Page 8 of 22
IM28.11-14 | Obstructive Airway Disease Functional and Imaging Tests — SDL Guide
Learning Objectives
- Describe, discuss, and interpret pulmonary function tests including spirometry and flow-volume loops
- Perform and interpret peak expiratory flow rate (PEFR) measurement
- Describe the appropriate diagnostic workup for suspected obstructive airway disease based on the presumed aetiology
- Enumerate the indications for and interpret the results of pulse oximetry, arterial blood gas (ABG), and chest radiograph in obstructive airway disease
INSTRUCTIONS
Functional and imaging investigations translate the clinical suspicion raised by history and examination into objective, measurable evidence that confirms diagnosis, quantifies severity, and guides management. This module covers the performance, interpretation, and clinical reasoning behind the key investigations for obstructive airway disease at the SH (Skills and Higher) level required by NMC competencies IM28.11–28.14.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 279 — Pulmonary Function Testing (textbook)
- API Textbook of Medicine, 10th ed. — Investigations in Respiratory Disease (textbook)
- Davidson's Principles & Practice of Medicine, 23rd ed. — Investigations in Respiratory Disease (textbook)
- ATS/ERS Technical Standard: Interpretive Strategies for Lung Function Tests, 2022 (guideline)
- GOLD Report 2023 — Spirometric Diagnosis and Assessment (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 48-year-old male smoker comes to your clinic. He has had a morning cough for four years and says he gets breathless only on 'hard work'. His physical examination is completely normal today — no wheeze, normal breath sounds, normal percussion, no hyperinflation signs. His SpO₂ is 95%. You could send him away reassured. But you order spirometry. The result: FEV1/FVC 0.58 (post-bronchodilator), FEV1 62% predicted. He has GOLD 2 COPD — moderate disease, asymptomatic on a good day, but his FEV1 is already 38% below what it should be for his age and height. Without spirometry, this diagnosis is invisible. This is the lesson: clinical evaluation identifies the possibility of obstructive airway disease; investigations make it objective, quantify severity, and open the door to prognosis and treatment planning.
WHY THIS MATTERS
In final-year clinical practice you will be expected to order, perform, and interpret the investigations that confirm obstructive airway disease. Spirometry is the gold standard for diagnosis; PEFR is the bedside tool for monitoring and emergency assessment; ABG determines respiratory failure type and guides oxygen therapy decisions; chest radiograph identifies complications and alternative diagnoses. Competency IM28.11–28.14 covers all four domains at the SH level — meaning you must not only know the thresholds but understand what to do with the results in the context of a real patient.
RECALL
Recall the key spirometric measurements before proceeding. FEV1 (forced expiratory volume in 1 second): the volume exhaled in the first second of maximal forced expiration from full inspiration. FVC (forced vital capacity): the total volume exhaled during maximal forced expiration. FEV1/FVC ratio: the fraction of FVC exhaled in the first second; the key obstruction indicator. PEFR (peak expiratory flow rate): the maximum flow rate achieved during forced expiration, measured in L/min; a surrogate for large-airway calibre. Recall also the ABG reference ranges: PaO₂ 80–100 mmHg, PaCO₂ 35–45 mmHg, pH 7.35–7.45, HCO₃⁻ 22–26 mEq/L on room air at sea level. These numbers are the benchmarks against which all abnormal results are interpreted.
Pulmonary Function Tests: Technique, Interpretation, and Clinical Relevance
Spirometry is the clinical indication and reference standard for the diagnosis and severity assessment of obstructive airway disease. It should be performed in any patient with persistent respiratory symptoms (dyspnoea, cough, wheeze), a significant smoking history (>10 pack-years), suspected occupational lung disease, or before and after bronchodilator therapy to assess reversibility. The governing principle is that spirometry objectifies the degree of airflow limitation and — through the bronchodilator reversibility test — distinguishes asthma (reversible obstruction) from COPD (persistent obstruction), a distinction that profoundly affects management and prognosis.
Technique for spirometry:
The patient should be seated, wearing a nose clip, with an appropriate-sized mouthpiece held firmly between the teeth and lips. Instruct: (1) inhale fully to total lung capacity; (2) seal the lips around the mouthpiece; (3) blast out as hard and fast as possible; (4) continue exhaling until no more air can be expelled (or for ≥6 seconds in adults, ≥3 seconds in children). A minimum of three acceptable and reproducible manoeuvres are required, with the best FEV1 and best FVC selected for reporting (from different blows). Acceptability criteria: the manoeuvre starts abruptly (no hesitation or false start), shows a smooth peak on the flow-volume curve, has no cough in the first second, and is continued for adequate duration. Reproducibility criteria: the two best FEV1 values must be within 150 mL of each other.
Key measurements and their interpretation:
- FEV1/FVC < 0.70 post-bronchodilator = obstruction (GOLD criterion for COPD)
- FEV1 % predicted after bronchodilator = severity in COPD (GOLD 1–4; see below)
- Bronchodilator response: administer salbutamol 400 mcg (4 × 100 mcg puffs via spacer) or ipratropium 160 mcg, wait 15 minutes (salbutamol) or 30 minutes (ipratropium), then repeat spirometry. A significant response = FEV1 increase ≥12% AND ≥200 mL from pre-bronchodilator baseline — favours asthma (or ACOS)
- GOLD severity grades (post-bronchodilator FEV1 % predicted, when FEV1/FVC < 0.70):
- GOLD 1 Mild: FEV1 ≥80%
- GOLD 2 Moderate: 50% ≤ FEV1 < 80%
- GOLD 3 Severe: 30% ≤ FEV1 < 50%
- GOLD 4 Very Severe: FEV1 < 30%
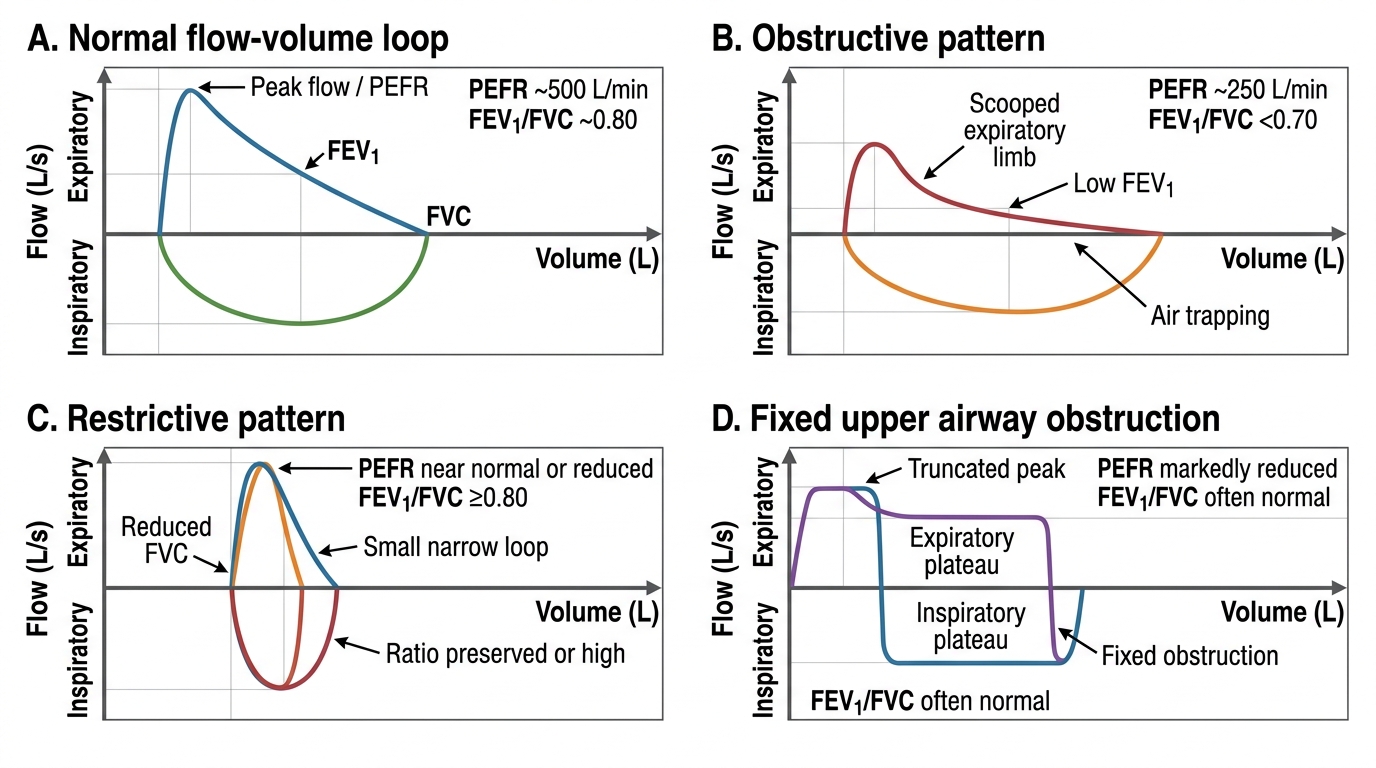
The flow-volume loop:
The flow-volume loop plots expiratory flow (y-axis, L/sec) against volume exhaled (x-axis, L). The normal loop has a rapid rise to a sharp peak flow, then a linear decline back to zero. In obstruction, the expiratory limb shows a characteristic scooped-out concavity (flow is disproportionately reduced relative to volume — small airway collapse during forced expiration). In restriction, the loop is narrow (reduced FVC) but the shape is preserved (no scooping). In large airway obstruction (tracheal stenosis, tumour), the peak flow is truncated and the loop shows a plateau (fixed obstruction) or variable flattening of the inspiratory or expiratory limb. The flow-volume loop provides pattern recognition beyond the FEV1/FVC ratio alone.
Additional PFT parameters (relevant in complex cases):
- Total lung capacity (TLC): increased in emphysema (air trapping); reduced in restriction
- Residual volume (RV): markedly increased in emphysema — the hallmark of air trapping
- RV/TLC ratio: >40% indicates significant air trapping
- Diffusing capacity (DLCO): reduced in emphysema (loss of alveolar surface area) but normal or increased in chronic bronchitis and asthma — DLCO distinguishes emphysema from other obstructive patterns
Spirometry Flow-Volume Loop Patterns
Peak Expiratory Flow Rate: Performance and Interpretation
Peak expiratory flow rate (PEFR) is the maximum flow rate achieved during a maximal forced expiratory manoeuvre from full inspiration. It is measured in litres per minute using a peak flow meter — a simple, portable, inexpensive device that requires no computer or calibration equipment beyond manufacturer checking. PEFR measurement is the key bedside assessment tool for asthma monitoring and severity grading in acute attacks, and it is the investigation you are most likely to perform yourself at the bedside during your clinical years and early career. NMC competency IM28.12 requires you to perform PEFR correctly and interpret the results accurately.
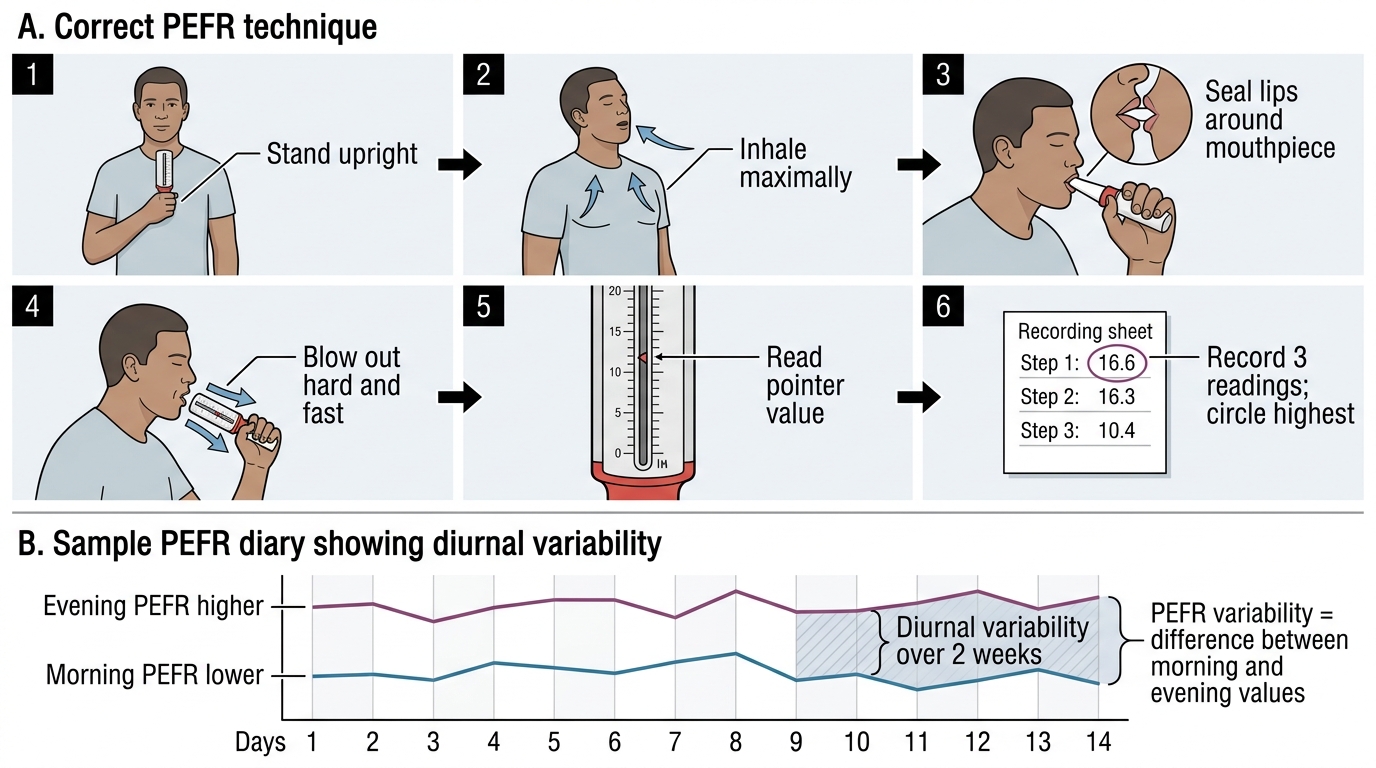
Technique for PEFR measurement:
The following steps describe the standard technique for performing PEFR. Adherence to this sequence is essential for reproducibility — even small departures from technique (incomplete inhalation, a loose lip seal, a slow rather than explosive exhalation) can reduce the reading by 50–80 L/min, leading to underestimation of true function and inappropriate severity classification. The technique should be taught to every patient who is prescribed a peak flow meter for home monitoring, with performance checked and corrected at every clinic visit because patient technique degrades over time without reinforcement.
1. Patient position: standing (preferred) or sitting upright — lying down reduces PEFR by approximately 20% and is not acceptable for formal assessment
2. Preparation: hold the peak flow meter horizontally, ensure the pointer is at zero, check that your fingers do not obstruct the vents or the pointer travel
3. Inhalation: instruct the patient to inhale fully to total lung capacity — a maximum breath in
4. Seal and blast: place the mouthpiece between the teeth and lips with a tight seal; blast out as hard and fast as possible in a single short explosive exhalation (duration 1–2 seconds — PEFR measures only peak flow, not sustained flow, so a short sharp effort suffices)
5. Read and record: note the pointer position in L/min
6. Repeat: perform three manoeuvres with a 30-second interval and record the highest of the three values — this is the reported PEFR
7. Compare to personal best or predicted: PEFR is most meaningful when compared to the patient's own personal best (established during optimal control) or age-height-sex predicted norms from reference tables
PEFR reference values and predicted normals:
PEFR varies substantially with age, height, sex, and ethnicity. The reference ranges used in Indian practice are based on Caucasian equations with correction factors, or, better, Indian-specific equations (Udwadia equations for Indian adults). For examination purposes, know the general ranges: adult males approximately 450–650 L/min; adult females 350–500 L/min. Personal best — measured during optimal asthma control after 2–3 weeks of optimal therapy — is the most clinically meaningful reference value for monitoring.
Interpretation of PEFR in acute asthma:
PEFR as a percentage of personal best (or predicted) is used to classify severity of an acute asthma attack:
- PEFR ≥75% personal best = mild
- PEFR 50–75% = moderate
- PEFR 33–50% = severe
- PEFR <33% = life-threatening
PEFR variability for asthma diagnosis:
In stable outpatient settings, serial PEFR monitoring over 2–4 weeks is used to confirm variable airway obstruction in suspected asthma. The patient records morning (immediately on waking, before inhaler use) and evening PEFR daily. Diurnal variability = (evening PEFR − morning PEFR) / evening PEFR × 100%. Variability >20% on most days strongly supports the diagnosis of asthma. This is also how occupational asthma is confirmed — increased variability on working days compared to days off.
Limitations of PEFR:
PEFR is effort-dependent and requires patient cooperation and consistent technique; it primarily reflects large-airway calibre (less sensitive to small-airway obstruction than FEV1); it cannot distinguish between asthma and COPD (both reduce PEFR); and it has wider within-subject and between-subject variability than spirometry. Therefore, spirometry remains the reference standard for diagnosis — PEFR is best used for monitoring and rapid severity assessment in acute settings.
PEFR Technique and Diary Recording
SELF-CHECK
A 22-year-old asthmatic woman presents to emergency with acute breathlessness. Her personal best PEFR is 460 L/min. Today her PEFR is 145 L/min. Which severity category does this place her in, and what does this require?
A. Moderate asthma (50–75% personal best) — treat with nebulised salbutamol and discharge
B. Severe asthma (33–50% personal best) — requires hospital assessment and systemic steroids
C. Life-threatening asthma (<33% personal best) — requires immediate treatment and ICU consideration
D. Mild asthma (≥75% personal best) — can be managed with increased inhaler frequency at home
Reveal Answer
Answer: C. Life-threatening asthma (<33% personal best) — requires immediate treatment and ICU consideration
PEFR 145/460 × 100 = 31.5% of personal best — this is BELOW 33%, placing this patient in the LIFE-THREATENING category. This requires immediate hospital admission, high-dose nebulised salbutamol and ipratropium, systemic corticosteroids (IV or oral), controlled supplemental oxygen to SpO₂ 94–98%, and ABG measurement. ICU involvement should be considered immediately. A PEFR this low — less than one-third of personal best — indicates near-complete airway closure and is associated with a very high risk of respiratory arrest. This patient should never be discharged from the emergency department.
Diagnostic Workup: Selecting Investigations Based on Presumed Aetiology
The choice of diagnostic investigations in suspected obstructive airway disease should be tailored to the presumed aetiology derived from the clinical evaluation. A targeted investigation strategy avoids unnecessary tests, reduces cost and patient burden, and focuses on investigations that will change management. In Indian practice, where patients may present late, where biomass-related COPD affects non-smoking women who are often not initially suspected of having airway disease, and where resources may be prioritised differently in different settings, the ability to construct a rational, prioritised investigation sequence is a core competency. The investigation plan must always be anchored in three questions: What do I need to confirm the diagnosis? What do I need to grade severity and guide treatment? What do I need to exclude dangerous alternative diagnoses or complications? This section outlines the recommended workup for the major clinical scenarios you will encounter.
Provided image
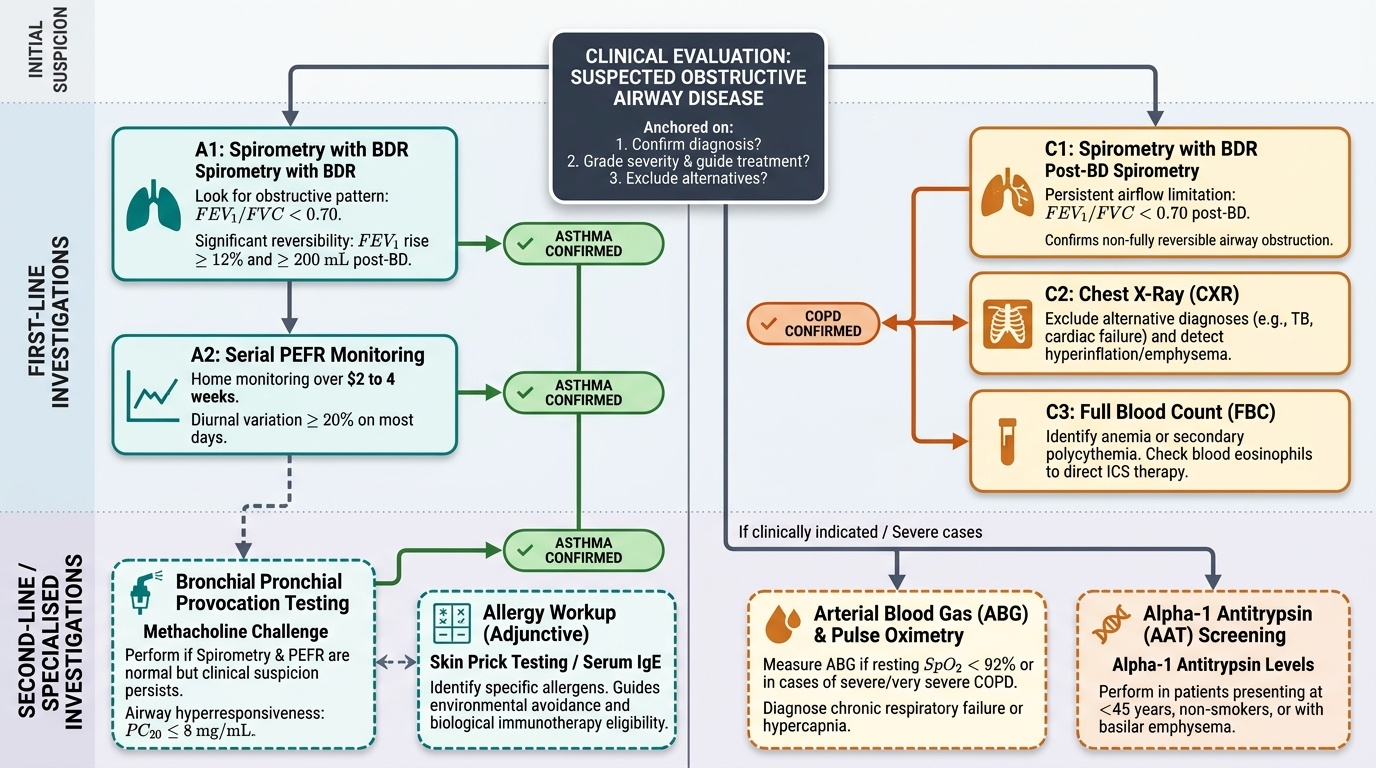
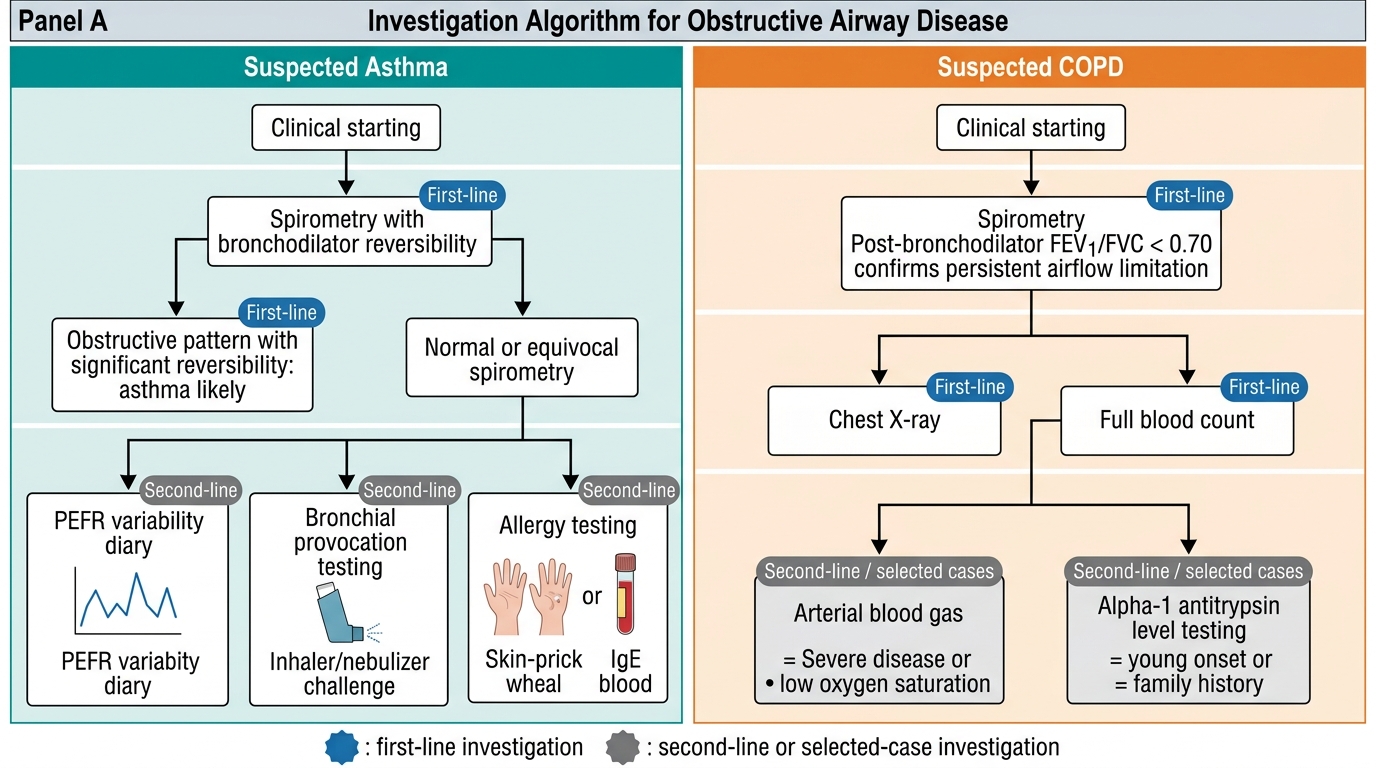
Scenario 1 — Suspected ASTHMA (young patient, episodic symptoms, atopy, reversible obstruction):
The investigation strategy aims to confirm variable airflow limitation and, if spirometry is initially normal, to demonstrate bronchial hyperresponsiveness:
- Spirometry with bronchodilator reversibility — confirm obstruction (FEV1/FVC < 0.70) and significant reversibility (≥12% and ≥200 mL FEV1 rise): this is sufficient to confirm asthma if the pre-bronchodilator FEV1/FVC is obstructed
- Serial PEFR monitoring (if resting spirometry is normal between attacks) — document ≥20% diurnal variation on most days over 2–4 weeks
- Bronchial provocation testing (methacholine challenge) — if spirometry and PEFR are both normal; a positive challenge (PC₂₀ ≤8 mg/mL) confirms airway hyperresponsiveness
- Skin prick testing or serum-specific IgE — to identify specific allergens in allergic asthma; guides allergen avoidance counselling and, if severe, allergen immunotherapy eligibility
- Full blood count (FBC) — peripheral eosinophilia (≥300 cells/mcL) supports eosinophilic asthma and may influence biologic therapy eligibility
- Total IgE and specific IgE to Aspergillus — to exclude ABPA in patients with asthma and recurrent exacerbations, radiographic infiltrates, or eosinophilia
- CXR — primarily to exclude alternative diagnoses (pneumothorax, pneumonia, cardiac enlargement); the chest radiograph is usually normal in uncomplicated asthma
Scenario 2 — Suspected COPD (>40 years, smoker/biomass exposure, progressive dyspnoea, chronic cough):
- Spirometry (post-bronchodilator) — confirm persistent obstruction (FEV1/FVC < 0.70 post-BD); document FEV1 % predicted for GOLD grading
- Chest radiograph (CXR) — characteristically shows hyperinflation (flat diaphragms, increased retrosternal airspace, horizontal ribs, lung periphery hyperlucency — 'oligaemia'); may show bullae in emphysema; important to exclude pneumonia complicating exacerbation, pneumothorax, and lung cancer (a smoking-related comorbidity that must not be missed)
- Arterial blood gas (ABG) — indicated in GOLD 3–4 (FEV1 <50%), resting SpO₂ ≤92%, clinical signs of hypercapnia or cor pulmonale; determines whether type-1 or type-2 respiratory failure is present and guides oxygen therapy decisions
- Full blood count — may show secondary polycythaemia (elevated haemoglobin and haematocrit) from chronic hypoxia; this is a marker of chronic significant hypoxaemia and a risk factor for thrombosis
- Serum AAT level — in all COPD patients diagnosed under 45 years, non-smokers with COPD, or emphysema with lower-lobe predominance
- ECG — in patients with suspected cor pulmonale: right axis deviation, P pulmonale (peaked P wave >2.5 mm in lead II), right bundle branch block, S1Q3T3 pattern
- Echocardiogram — if cor pulmonale suspected clinically; quantifies pulmonary artery pressure
- CT chest — not routinely required for diagnosis; indicated for: evaluation of emphysema subtype and distribution (pre-surgical assessment for lung volume reduction surgery or bullectomy), characterisation of a pulmonary nodule, or suspected bronchiectasis coexisting with COPD
Scenario 3 — Acute exacerbation of OAD:
The investigation strategy during an acute exacerbation is directed at confirming the diagnosis, determining severity, identifying the precipitant, and guiding immediate management:
- SpO₂ (pulse oximetry) — immediate, continuous monitoring; determines urgency of supplemental oxygen
- ABG — if SpO₂ <92% on room air or in known CO₂ retainer; classifies type of respiratory failure and guides NIV/ICU decision
- CXR — to exclude pneumonia, pneumothorax, pulmonary oedema
- PEFR or spirometry — to quantify severity (PEFR % personal best in asthma; spirometry if clinically feasible in COPD exacerbation)
- FBC — leucocytosis supports bacterial infection
- Sputum Gram stain and culture — in moderate-severe COPD exacerbations with purulent sputum or if hospital-acquired or resistant organism suspected
- Blood cultures — if febrile or septic
- ECG — arrhythmia precipitating or complicating exacerbation; signs of right heart strain
- D-dimer ± CTPA — if clinical suspicion of pulmonary embolism as precipitant (unexplained tachycardia, low-grade fever, pleuritic pain, Wells score ≥2)
Investigation Algorithm for Asthma and COPD