonists (used in rheumatoid arthritis, inflammatory bowel disease) powerfully suppress the granuloma maintenance — screening for LTBI and treating with TB preventive therapy is mandatory before starting any TNF-α blocker.
HIV-TB Synergy Across CD4 Decline
Drug Resistance in Tuberculosis — Epidemiology, Mechanisms, and Determinants
Drug-resistant tuberculosis (DR-TB) represents the most serious threat to the global TB control effort and the single greatest challenge to the NTEP's elimination goal. India, as the country with the highest absolute number of TB cases, correspondingly carries one of the highest absolute burdens of DR-TB worldwide — a crisis that is simultaneously a scientific problem (inadequate drugs), a programme problem (inadequate supervision and support), and a patient problem (inadequate adherence resources in a context of catastrophic costs). Understanding the biology of resistance is not an academic exercise: it determines why the physician must never add a single drug to a failing regimen, why adequate dosing and duration are non-negotiable, and why universal drug sensitivity testing before any TB treatment is a rational and essential programme design choice. The principles that explain how resistance arises are also the principles that explain why combination therapy is the only bacteriologically coherent treatment approach for tuberculosis, and grasping this connection transforms treatment guidelines from arbitrary rules into logical necessities.
Classification of drug resistance:
- Mono-resistance: resistance to one first-line anti-TB drug only.
- Poly-drug resistance (PDR): resistance to more than one first-line drug, but NOT the combination of isoniazid and rifampicin.
- Multi-drug-resistant TB (MDR-TB): resistance to at least isoniazid (H) and rifampicin (R) — the two most bactericidal first-line drugs. This is the clinically critical threshold because it eliminates the most effective agents from the regimen.
- Pre-extensively drug-resistant TB (pre-XDR-TB): MDR/RR-TB plus resistance to any fluoroquinolone (levofloxacin or moxifloxacin).
- Extensively drug-resistant TB (XDR-TB): MDR/RR-TB plus resistance to any fluoroquinolone AND at least one of bedaquiline or linezolid.
- Rifampicin-resistant TB (RR-TB): resistance to rifampicin detected by molecular testing (often used interchangeably with MDR-TB for treatment purposes under NTEP since RR-TB alone mandates second-line therapy).
Magnitude: According to the WHO Global TB Report 2023, India has approximately 119,000 MDR/RR-TB cases annually, the largest absolute number globally. The treatment success rate for MDR-TB is approximately 57% — far lower than the 88–90% for drug-sensitive TB — reflecting the complexity and toxicity of second-line regimens.
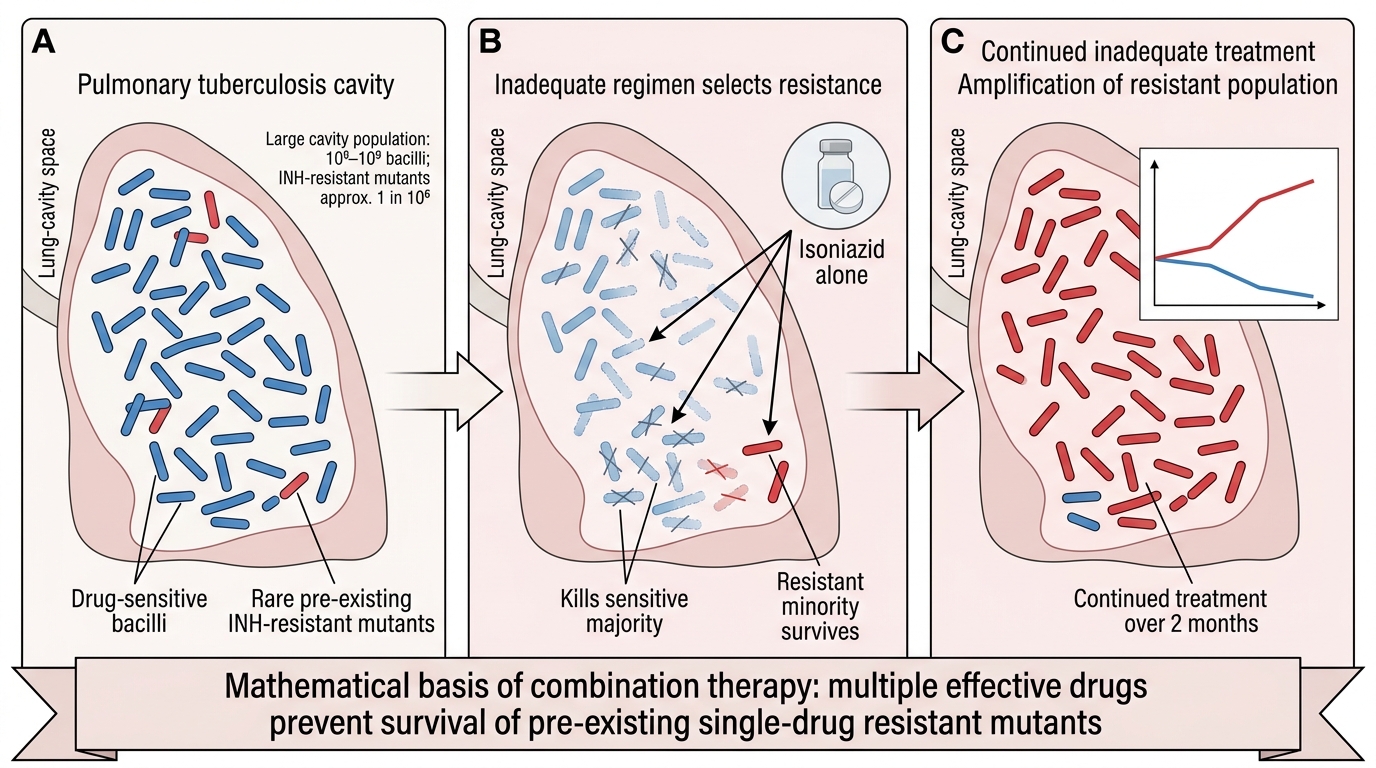
Mechanism of drug resistance — mutations, not plasmids: Unlike resistance in Gram-negative bacteria (where plasmid-mediated horizontal gene transfer is common), drug resistance in M. tuberculosis arises exclusively through chromosomal point mutations — there are no plasmids, no integrons, no class 1 integron-mediated transfer. Every resistance mutation must be selected de novo from the spontaneous mutation rate of the organism (approximately 1 in 10⁶–10⁸ bacilli for each drug). In an untreated cavitary TB patient, the cavity can contain 10⁸–10⁹ bacilli, meaning statistically, pre-existing resistant mutants exist for every drug at therapy initiation. The key bacteriological insight: a single-drug mutant is present at an undetectable frequency; for two drugs, the probability is the product of individual rates (10⁻⁶ × 10⁻⁸ = 10⁻¹⁴), which is why combination therapy is bacteriologically essential and why adding one drug to a failing regimen (virtual monotherapy) simply selects the doubly-resistant subpopulation.
Key resistance gene mutations for first-line drugs:
- Isoniazid (H): mutations in katG (catalase-peroxidase, activates isoniazid — >70% of H-resistance), inhA promoter region (NADH-enoyl ACP reductase).
- Rifampicin (R): mutations in rpoB (beta subunit of RNA polymerase) — present in >95% of RIF-resistant strains and detectable by CBNAAT/Xpert MTB/RIF.
- Pyrazinamide (Z): mutations in pncA (pyrazinamidase).
- Ethambutol (E): mutations in embB (arabinosyl transferase).
- Fluoroquinolones: mutations in gyrA and gyrB (DNA gyrase subunits).
Determinants of drug resistance — why does it emerge?
The epidemiology of resistance is determined by three interacting factors:
1. Microbial factors: spontaneous mutation rates, fitness of resistant mutants, and transmissibility (MDR strains of the Beijing genotype are highly fit and transmissible).
2. Therapeutic/programmatic factors: inadequate regimen (too few drugs, wrong drugs), inadequate duration (premature treatment cessation), poor quality drugs (substandard fixed-dose combinations), interruption due to side effects or supply chain failure, monotherapy or virtual monotherapy (adding a single drug to a failing regimen), and lack of drug sensitivity testing (DST) before treatment.
3. Patient and system factors: irregular drug intake (the historically cited driver under DOTS — now mitigated by daily directly observed treatment), poor treatment support, comorbidities reducing drug absorption, and critically, transmission of resistant strains (primary resistance) — a patient acquiring MDR-TB from contact with an MDR case has primary resistance, never had a sensitive strain.
Programmatic implications: The NTEP's move to universal drug sensitivity testing (DST) — using CBNAAT (Xpert MTB/RIF) at diagnosis and line probe assay (LPA) for first- and second-line drug resistance — directly addresses the diagnostic gap. The current NTEP guidelines mandate upfront NAAT/DST before initiating treatment, precisely to detect RR/MDR-TB early and prevent inadvertent monotherapy.
Emergence of Acquired Drug Resistance in Tuberculosis
SELF-CHECK
A patient with smear-positive pulmonary TB was treated with isoniazid alone for 2 months by a private physician before being referred to an NTEP centre. What is the most likely consequence of this treatment approach?
A. The patient will develop immunity to TB and the disease will be cured
B. Selection and amplification of isoniazid-resistant mutants, creating acquired drug resistance
C. Sputum conversion to smear-negative without any risk of resistance
D. No significant consequence as isoniazid is the most bactericidal first-line drug
Reveal Answer
Answer: B. Selection and amplification of isoniazid-resistant mutants, creating acquired drug resistance
Treating TB with a single drug (monotherapy) is the classical mechanism of acquired drug resistance. In an untreated pulmonary TB cavity with 10⁸–10⁹ bacilli, spontaneous isoniazid-resistant mutants already exist at a frequency of approximately 1 per 10⁶ bacteria. Isoniazid monotherapy kills the sensitive majority but selects the resistant minority. Over 2 months, the resistant population becomes dominant. This is called amplification — turning a pre-existing minority into the predominant strain. The correct approach (combination therapy with at least 4 drugs in the initial phase) prevents this because the probability of a mutant resistant to all four drugs simultaneously is astronomically low (10⁻⁶ × 10⁻⁸ × 10⁻³ × 10⁻² = 10⁻¹⁹). This case will now require DST and likely MDR-TB workup before treating.
BCG Vaccine — Origins, Technique, Efficacy, and Complications
The Bacille Calmette-Guérin (BCG) vaccine is the world's most widely administered vaccine and the only currently licensed vaccine against tuberculosis. Despite nearly a century of use, it remains the subject of significant scientific debate — its efficacy against pulmonary TB in adults is inconsistent across trials, yet its role in preventing severe childhood TB is unequivocal and forms the basis of its inclusion in India's Universal Immunisation Programme.
Origins: BCG was developed by Albert Calmette and Camille Guérin at the Pasteur Institute, Lille, between 1906 and 1921, through 230 serial subcultures of a virulent M. bovis strain on potato-glycerine-ox bile medium over 13 years. Progressive attenuation (loss of virulence) without loss of immunogenicity produced the live attenuated strain first used in humans in 1921. Multiple daughter strains (Tokyo, Danish 1331, Pasteur, Glaxo, Connaught) were developed from this original culture; they differ slightly in lipid content, immunogenicity, and reactogenicity. India primarily uses the Danish 1331 strain through its national programme.
Indications: BCG is indicated for:
- All neonates at birth (or as soon as possible after birth) under India's Universal Immunisation Programme, regardless of maternal HIV status (WHO recommends withholding BCG only from symptomatic HIV-positive infants).
- Children under 5 years who have not received BCG and are tuberculin-negative.
- Healthcare workers with confirmed negative TST in settings where TB exposure is high (institutional policy-dependent).
- Contacts of multibacillary leprosy (BCG also provides approximately 50% protection against leprosy — the vaccine's most consistent and uniform efficacy).
Contraindications:
- Symptomatic HIV infection or known immune deficiency states (due to risk of BCG-itis and disseminated BCG disease from the live attenuated organism).
- Active generalised skin disease at the vaccination site.
- High-dose corticosteroid or immunosuppressive therapy.
Technique of administration:
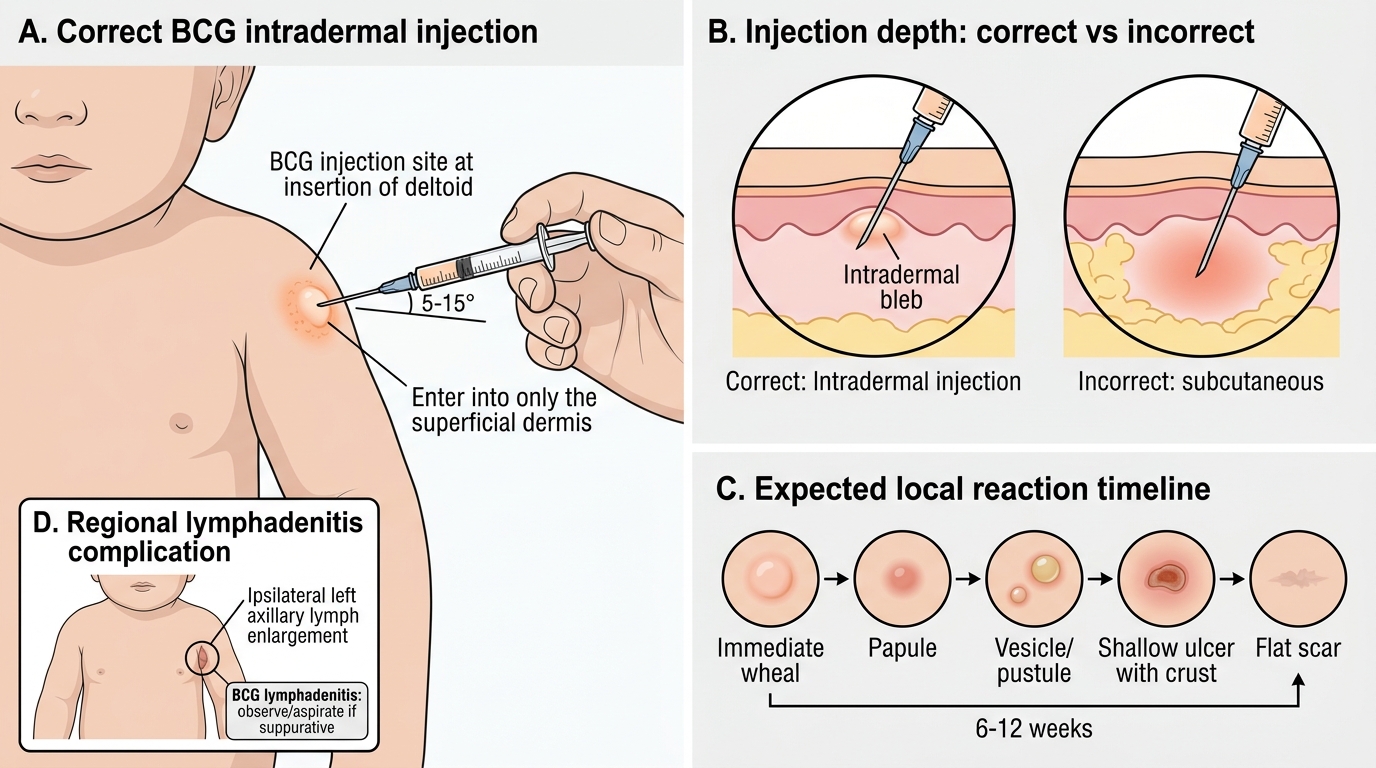
- Route: strictly intradermal (ID) injection only — subcutaneous injection causes excessive local reaction, cold abscess, and inadequate immunogenicity.
- Site: left deltoid region, at the insertion of the deltoid (upper arm), standardised to allow BCG scar identification in field surveys.
- Dose: 0.1 mL for children >1 month; 0.05 mL for neonates under 1 month.
- Reconstitution: BCG is a lyophilised (freeze-dried) live vaccine; it must be reconstituted with the supplied diluent (0.9% saline), kept cold (2–8°C), used within 4–6 hours of reconstitution, and protected from sunlight at all times.
- Expected local reaction: a small papule appears at the injection site within 2–4 weeks, which evolves through a vesicle stage, forms a superficial ulcer (5–7 mm), and heals over 6–12 weeks leaving a characteristic BCG scar (a small, round, slightly depressed scar). The scar confirms successful vaccination in field settings.
Mechanism of immunity: BCG induces cell-mediated immunity similar to natural TB infection — it trains CD4+ Th1 cells, generates memory T cells, and elicits a positive TST response (one reason BCG-vaccinated individuals may have a positive TST). BCG does not prevent infection but reduces the risk of progression to severe disease by accelerating the memory immune response on subsequent encounter with M. tuberculosis.
Efficacy:
- Children — highly effective: BCG provides approximately 70–80% protection against tuberculous meningitis and miliary TB in young children. This protection is the strongest and most consistent finding across all trials globally and forms the primary justification for neonatal vaccination in high-burden countries.
- Adults — variable and inconsistent: Efficacy against pulmonary TB in adults ranges from 0% to 80% across different randomised trials. The reasons for this variability are incompletely understood but include: differences in BCG strain, exposure to environmental non-tuberculous mycobacteria (NTM) in tropical countries (which may mask BCG's immunological effect — the "hygiene hypothesis" for BCG), and latitude effects (efficacy higher in cooler northern latitudes). The landmark MRC Madanapalle trial conducted in Tamil Nadu in the 1970s showed almost zero efficacy of BCG against pulmonary TB in adults in India — a finding that has never been fully explained.
- Duration: Protection appears to wane significantly by 10–15 years after vaccination, which is why BCG is not recommended as a booster strategy in adults under current Indian policy.
Complications of BCG vaccination:
- Local reactions: Keloid formation (more common with subcutaneous injection or certain strains), prolonged ulceration (>12 weeks), and satellite lymphadenitis (regional axillary lymph node enlargement — usually resolves spontaneously; large fluctuant nodes may require aspiration but NOT surgical incision, which risks sinus formation).
- BCG lymphadenitis (suppurative): The most common serious local complication — a fluctuant, tender axillary or cervical lymph node. Management: needle aspiration; oral isoniazid for 6 months is sometimes used though evidence is limited; surgical excision is a last resort.
- Disseminated BCG disease (BCG-itis): A rare but life-threatening complication, occurring almost exclusively in infants with severe combined immunodeficiency (SCID), symptomatic HIV, or other profound immunodeficiency. The live attenuated organism disseminates haematogenously, causing multi-organ granulomatous disease. Treatment requires prolonged anti-TB therapy excluding pyrazinamide (BCG is naturally resistant to pyrazinamide as it lacks a functional pyrazinamidase).
- Osteitis/osteomyelitis: Very rare; more reported with certain BCG strains (Gothenburg, Finnish).
BCG Vaccination Technique and Local Reaction Timeline
SELF-CHECK
A 4-month-old infant presents with a 3 cm, fluctuant, non-tender left axillary lymph node. She received BCG at birth at the left deltoid. The node appeared 6 weeks after vaccination. There is no fever, no weight loss, and the child is otherwise well. What is the most appropriate management?
A. Immediate surgical excision of the lymph node
B. Start standard 4-drug anti-TB treatment (2HRZE/4HRE)
C. Needle aspiration of the node; observe without anti-TB drugs unless immunodeficiency is detected
D. Admit for IV antibiotics targeting staphylococcal infection
Reveal Answer
Answer: C. Needle aspiration of the node; observe without anti-TB drugs unless immunodeficiency is detected
This is BCG lymphadenitis — suppurative regional lymphadenopathy following BCG vaccination, the most common significant local complication. In an otherwise well, immunocompetent infant, the recommended management is needle aspiration (both diagnostic and therapeutic) to decompress the node, followed by observation. Surgical excision carries the risk of sinus formation and is reserved for large nodes that recur or fail aspiration. Standard 4-drug anti-TB therapy is not indicated — this is a local complication from the live attenuated BCG strain, not active M. tuberculosis disease, and the infant shows no systemic TB features. Anti-TB drugs should be considered only if there is evidence of disseminated BCG disease or immunodeficiency. IV antibiotics would be appropriate for pyogenic (staphylococcal) lymphadenitis, but BCG lymphadenitis does not respond to antibiotics.