Page 9 of 22
IM28.11-14 | Obstructive Airway Disease Functional and Imaging Tests — SDL Guide (Part 2)
Pulse Oximetry, ABG, and Chest Radiograph: Indications and Interpretation
Three investigations — pulse oximetry, arterial blood gas analysis, and chest radiograph — form the core of bedside and emergency assessment in obstructive airway disease and are specifically mandated by NMC competency IM28.14. Each provides distinct, non-redundant information, and each has specific indications that determine when it should be ordered.
Pulse Oximetry:
Indication: all patients presenting with acute breathlessness, exacerbation of OAD, or any respiratory complaint. SpO₂ measurement is rapid, non-invasive, and continuous — it should be the first investigation in any breathless patient. Interpretation: SpO₂ ≥95% on room air = acceptable oxygenation (target 94–98% for most patients; 88–92% for known CO₂ retainers). SpO₂ <92% = significant hypoxaemia requiring supplemental oxygen and investigation. SpO₂ <88% = severe hypoxaemia requiring urgent intervention. Limitations of pulse oximetry: it measures only oxygenation (not ventilation — cannot detect hypercapnia); falsely elevated in carbon monoxide poisoning (carboxyhaemoglobin registers as oxyhaemoglobin); inaccurate with poor peripheral perfusion (cold hands, Raynaud's, arrhythmia, significant anaemia); a normal SpO₂ does not exclude early respiratory failure if CO₂ is rising.
Arterial Blood Gas (ABG) Analysis:
Indications: SpO₂ <92% on room air or despite supplemental oxygen; known or suspected chronic CO₂ retainer; clinical signs of hypercapnia (drowsiness, confusion, asterixis, bounding pulse, warm peripheries); acute severe or life-threatening asthma; acute exacerbation of COPD requiring hospitalisation; GOLD 3–4 COPD at baseline assessment for LTOT eligibility; unexplained respiratory distress.
Technique: radial artery puncture is the most common site; brachial and femoral arteries are alternatives. The sample must be processed within 15–30 minutes if kept at room temperature (or within 60 minutes if on ice). Heparin in the syringe prevents clotting. Avoid air bubbles (O₂ diffuses from air into sample, falsely elevating PaO₂).
ABG interpretation — systematic approach (5-step method):
1. Oxygenation: Is PaO₂ adequate? (<80 mmHg = hypoxaemia; <60 mmHg = significant hypoxaemia requiring intervention)
2. pH: Is it acidaemic (<7.35) or alkalaemic (>7.45) or normal?
3. Primary process: Is PaCO₂ elevated (>45 mmHg = respiratory acidosis) or reduced (<35 mmHg = respiratory alkalosis)? Is HCO₃⁻ elevated (>26 = metabolic alkalosis) or reduced (<22 = metabolic acidosis)?
4. Compensation: Does the compensation match the expected formula?
- Metabolic acidosis: expected PaCO₂ = 1.5 × HCO₃⁻ + 8 (±2) [Winter's formula]
- Respiratory acidosis (acute): HCO₃⁻ rises 1 mEq/L per 10 mmHg rise in PaCO₂
- Respiratory acidosis (chronic): HCO₃⁻ rises 3.5 mEq/L per 10 mmHg rise in PaCO₂ (elevated baseline HCO₃⁻ indicates chronicity)
5. Clinical correlation: does the ABG pattern fit the clinical presentation?
ABG patterns in obstructive airway disease:
| ABG Pattern | Clinical Scenario | Action |
|---|---|---|
| PaO₂ low, PaCO₂ low, pH high (resp. alkalosis) | Acute asthma, hypoxia-driven hyperventilation | O₂ supplement, treat asthma; hypocapnia = compensation working |
| PaO₂ low, PaCO₂ normal (38–42 mmHg), pH normal | Acute severe asthma with FATIGUE — DANGER | Escalate urgently; PaCO₂ should be low in acute asthma |
| PaO₂ low, PaCO₂ high, pH low (resp. acidosis) | Acute hypercapnic respiratory failure | NIV/intubation; type-2 respiratory failure |
| PaO₂ low, PaCO₂ high, pH near-normal, HCO₃⁻ elevated | Chronic CO₂ retention (compensated) | Controlled O₂, target SpO₂ 88–92% |
Chest Radiograph (CXR) in OAD:
Indications: all patients with acute exacerbation of OAD; initial COPD assessment; unexplained worsening of breathlessness; suspected complications (pneumothorax, pneumonia, cardiac failure); clinical features atypical of pure OAD.
Interpretation — systematic reading:
Always read the CXR systematically: (A) adequacy and orientation (penetration, rotation); (B) bony structures (rib fractures, vertebral changes); (C) cardiac outline (size, shape, borders); (D) diaphragm (level, flat or domed, costophrenic angles); (E) everything else (soft tissues, mediastinum, hila, lungs).
CXR findings in stable COPD:
- Hyperinflation: depressed flat diaphragms (below the anterior end of the 6th rib bilaterally), increased retrosternal airspace >3 cm (on lateral CXR), horizontal ribs, barrel-shaped thoracic cage
- Oligaemia (peripheral vascular attenuation): the lung periphery appears hyperlucent with sparse vascular markings — evidence of emphysema and loss of capillary bed
- Bullae: rounded thin-walled avascular areas; visible in bullous emphysema
- CXR in asthma (uncomplicated): usually normal; may show hyperinflation during an attack
CXR findings in acute complications:
- Pneumonia complicating exacerbation: lobar or segmental consolidation (airspace opacity with air bronchograms)
- Pneumothorax: visible pleural line (sharp white line at lung margin) with absent lung markings peripheral to it; tension pneumothorax shows mediastinal shift
- Pulmonary oedema (if cardiac failure coexists or is misdiagnosed): upper lobe venous diversion, Kerley B lines (fine horizontal lines at the periphery of the lower zones — interstitial oedema), perihilar haze, bilateral basal airspace opacities, cardiomegaly
- Lung cancer: hilar mass, peripheral nodule, pleural effusion — must not be missed in smokers presenting with 'COPD exacerbation'
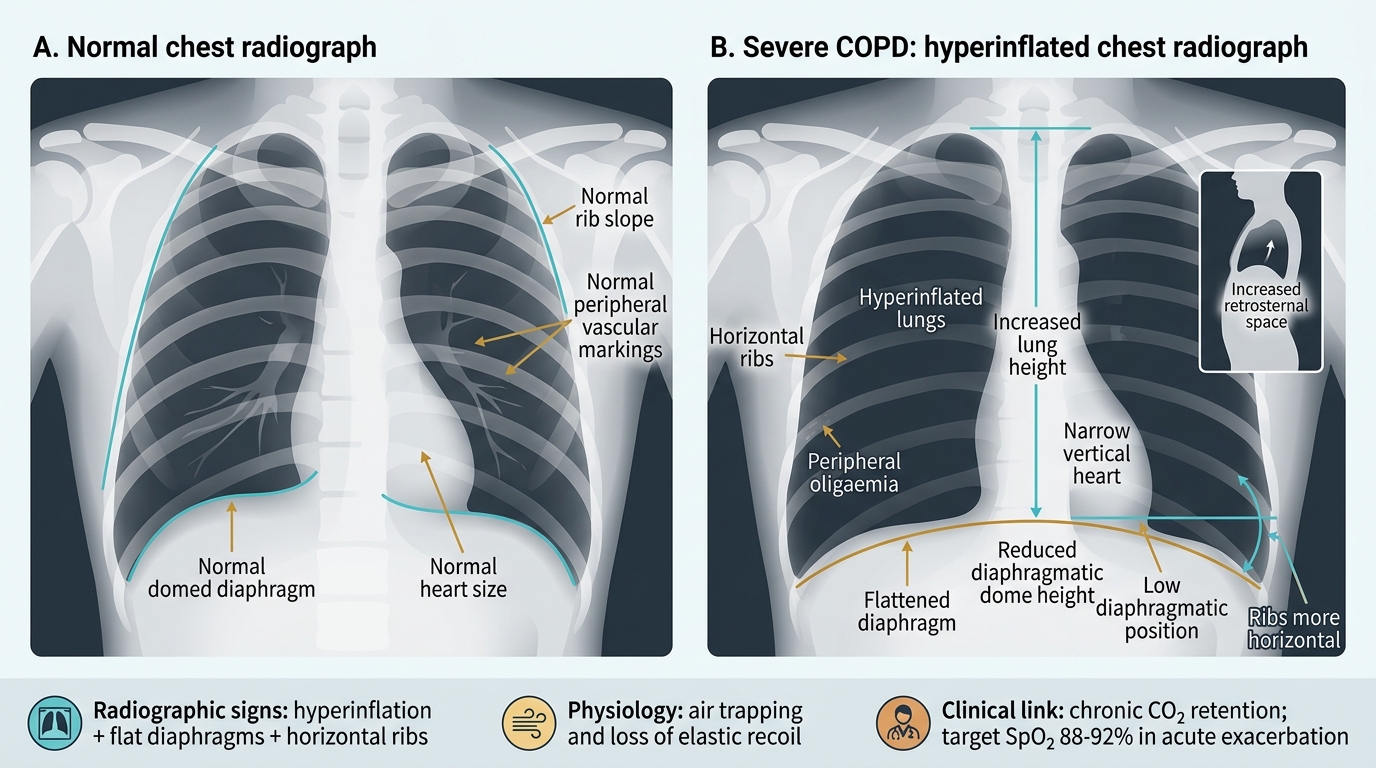
Chest Radiograph Signs of Severe COPD
SELF-CHECK
A 70-year-old COPD patient on LTOT at home is admitted with worsening breathlessness. His ABG on 2 L/min nasal O₂ shows: pH 7.29, PaO₂ 58 mmHg, PaCO₂ 72 mmHg, HCO₃⁻ 34 mEq/L, SpO₂ 88%. How should you interpret this ABG and what is the priority action?
A. Metabolic alkalosis from bicarbonate retention — reduce supplemental oxygen
B. Acute uncompensated respiratory acidosis — increase supplemental oxygen to improve SpO₂ to 94–98%
C. Acute-on-chronic respiratory acidosis — initiate NIV, target SpO₂ 88–92%, do NOT increase oxygen further
D. Mixed respiratory and metabolic acidosis — sodium bicarbonate infusion is indicated
Reveal Answer
Answer: C. Acute-on-chronic respiratory acidosis — initiate NIV, target SpO₂ 88–92%, do NOT increase oxygen further
pH 7.29 (acidosis), elevated PaCO₂ (72 mmHg, respiratory cause), elevated HCO₃⁻ (34 mEq/L — indicating chronic renal compensation, confirming chronic CO₂ retention), and low PaO₂ = acute-on-chronic hypercapnic respiratory failure (type-2). The elevated HCO₃⁻ indicates this patient is a known chronic CO₂ retainer — the safe SpO₂ target is 88–92%, NOT 94–98%. The appropriate intervention is NIV (BiPAP) to augment ventilation and reduce CO₂ retention. Increasing oxygen further would worsen hypercapnia by suppressing the hypoxic drive. Bicarbonate infusion worsens respiratory acidosis by removing the compensatory drive to breathe off CO₂.
Applied Practice: Integrating Investigations into Clinical Decision-Making
The investigations reviewed in this module do not exist in isolation — their value lies in their integration with the clinical context to drive management decisions. In practice, no single investigation result should be acted upon without being interpreted in light of the history, examination, and other investigations. This section consolidates the skill of investigation-directed clinical reasoning through a structured approach to common clinical scenarios.
Provided image
Case-based integration exercise:
Scenario A: A 38-year-old woman with known asthma is monitored in the outpatient clinic. She reports good control with her current ICS/SABA regimen. Her resting spirometry today shows FEV1/FVC 0.72, FEV1 88% predicted — both normal. PEFR diary for the past 4 weeks shows morning PEFR 340 L/min, evening PEFR 430 L/min on most days (diurnal variability = (430–340)/430 × 100 = 21%). Her skin prick tests show a 6 mm wheal to house dust mite.
Analysis: Normal resting spirometry between attacks is entirely consistent with mild asthma — FEV1/FVC returns to normal between episodes. The serial PEFR variability of 21% (>20% on most days) confirms significant variable airflow limitation consistent with asthma. The HDM sensitisation guides avoidance advice (mattress covers, reduce humidity, acaricidal sprays). This patient's asthma is clinically confirmed by PEFR variability even when spirometry is normal.
Scenario B: A 60-year-old male smoker (30 pack-years) presents with progressive breathlessness. Spirometry post-bronchodilator: FEV1/FVC 0.61, FEV1 57% predicted. CXR shows bilateral hyperinflation, flat diaphragms, and a 2 cm nodule in the right upper lobe. SpO₂ 93% at rest on room air.
Analysis: FEV1/FVC 0.61 and FEV1 57% = GOLD 2 COPD (moderate). However, the right upper lobe nodule on CXR in a 30 pack-year smoker is highly suspicious for primary lung carcinoma (squamous cell carcinoma is commonest in upper lobes). This nodule requires urgent CT chest with contrast for characterisation and staging — it must not be attributed to COPD without exclusion of malignancy. SpO₂ 93% on room air: not yet at the LTOT threshold (≤88% or ≤92% with cor pulmonale) but warrants ABG for baseline documentation.
Scenario C: A 25-year-old woman is brought to emergency with acute severe asthma. On admission: PEFR 42% personal best, RR 26/min, SpO₂ 94% on 6 L/min O₂ via mask. After 1 hour of intensive bronchodilator therapy (three back-to-back nebulisations), PEFR has risen to 55% personal best, RR 22/min. A repeat ABG shows PaCO₂ 44 mmHg. Is she improving or deteriorating?
Analysis: PEFR is rising (42% → 55%) and RR is falling — these suggest improvement. But the PaCO₂ of 44 mmHg demands urgent attention: in a 25-year-old asthmatic on 6 L/min O₂ who is still tachypnoeic (RR 22/min), PaCO₂ should be 30–35 mmHg due to hyperventilation. A PaCO₂ of 44 mmHg is within the 'normal' laboratory range but represents significant ventilatory fatigue in this context — it is a near-fatal marker. PEFR is still <66% personal best. This patient is not safe for discharge and should remain in hospital with repeat ABG in 30–60 minutes.
Key Investigation Findings in Obstructive Airway Disease
SELF-CHECK
A 50-year-old male smoker has spirometry showing FEV1/FVC 0.58 pre-bronchodilator and 0.61 post-bronchodilator, with FEV1 rising from 1.68 L to 1.83 L after salbutamol (a 9% rise, 150 mL improvement). Which statement correctly interprets this result?
A. Significant bronchodilator reversibility — consistent with asthma (≥12% improvement present)
B. No significant bronchodilator reversibility — persistent obstruction consistent with COPD
C. The post-bronchodilator FEV1/FVC of 0.61 confirms restriction, not obstruction
D. A 150 mL improvement alone is sufficient to confirm reversibility regardless of percentage
Reveal Answer
Answer: B. No significant bronchodilator reversibility — persistent obstruction consistent with COPD
Significant bronchodilator reversibility requires BOTH criteria to be met simultaneously: ≥12% improvement AND ≥200 mL absolute improvement in FEV1. This patient has a 9% improvement (below 12%) AND only 150 mL improvement (below 200 mL) — neither threshold is met individually, and therefore this does NOT constitute significant reversibility. The post-bronchodilator FEV1/FVC of 0.61 (below 0.70) with a 50-year-old smoker and no significant reversibility confirms GOLD-criterion COPD. A post-bronchodilator FEV1/FVC below 0.70 is obstruction, not restriction (restriction requires reduced FVC with preserved or elevated ratio).
CLINICAL PEARL
Three investigation traps that every final-year student must know: First, a normal spirometry result does not exclude asthma — spirometry is normal between attacks in mild-moderate asthma; serial PEFR variability (>20% diurnal change) or bronchial provocation testing is required to confirm the diagnosis in these patients. Second, a normal PaCO₂ is not reassuring in acute severe asthma — in a hyperventilating asthmatic, PaCO₂ should be low (30–35 mmHg); a 'normal' value of 40 mmHg signals ventilatory fatigue and impending respiratory arrest. Third, the chest radiograph in acute asthma is normal in the majority of cases — its main role is to exclude complications (pneumothorax, pneumonia, pneumomediastinum) and alternative diagnoses, not to confirm asthma.
Self-Assessment: Interpreting Investigations
Test your ability to interpret the investigations reviewed in this module through the following structured vignettes. For each, identify the key abnormality, its clinical significance, and the immediate management implication.
Vignette 1: Spirometry results: FEV1 pre-BD 1.42 L (60% predicted), FVC pre-BD 1.95 L, FEV1/FVC pre-BD 0.73. Post-bronchodilator: FEV1 1.85 L (78% predicted), FVC 2.10 L, FEV1/FVC 0.88. Patient is a 28-year-old woman with episodic nocturnal wheeze. What is the diagnosis and the key spirometric criterion?
Analysis: Pre-bronchodilator FEV1/FVC of 0.73 = borderline/normal (>0.70). Post-bronchodilator: FEV1 rises from 1.42 to 1.85 L = 430 mL improvement = 30% improvement — both the ≥12% AND ≥200 mL criteria are met. Significant bronchodilator reversibility confirms variable airflow limitation consistent with asthma. The pre-BD ratio of 0.73 (just above 0.70) does not rule out asthma — in early or mild asthma the resting obstruction may be mild. The reversibility criterion is the diagnostic key.
Vignette 2: CXR report: 'Right costophrenic angle blunting with a horizontal upper border; mediastinum central; left lung clear; heart size normal.' ABG: pH 7.36, PaO₂ 68 mmHg, PaCO₂ 42 mmHg, HCO₃⁻ 23 mEq/L. PEFR 310 L/min (personal best 490 L/min). Patient has asthma and was admitted with acute breathlessness after a chest infection.
Analysis: CXR shows right pleural effusion (blunted costophrenic angle, horizontal upper border). ABG: pH 7.36 (normal), PaO₂ 68 mmHg (hypoxaemia — type-1 respiratory failure: low O₂, normal CO₂), normal HCO₃⁻ = no chronic compensation. PEFR 310/490 = 63% personal best = severe asthma territory but also significantly impaired by the coexisting pleural process. The effusion requires diagnostic aspiration (parapneumonic effusion vs empyema vs malignancy). The type-1 respiratory failure requires supplemental O₂ targeting SpO₂ 94–98%.
Vignette 3: A 65-year-old COPD patient has the following spirometry: post-bronchodilator FEV1 0.98 L (28% predicted), FVC 3.12 L, FEV1/FVC 0.31. What GOLD grade is this, and what does it imply for management?
Analysis: FEV1/FVC 0.31 (< 0.70) = obstruction confirmed. FEV1 28% predicted (< 30%) = GOLD 4 Very Severe COPD. This patient requires: maximum inhaler therapy (LAMA + LABA ± ICS), assessment for LTOT (if SpO₂ ≤88% or PaO₂ ≤55 mmHg), pulmonary rehabilitation, nutritional support, assessment for comorbidities (lung cancer, cardiac failure, depression), advance care planning discussion, and assessment for surgical options (lung volume reduction surgery, bullectomy, or lung transplantation referral in selected cases).
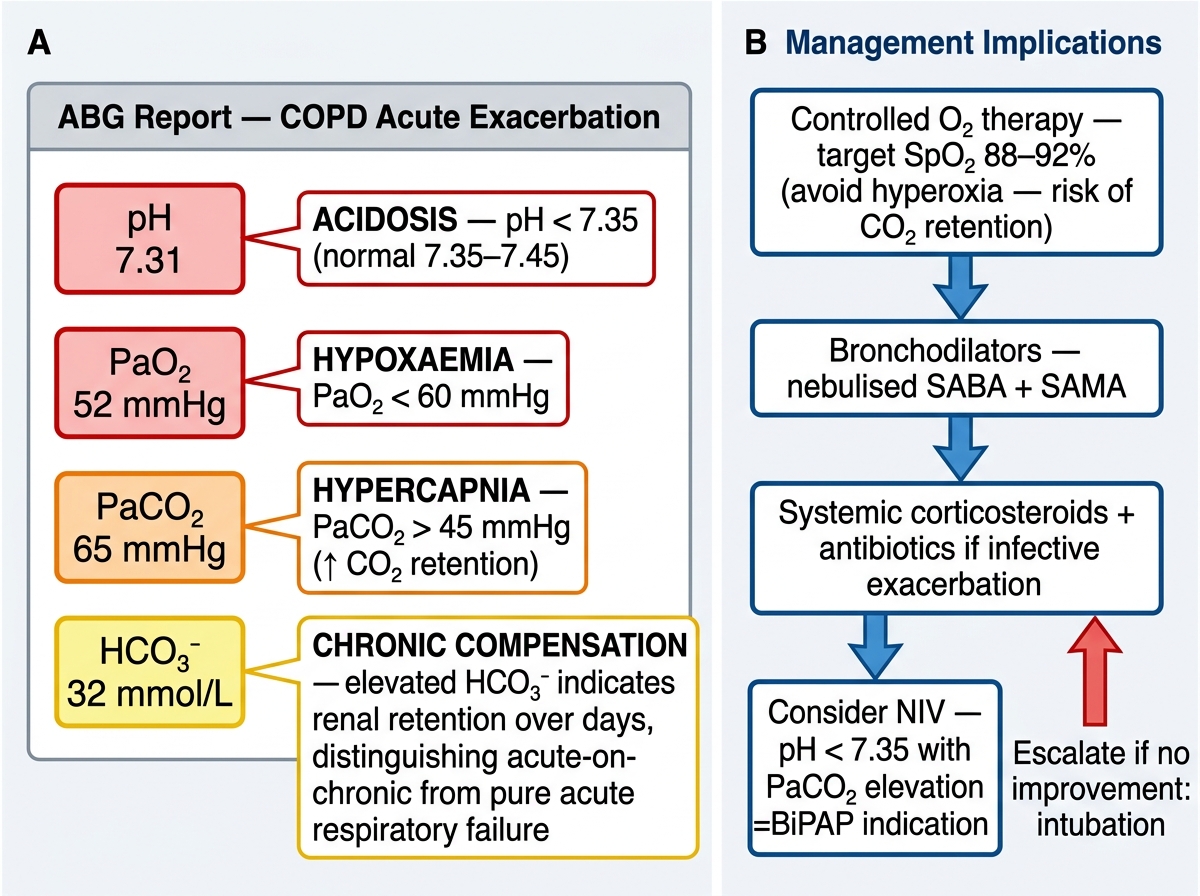
Annotated ABG Interpretation — COPD Acute Exacerbation